

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Polyunsaturated fatty acids (PUFAs) are categorized as n-6 PUFA and n-3 PUFA [1]. Long-chain n-3 PUFAs serve as precursors for endocannabinoids, oxylipins, and eicosanoids, which are important regulators of adipogenesis, inflammation, insulin action, and neurological function (Fig. 1) [2]. Since n-3 PUFA and n-6 PUFAs compete for enzymes responsible for the production of long-chain n-3 PUFAs, their balance influences the production of eicosanoids and oxylipins [3].
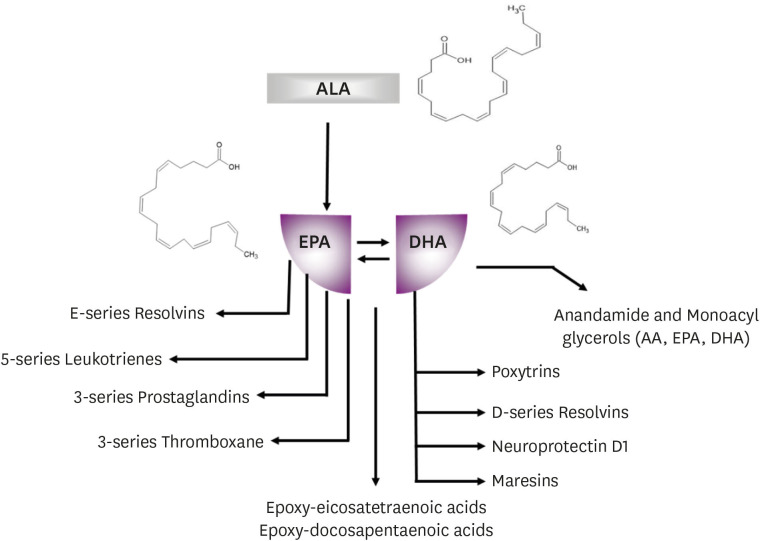
Among the n-3 PUFAs, alpha-linolenic acid (ALA; 18:3n3) is an essential fatty acid which cannot be synthesized in humans, and must therefore be obtained through diet [14]. Thus, a lack of ALA in the diet results in clinical symptoms of deficiency, such as scaly dermatitis and reduced growth [5]. In addition, ALA acts as a precursor for the long-chain n-3 PUFAs, eicosapentaenoic acid (EPA; 20:5n3) and docosahexaenoic acid (DHA; 22:6n3), through elongation and desaturation [6]. The major food sources for EPA and DHA are fatty fish, fish oils, and products fortified with fish oils, which help reduce the risk of cardiovascular disease (CVD) [7].
Because of their cardioprotective effects, dietary recommendations for EPA, DHA, and ALA have been issued globally. Due to limited evidence, Korea set a Dietary Reference Intake (DRI) for n-3 PUFA for the first time in 2020 [8]. This paper describes the process and evidence used to create the DRI of ALA and EPA + DHA for Koreans.
Go to : 
DIETARY RECOMMENDATION OF N-3 PUFA FOR KOREANS
Dietary recommendation of n-3 PUFA for children and adults
To estimate the average requirement (EAR) and recommend the nutrient intake (RNI) for n-3 PUFA, data are required to determine a defined intake level at which risk of inadequacy or prevention of chronic disease occurs [9]. However, there is no convincing evidence that deficiency symptoms of n-3 PUFAs (ALA, EPA, and DHA) are absent, or that the deficiency exerts detrimental effects in healthy individuals. Thus, due to lack of evidence for determining the minimal requirement in healthy individuals, the EAR and RNI could not be established.
Due to inadequacy of scientific basis to compute EAR and RNI, adequate intake (AI) is sufficient to maintain a satisfactory nutritional status of a particular sex and age group [9]. AL is generally based on epidemiological studies that estimate the nutritional intake of healthy individuals [9]. For the first time, the average intake of n-3 PUFA for Koreans was obtained in the 2013–2017 Korea National Health and Nutrition Examination Survey (KNHANES) for individuals aged 1 yr and older [8]. The AI of n-3 PUFA for Koreans was established using the distribution of dietary intake based on KNHANES. The average intakes of ALA and EPA + DHA in Koreans aged 1 yr and older were determined to be 1.27 g/day and 279 mg/day, respectively (Tables 1 and 2). The AIs for ALA are based on the average intake of ALA according to the different life stages and sex groups with no reported ALA deficiencies in healthy individuals (Table 3) [8]. The AIs for EPA + DHA are also based on the average intake of EPA + DHA in Koreans aged 6 yrs and older; the function of EPA and DHA intake is not to prevent deficiency, but to lower the risk of chronic diseases, particularly CVD. The currently available evidence does not permit the definition of an age-specific quantitative estimate of adequate dietary intake for EPA and DHA for children under 6 yrs of age. However, general dietary advice for children should be consistent with advice for the adult population, comprising 1 to 2 fatty fish meals per week [10].
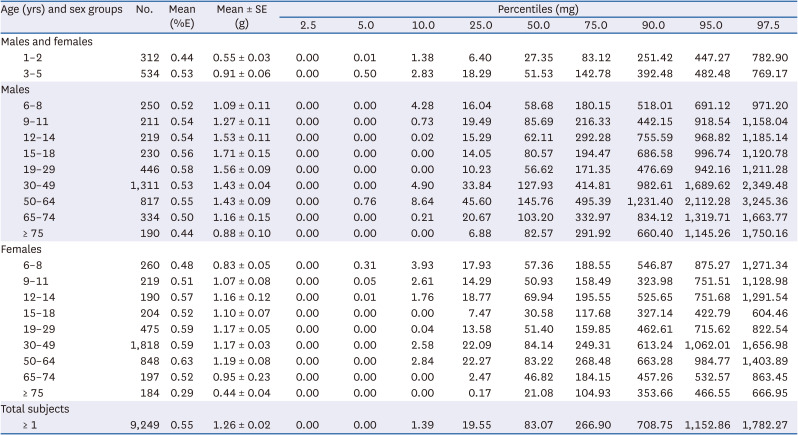
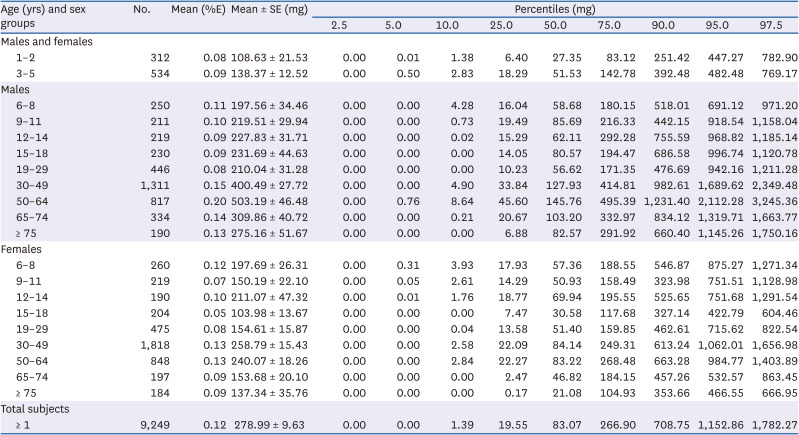
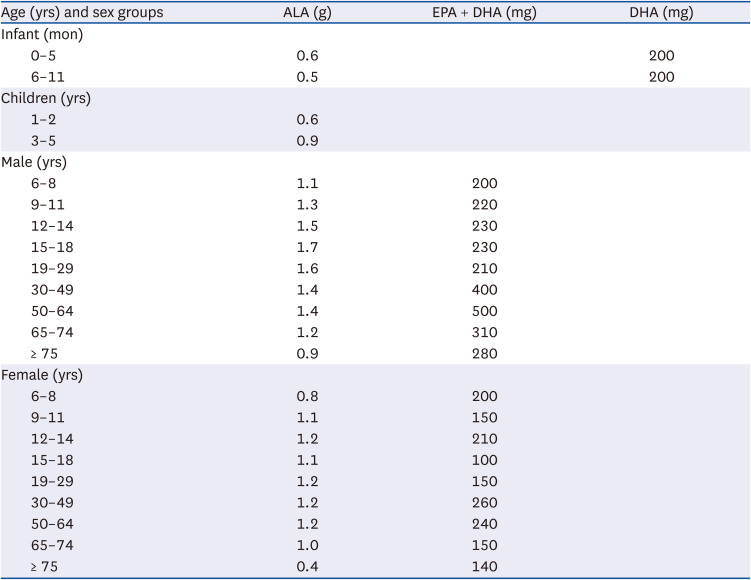
Table 1
Distribution of dietary alpha-linolenic acid intake based on Korea National Health and Nutrition Examination Survey 2013–2017
![]()
Table 2
Distribution of dietary eicosapentaenoic acid and docosahexaenoic acid intake based on Korea National Health and Nutrition Examination Survey 2013–2017
![]()
Table 3
Adequate intake of n-3 polyunsaturated fatty acids from 2020 Korean dietary reference intakes1)
ALA, alpha-linolenic acid; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid.
1)Ministry of Health and Welfare 2020 [8].
![]()
Dietary recommendation of n-3 PUFA for infants
Establishment of the AIs were based on the observed average intake of ALA and DHA for infants aged 0–12 mon who were principally fed maternal milk. DHA is essential during early development as it plays a critical role in normal brain and retinal development. However, the conversion of DHA from ALA is limited and highly variable in infants [11]. To compensate for oxidative losses of maternal dietary DHA, and accumulation of DHA in the body fat of the fetus/infant, the minimum intake of DHA for pregnant or lactating women is recommended at 200 mg/day [11]. The European Food Safety Authority (EFSA) suggested that DHA intakes of 50 to 100 mg/day are effective for visual function during the complementary feeding period, and are adequate levels for older infants [11].
Human milk is the preferred infant food and a source of DHA, but levels of DHA are variable and dependent on the maternal diet [11]. Thus, the content of DHA in human milk can serve to define the AI of DHA for infants [11]. Since 0.78 L/day is the reported mean quantity of human milk consumed by an infant aged 0 through 5 mon, the standard quantity to be consumed by a healthy infant has been established as 0.78 L/day [121314151617]. For infants aged 6–11 mon, consumption of food other than human milk (or other milk products prepared for infants) also needs to be considered. However, due to insufficient valid and accurate data for Koreans [1618], extrapolated values for infants aged 0–5 mon were used for infants aged 6–11 mon. Levels of ALA and DHA in Korean maternal milk have been reported as 772.50 mg/L and 298.71 mg/L, respectively, during the first 5 mon [19]. Thus, the AI for an infant aged 0 through 5 mon is estimated at 600 mg/day ALA (772.50 mg/L × 0.78 L/day = 602.55 mg/day ≒ 600 mg/day) and 200 mg/day DHA (298.71 mg/L × 0.78 L/day = 232.99 mg/day ≒ 200 mg/day) [8]. For infants aged 6 through 11 mon, estimation of AI is based on the AI for infants aged 0–5 mon and the metabolic weight: 800 mg/day ALA (600 mg/L × (8.4/5.5)0.75 = 820 mg/day ≒ 800 mg/day) and 300 mg/day DHA (200 mg/L × (8.4/5.5)0.75 = 274.77 mg/day ≒ 300 mg/day) [8].
Dietary recommendation of n-3 PUFA for pregnant and lactating women
The AIs of n-3 PUFA for non-pregnant and non-lactating women were computed for their specific age category in Korea, with no additional requirement for pregnancy and lactation. The EFSA added 100 to 200 mg DHA during pregnancy and lactation to compensate for oxidative losses of maternal dietary DHA and accumulation of DHA in the body fat of the fetus/infant [20]. However, since levels of DHA obtained in Korean maternal milk were high, and infant consumption of DHA is estimated to be 200–300 mg/day, the AI of DHA was set for EFSA. Furthermore, the National Health and Nutrition Examination Survey (1999–2000) for the US population (including all ages and both sexes) reported the mean intake of EPA and DHA to be about 100 mg/day [21]. Stark et al. [22] reported that the blood levels of EPA and DHA (the biomarkers for dietary intake of n-3 PUFA) were higher than 8% in Koreans, whereas levels obtained were ≤ 4% in Americans and 4–6% in most Europeans. This indicates that Korean women consume more fish than American or European women, thereby eliminating the need for additional intake of DHA for pregnant or lactating Korean women.
Upper intake level (UL) of n-3 PUFA
A high intake of n-3 PUFA results in increased lipid peroxidation and prolongs the bleeding time, particularly in people taking anticoagulants, including aspirin and warfarin [11]. However, higher consumption levels (as high as 3 g/day), reduce other cardiovascular risk factors with no reported adverse effects in short- and intermediate-term randomized trials [1020]. In addition, some individuals in populations with high seafood consumption show no apparent adverse effects [1020]. Hence, the US Food and Drug Administration has set a “Generally Regarded as Safe” level of 3 g/day for EPA and DHA.
There is concern regarding certain species of large fish that are a major source of methylmercury, which may induce neurotoxic effects on the fetus and reduce cognition in young people [2324]. However, 2 large prospective cohorts reported that the concentrations of mercury obtained in toenails of subjects were not associated with the risk of hypertension or CVD [2526]. In addition, a 0.5% increase in blood n-3 PUFA was associated with a 23% lower risk of sudden cardiac death among Finnish men, with no significant difference in men with high mercury levels in hair [27]. The existing evidence supports that the benefits of fish on the CVD endpoint, especially consumption of a certain variety of seafood, outweigh the unfavorable risks of mercury in fish. Thus, currently, there is sufficient evidence to set an UL for n-3 PUFA in Korea. Future randomized controlled trials (RCTs) and other studies are required to set the UL.
Go to :
INTERNATIONAL RECOMMENDATION FOR DIETARY N-3 PUFA
Various global organizations have suggested dietary recommendations for n-3 PUFA, including ALA, EPA, and DHA, mainly for reducing the risk of CVD and hypertriglyceridemia (Table 4) [42028]. Additionally, recommendations for DHA intake have been made for infants. The Institute of Medicine (IOM) of the National Academies has set an AI for ALA based on an intake that supports normal growth and neural development, with no nutrient deficiency. Although IOM of the National Academies had no DRI for EPA and DHA, the recommended macronutrient distribution range for n-3 PUFA is 0.1–0.2%. The American Heart Association, American Dietetic Association, and Dietitians of Canada recommend 500 mg/day EPA + DHA provided by 2 servings of fatty fish/week (1 serving is 112 g cooked) [10]. The Food and Agriculture Organization (2010) recommends 200 mg/day DHA or 300 mg/day DHA + EPA, and the World Health Organization recommends regular fish consumption (1 to 2 servings per week; each serving should provide an equivalent of 200–500 mg EPA + DHA) [11].
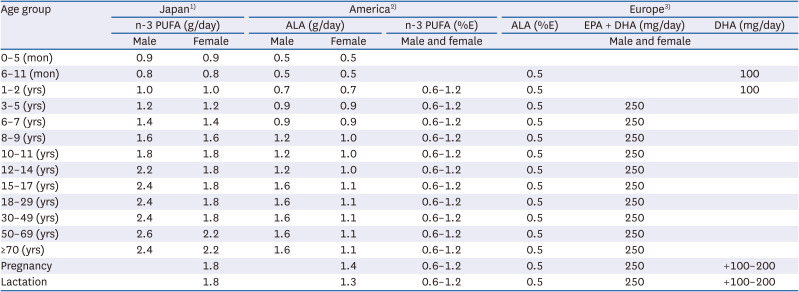
Table 4
Dietary recommendation of n-3 PUFAs in Japan, America, and Europe
PUFA, polyunsaturated fatty acid; ALA, alpha-linolenic acid; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid.
1)Ministry of Health, Labor, and Welfare of Japan 2020 [28].
2)Institute of Medicine 2005 [4].
3)European Food Safety Authority 2017 [20].
![]()
The EFSA proposes to set an AI for ALA of 0.5%E, based on the lowest estimated mean intakes of various population groups from numerous European countries, where overt deficiency symptoms of ALA are absent (Table 4) [20]. Based on cardiovascular considerations, the EFSA recommends an AI of 250 mg EPA + DHA for adults. When considering CVD, prospective epidemiological and dietary intervention studies indicate that oily fish consumption or dietary n-3 long-chain PUFA supplements (equivalent to 250 to 500 mg/day EPA + DHA) decreases the risk of mortality from CVD and sudden cardiac death. In infants, DHA intakes of 50 to 100 mg/day are found to be effective for visual function and considered to be adequate in the complementary feeding period. Thus, EFSA proposes an AI of 100 mg DHA for infants (> 6 mon of age) and young children below the age of 24 mon (Table 4).
In Japan, the AI of n-3 PUFA was established on the median intake determined from epidemiological studies that estimated the intake of healthy individuals [28]. For infants, AI was computed on the n-3 PUFA concentration present in human milk, and the amount consumed by the infant was used for calculation.
There is no convincing evidence that high intakes of ALA and n-3 PUFA have detrimental effects on health [420]. Supplemental intake of EPA and DHA combined at doses up to 5 g/day, supplemental intake of EPA alone up to 1.8 g/day, and supplemental intake of DHA up to 1,000 mg/day do not raise safety concerns for adults [11]. Thus, no global dietary recommendation is set for the UL of n-3 PUFA.
Go to :
EFFECT OF N-3 PUFA ON CVD
N-3 PUFA is known to exert cardioprotective effects via antiarrhythmic, anti-inflammatory, hematologic, and endothelial mechanisms [29]. In multiple prospective cohort studies, including the Physicians’ Health Study, a significant association was obtained between the dietary intake of n-3 PUFA and a lower risk of fatal CVD events, especially sudden cardiac death [3031323334].
In particular, a dose-dependent association was observed between very low to moderate intake and lower risk of sudden cardiac death, thereby indicating that consuming 1 to 2 fatty fish meals per week is associated with a 50% lower risk of sudden cardiac death, as compared with little or no seafood intake [3233]. In contrast, intake of n-3 PUFA was not found to be associated with a lower risk of sudden cardiac death in the Japanese population [3536]. Interestingly, the dietary intake of fish among Japanese was 3 to 4 times higher than most Western countries, and similar to the Korean consumption [37]. Current evidence suggests that the association between long-chain n-3 PUFA from seafood and the risk of sudden cardiac death may be not linear, but a modest consumption of seafood (1–2 servings per week) may be better, compared with little or no seafood intake.
Clinical trials have presented the benefits of both fish and n-3 PUFA supplements in CVD. The Diet and Reinfarction Trial reported that fish (or fish oil) consumption significantly reduces all-cause mortality and CVD in men who had recovered from a myocardial infarct [38]. The Gruppo Italiano per la Sperimentazione della Strepto-chinasi nell’Infarto Miocardico trial enrolled patients who had survived a myocardial infarct. They reported that supplementation of approximately 867 mg/day EPA + DHA (1:2 ratio, or about 289 mg EPA and 578 mg DHA) reduces the risk for CVD by 11–20%, and a 47% decrease in sudden cardiac death [39]. In the prospective randomized open-label trial of the Japan EPA Lipid Intervention Study, supplementation with 1,800 mg/day EPA resulted in a 19% relative reduction in major coronary events in patients who were taking statins [40]. Two very recent trials also reported some benefits of n-3 PUFA supplementation in high-risk patients. The REDUCE-IT trial involved patients with established CVD or with diabetes and other risk factors who were taking statins. They found that 4 g/day EPA lowered the risk of ischemic events, including cardiovascular death among patients with elevated TG levels despite the use of statins [41]. However, the STRENGTH trial determined the impact of 4 g/day EPA + DHA in patients receiving statins with mildly elevated triglyceride levels, and found no significant effect on major adverse cardiac events, including cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, coronary revascularization, and unstable angina requiring hospitalization [42].
As a rule, subjects to whom the DRI is applied are healthy individuals or groups of healthy individuals, but the previous randomized clinical trials included only at risk of CVD and CVD populations. The VITAL trial is a study for the primary prevention of CVD in men aged 50 yrs or older and women aged 55 yrs or older in the US [43]. This study reported that supplementation of 1 g/day EPA + DHA did not affect a lower incidence of major cardiovascular events, but significantly reduced death from myocardial infarction and total CVD. Since there is insufficient evidence demonstrating the effect of n-3 PUFA on clinical CVD outcomes, particularly in healthy populations, dietary guidelines of n-3 PUFA for disease reduction cannot be recommended.
Go to :
CONCLUSION
Global organizations have suggested dietary recommendations for n-3 PUFA, including ALA, EPA, or DHA, for the prevention of deficiency and reducing the risk of CVD. Based on the national health and nutrition survey, the AI for ALA and EPA + DHA were established for the first time for Koreans aged 1 yr and older. For Korean infants aged 0–11 mon, AI was based on the observed human maternal milk content of ALA and DHA. Future RCTs and other research on n-3 PUFA are required to establish the EAR, RNI, and recommendations for disease reduction, particularly for the healthy Korean population.
Go to :
 XML Download
XML Download