

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Isoflavone is one of the subclasses of dietary flavonoids, which is the major group of polyphenolic compounds predominantly present in plant-based foods [12]. Soy and soy products are the predominant dietary sources of isoflavones [3]. The amount of isoflavones in soy varies according to the cultivar, cultivation conditions, and post-harvest processing [45]. The isoflavone content ranges from 580 to 3,800 mg/kg fresh weight and 1.2 to 4.2 mg/g dry weight in soybean (primarily in the structure of daidzein, genistein, and their conjugates) [36]. The isoflavone levels in soy milk have been reported to range between 30 and 175 mg/L [3]. Isoflavones are also present in legumes (e.g., chickpeas and lentils), nuts, vegetables, and fruits [7].
Isoflavones act as phytoestrogens because they have a chemical structure similar to estrogen. Isoflavone glycosides include the following: daidzin, genistin, glycitin, ononin, issotrin, acetyldaidzin, acetylgenistin, acetylglycitin, malonyldaidzin, malonylgenistin, malonylglycitin, malonylononin, and malonylsissotrin. Isoflavone aglycones include genistein (7,4′-dihydroxy-6-methoxyisoflavone), daidzein (7,4′-dihydroxyisoflavone), glycitein (7,4′-dihydroxy-6-methoxyisoflavone), biochanin A (5,7-dihydroxy-4′-methoxyisoflavone), and formononetin (7-hydroxy-4′-methoxyisoflavone) [8]. Isoflavone aglycones are the active forms hydrolyzed from glycosides, which are inactive forms of isoflavone [89]. In particular, daidzin and daidzein (soy isoflavone) are metabolized to equol (7-hydroxy-3-[4′-hydroxyphenyl] chroman) by the action of intestinal microflora [1011]. Equol has been suggested to have beneficial effects on human health [10].
Epidemiological and intervention studies have reported that the consumption of soy or isoflavone is inversely associated with the risk of type 2 diabetes mellitus (T2DM) [12], cardiovascular disease (CVD) [1314], cerebral and myocardial infarctions (CI and MI) [15], bone loss [1617], cognitive degeneration [1819], gastrointestinal cancer [20], colorectal cancer [21], prostate cancer [22], breast cancer [2324], and menopausal symptoms [25]. A meta-analysis of six prospective studies with 4 publications showed that the highest intake (60 mg/d) of soy isoflavone was associated with a 12% lower risk of T2DM compared to the lowest intake of soy isoflavone (relative risk = 0.88; 95% confidence interval, 0.81 to 0.96; I2 = 37.2%) [12]. In a meta-analysis of 63 randomized controlled trials (RCTs) in 6,427 postmenopausal women, the intake of genistein (54 mg/d) or ipriflavone (600 mg/d) was associated with improved bone mineral density (BMD) [16].
Despite the beneficial effects of dietary intake of isoflavone on T2DM, CVD, osteoporosis, cognitive function, and cancers [12151618222426], there are still concerns about isoflavone intake as a potential endocrine disruptor with adverse effects on growth, fertility, and the reproductive and endocrine systems at certain human life stages [27]. According to the USA National Toxicology Program (USA-NTP), adverse doses of fertility were reported to be 0.1 mg/(kg body weight × days) in children and 0.3 mg/(kg body weight × days) in adults depending on the individual’s susceptibility [28]. Infants fed soy milk or formula at ≤ 4 mon showed higher Pre-School Activities Inventory (PSAI) scores (less female-typical role play) in girls compared with infants fed breast milk and milk formula [29]. Girls with precocious puberty had a significant level of serum isoflavone [30].
An accurate estimation of the dietary isoflavone intake based on gender and age is critical when considering the beneficial and harmful aspects of isoflavone for public health [2731]. The estimation of the total isoflavone intake and major food sources has been conducted in several countries, including Japan [3233], China [32], Hong Kong [3234], Singapore [32], the USA [3536], the UK [373839], Australia [40], Spain [41], Ireland [39], Italy [39], and the Netherlands [39]. Adults in the USA, the UK, Australia, Spain, Ireland, Italy, and the Netherlands aged ≥ 19 yrs consumed less than 3 mg/d of isoflavone [353637394041]. Adults (aged ≥ 19 yrs) in Japan showed a daily isoflavone intake of 25 to 50 mg. Hong Kong and Singaporean adults showed lower isoflavone intakes than Chinese adults [32]. The major food sources of isoflavone are soy products, followed by legumes in those countries [32353637394041].
Although a few studies on the estimation of dietary isoflavone intake and major food sources in Korea have been conducted, they focused on a certain age group of the Korean population [42434445]. Thus, the research on the usual dietary intake and major food sources of isoflavones based on a representative Korean population is still required to reflect the differences across age groups. This study examined the usual total isoflavone intake and explored major food sources for different age and sex groups in the Korean population using Korea National Health and Nutrition Examination Survey VII (KNHANES VII) data.
Go to : 
SUBJECTS AND METHODS
Database for calculation of usual intake and subjects
The KNHANES is a large, representative, nationwide cross-sectional health and nutrition survey conducted for Koreans aged 1 yrs or older living in Korea. Further details of KNHANES can be found elsewhere [44]. The KNHANES consists of a health interview survey, a nutrition survey, and a health examination survey. A 2-step stratified cluster sampling method was applied in KNHANES to ensure a representative sample and estimation accuracy. Detailed investigation methods and protocols have been addressed in previous studies [4647]. A multiple-pass 24-h dietary recall method and the relative frequency weighting of each food were used to estimate the usual total isoflavone intake in the KNHANES [48]. At least 2 days of dietary data are required to estimate the usual of total isoflavone intake. On the other hand, because the KNAHNES basically provides only one-day data for each individual except for KNHANES 2009, this study calculated the ratio of the within- and between-participants variance of the 7th KNHANES (2016, 2017, and 2018) data based on the 2009 KNHANES data. It estimated the usual isoflavone intake using the 2016, 2017, and 2018 KNHANES data.
The 24-h dietary recall method in the 2009 KNHANES was performed with an additional one day in 50 out of 200 surveys (n = 9,391). Through this process, two-day intake data were generated from 2,029 of the total subjects, which was the most recent data consisting of two days of a 24-h dietary recall method available thus far. Thus, this study calculated the ratio of within-person to between-person variance in isoflavone intake from the 2009 KNAHNES data. The usual isoflavone intake was estimated by applying the ratio to the 24-h dietary recall data of the 7th KNAHNES data (n = 21,271) conducted in 2016, 2017, and 2018.
Dietary assessment
The isoflavone intake was calculated mainly based on the ‘isoflavone database’ developed by the Korea Rural Development Administration (RDA) in 2018. The isoflavone content (mg/100 g) of 268 food items was released, and the isoflavone content was calculated from genistein, daidzein, glycitein, biochanin A, formononetin, isomucronulatol, methylnissolin, 3′-hydroxydaidzein, 3′-methoxydaidzein, calycosin, and odoratin. The information on the isoflavone content from 142 food items provided in Park’s thesis [49] and data on isoflavone content from 560 food items in the U.S. Department of Agriculture database (Release 2.0) were also used to increase the coverage of the database [50]. The food intake data with food code (N_FCODE3) was used in the dataset. The food intake amount was calculated by linking each food code with the isoflavone content database, where KNHANES has the unique food code system used as the primary code. The isoflavone intake was calculated for each food based on the isoflavone contents when identified as a similar food after examining the moisture content and properties of the food. The linkage process was first performed using the 2009 KNHANES to calculate isoflavone intake for 4 yrs and then relinked with the food code of the 7th KNHANES. After matching, as isoflavone content is not zero, 266 food codes in the KNHANES were used in this linkage process. For the ‘cereals’ food group, bread and rice cakes were the main foods in the DB for the isoflavone content, while soybeans, peas, kidney beans, tofu, and arrowroot were the main foods in the ‘legumes’ food group. Peanuts in the ‘nuts and seeds’ food group and bean sprouts and mungbean sprouts in the ‘vegetables’ food group had relatively high isoflavone contents. This study’s database also included peanut butter from the ‘fats and oils’ food group, as well as gochujang, soybean paste, and ssamjang from the ‘seasonings’ food group.
Statistical analysis
The National Cancer Institute (NCI) one-day method was applied to estimate the usual isoflavone intake. The intake data for more than 2 days are required for some subjects in the target group to use the existing NCI method. The basic principle of the NCI 1-d method is the same as that of the NCI method. The NCI 1-d method calculates the within-person to between-person variance ratio from intakes for two days or more in a group other than the same group and then applies it to the target group. Ultimately, the daily intake of the target group can be estimated.
Therefore, this study calculated the variance ratio of the isoflavone intake from the intake data for 2 days in the 2009 KNHANES through the MIXTRAN macro and applied it to the 3-yrs data of the 7th KNHANES (TRAN-1 macro). The estimated daily total isoflavone intake is presented with the mean, SE, and 9 percentiles (1st, 5th, 10th, 25th, 50th, 75th, 90th, 95th, and 99th). All statistical analyses were carried out using Statistical Analysis System (SAS version 9.4; SAS Institute, Cary, NC, USA). The SAS survey procedures and the appropriate weight, strata, and cluster variables were applied to account for the complex survey design of the KNHANES.
Go to :
RESULTS
Isoflavone contents of food groups and contribution rates of each food source
Table 1 lists the isoflavone contents of 15 food groups according to the food code classification system. The legumes group had the highest isoflavone content (615.50 mg), followed by seasonings (90.41 mg), sugars (41.28 mg), and processed foods (25.36 mg). The contribution of the legumes food group to the daily isoflavone intake in the 7th KNHANES was the highest (90.99%). In comparison, the contribution rates of the vegetables and seasonings food groups were 5.56% and 2.13%, respectively (Table 1).
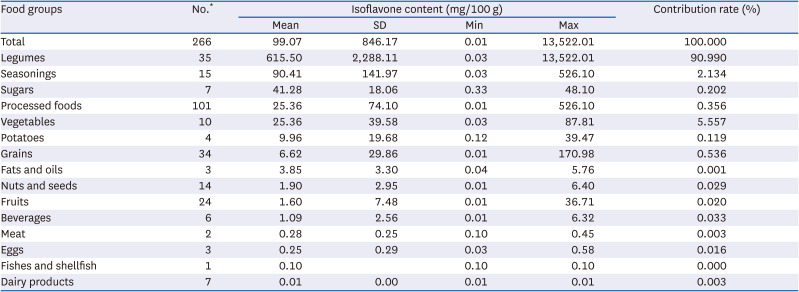
Table 1
Database for the isoflavone content of the selected food groups and percentage contribution for each food group (KNHANES VII)
KNHANES, Korea National Health and Nutrition Examination Survey
*Number of individual foods in each food group.
![]()
Table 2 lists the contribution rates of individual food sources of isoflavone. The highest contribution rate to isoflavone intake was 67.16% for arrowroot, 21.25% for soybean, 5.44% for bean sprouts, and 2.10% for tofu (Table 2).
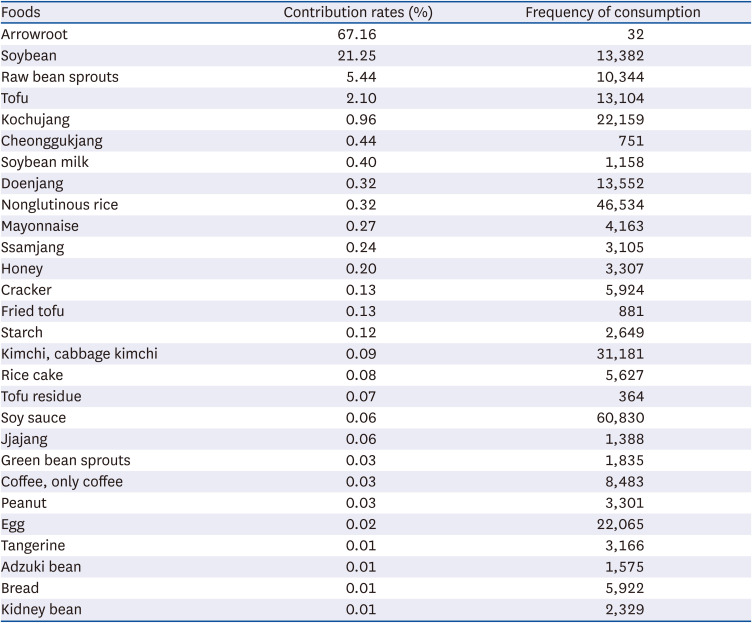
Table 2
Contribution rates and frequency for individual food sources of isoflavone
![]()
Average and usual intake of total isoflavone according to age groups
Table 3 lists the average total isoflavone intake in the Korean population (KNHANES VII) according to the age groups. The average intake of the 50–64 yrs age group was highest (287.87 mg) across all age groups. In the 50–64 yrs age group, a significant difference of 579.77 mg was detected between the 99th (790.41 mg) and 95th percentile (210.64 mg) (Table 3).
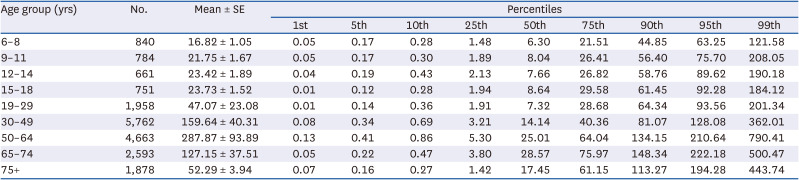
Table 3
Average intake* of total isoflavone in the Korean population (KNHANES VII) according to the age groups
![]()
Table 4 presents the usual total isoflavone intake in Koreans according to the age groups. The 50–64 yrs age group showed the highest usual total isoflavone intake (62.32 mg). In the 50–64 yrs age group, the usual intakes at the 99th and 95th percentile were 220.42 mg and 110.59 mg, respectively (Table 4).
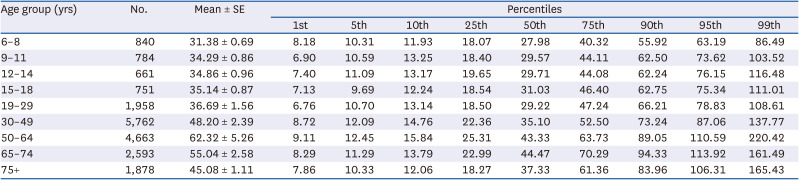
Table 4
Usual intake* of total isoflavone in the Korean population (KNHANES VII) according to age groups
![]()
The average and usual intake of total isoflavone according to gender and age groups
Table 5 lists the average total isoflavone intake in Koreans according to gender and age groups. The distribution had a long tail to the right. The mean total isoflavone intake was 139.27 mg, but the median total isoflavone intake was 13.96 mg (data not shown), indicating that the mean was increased by extreme values. The isoflavone intake distribution was also presented according to gender and age groups. Overall, average isoflavone intake was likely to increase with age. The 50–64 yrs age group showed the highest isoflavone intake for both men and women (men: 232.45mg, women: 343.01mg), with the 50–64-yrs-old women group showing the highest intake. On the other hand, the isoflavone intake decreased for the participants aged 65 yrs and older. Among the participants aged 6 to 18 yrs and 65 yrs and older, the average isoflavone intake of men was higher than that of women. The average isoflavone intake of women was higher than that of men aged 19 to 64 yrs. Overall, the isoflavone intake at the 99th percentile (379.02 mg/d) was much higher than that at the 95th percentile (146.95 mg/d) in most age and gender groups resulting in an increase in average isoflavone intake (Table 5).
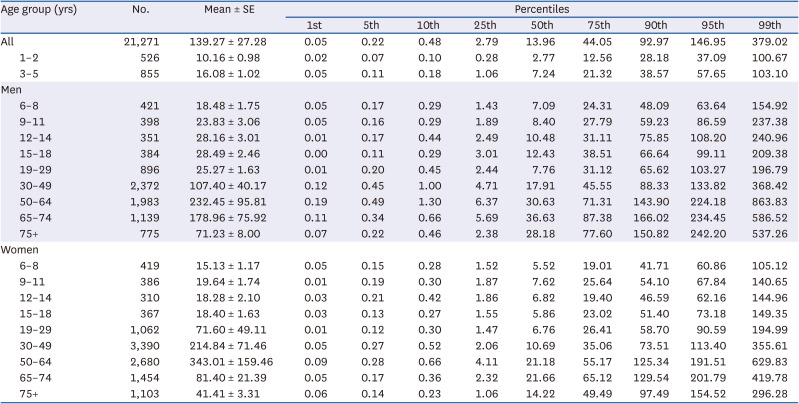
Table 5
Average intake* of total isoflavone in the Korean population (KNHANES VII) according to gender and age groups
![]()
Table 6 lists the estimated usual intake of the total isoflavone by gender and age groups using the NCI 1-d method. The usual intake in the Korean population was 47.44 mg and the SE was 1.60. The usual intake decreased significantly compared to the average intake (Table 5), and the SEs were small. The difference between the median value (data not shown) and the mean value of the usual intake also decreased compared to the difference in average intake. The usual intake at the 99th percentile (149.42 mg/d) was similar to the intake at the 95th percentile (94.32 mg/d). As shown in Table 6, the usual total isoflavone intake ranged from 30 to 40 mg per day in both men and women under the age of 30. The usual intake of subjects aged 30 yrs and older was higher than that of subjects under 30 yrs, showing the highest intake level in the 50–64 yrs age group. The usual isoflavone intakes of men and women aged 30–49 yrs were 47.57 and 48.88 mg/d, respectively, while the usual isoflavone intakes of men and women aged 50–64 yrs were 62.00 and 62.63 mg/d, respectively. There appeared to be no gender difference in the age group under 64 yrs of age, whereas in the age group 65 yrs and older, the usual isoflavone intake of men was higher than that of women (Table 6).
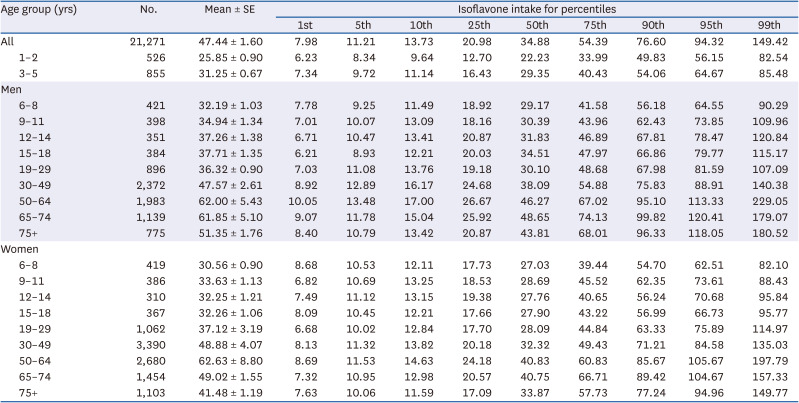
Table 6
Usual intake* of total isoflavone in the Korean population (KNHANES VII) according to gender and age groups
![]()
Go to :
DISCUSSION
This study evaluated the usual isoflavone intake and its major food sources for different age groups by gender in the Korean population using an expanded isoflavone database and a 24-h dietary recall data of KNHANES VII. The present study showed that the average intake and usual intake differed according to age and gender. The average intake showed a gender difference in all age groups, while the usual intake showed a gender difference only in the age group over 65 yrs old. The difference between the average intake and the usual intake is likely to be more pronounced when a large quantity of foods high in isoflavones are consumed occasionally.
The usual dietary isoflavone intake was greater among adults aged 30 yrs and older than those aged under 30 yrs (30–40 mg for those aged < 30 yrs, over 47 mg for those aged 30 yrs and older except for women aged 75 yrs and older), which is consistent with the results by Lee and Kim [45]. Korean adults aged 50–64 yrs consumed the highest amount of total isoflavone across all age groups.
In this study, the usual intake of isoflavone in adults aged 20 yrs and older was greater than the results of Lee and Kim [45]. They reported a mean isoflavone intake of 23.1 mg/d in Korean adults aged 20 yrs and older with a substantial variation among individuals (16.9 mg/d [0–190 mg] at the 50th percentile; 10% of individuals consumed 50 mg/d; and 10% of individuals consumed 5 mg/d) [45].
In a previous European study on the total isoflavone intake across four countries [39], dietary isoflavone intakes were 913 µg/d in the Netherlands, 726 µg/d in Ireland, 718 µg/d in the UK, and 554 µg/d in Italy [39]. The main sources of isoflavones in European countries were soy products, followed by legumes and (pea) nuts, bread, and breakfast cereals [39]. Individuals (aged 35–74 yrs) in most European countries [4151] consumed less than 3 mg/d of isoflavones. Individuals (aged ≥ 19 yrs) in the USA also consumed less than 3 mg/d of isoflavones (1.0 mg/day or 0.7 mg/1,000 kcal) [52]. The mean daily isoflavone intake of Australian men and women aged 39–65 yrs was 2.22 mg. The main sources of isoflavone were bread followed by minced-meat dishes, tofu, soy-based noodles and pasta, minced meat as a sauce, soybeans, coffee, soy crisps/snacks, and tempeh [40]. Japanese people (aged 19–80 yrs) consumed 25 to 50 mg per day [32]. Adults in Hong Kong and Singapore consumed less isoflavones than those in Japan. In particular, China showed regional variations in intake [32]. Asian countries tend to consume more isoflavones than European countries owing to their higher intake of soy or soy products [323752535455]. Wakai et al. [33] reported that soy foods, such as tofu, miso, natto, and fried tofu, accounted for approximately 90% of the total isoflavone intake in Japan.
In the present study, the usual intakes of isoflavone were 32–35 mg/d in Korean children (aged 6–11 yrs). These results are inconsistent with previous findings of isoflavone intake of 8 mg/d in Korean children (aged 8–11 yrs) [5657]. The discrepancy in Korean children can be explained by the differences in their family’s dietary patterns. Owing to the rapid westernization of the Korean diet, various dietary patterns coexist, along with the Korean traditional diet pattern and the Western-style pattern. According to Lee et al. [58], using a 24-h dietary recall in the 2008 KNHANES, isoflavone intake was 30.4 mg/d in children aged 2–18 yrs and consumed the recommended daily intakes of fruits and vegetables, whereas the isoflavone intake was 4.9 mg/d in children who did not consume the recommended daily intakes of fruits and vegetables. Compared to other Asian countries, the daily isoflavone intake was 12–14 mg/d in Japanese children (aged 1–6 yrs) [59]. In Chinese children (aged 1–14 yrs), daily isoflavone intake was 500 µg/kg body weight [60]. Taiwanese children aged 8–9 yrs consumed 36.6 mg/d [61]. Overall, there are differences in usual isoflavone intakes according to age and gender within Korea. An inconsistency in the usual isoflavone intake has been observed among countries or ethnicities and dietary patterns via cumulated evidence.
This study also found that the major contributing food groups to the isoflavone intake in Korea were legumes (91%), vegetables (5.6%), and seasonings (2.1%). Thus, certain dietary patterns that include these contributors, such as legumes, may contribute to the usual isoflavone intake, as mentioned above. This study identified legumes (90%) as a major food group contributing to isoflavone in Korea, which was consistent with a previous study [4245]. As for the major individual food sources of total isoflavone, arrowroot showed the highest proportion of total isoflavone intake (67.16%) owing to its high isoflavone content. There is the possibility that arrowroot was consumed on certain days when the KNHANES was performed, which resulted in the highest arrowroot intake in the legumes food group. As arrowroot is not a frequently consumed food, dietary data based on a one-day 24-h dietary recall in KNHANES may result in large variations in the isoflavone intake level between the consumer group and non-consumer group. Therefore, further study will be needed to estimate the daily consumption, which may provide more specific and realistic data on the food sources of the isoflavone intake.
This study had some limitations. First, recall bias can exist as the 24-h dietary recall data depends on the subjects’ memory, which can lead to under- or overestimations of the total isoflavone intake. Second, the estimated isoflavone intake can be reduced or elevated if more food sources of isoflavone are added (updated) to the isoflavone database. Third, the dominant isoflavone sources, especially arrowroot, which are not foods commonly consumed by the general population, may result in greater variations among individuals.
Despite the limitations, these findings provide crucial information. To the best of the authors’ knowledge, this is the first study to estimate the usual total isoflavone intake and examine the major food sources of isoflavone in the Korean population according to age and gender using KNHANES VII. Furthermore, MIXTRAN macro with the NCI 1-d method as a novel analysis method for KNHANES data was applied in this study to estimate the total isoflavone intake with the 3-yrs data of KNHANES. This study used a nationally representative sample of the Korean population and a national isoflavone database based on a typical diet to provide fundamental evidence for establishing the isoflavone intake recommendations for Koreans, such as dietary reference intakes and recommended dietary allowance. Lastly, this study provided basic data on isoflavone intake for the global comparison between countries according to age and gender.
In conclusion, this study examined the usual isoflavone intake and major food sources of isoflavone in the Korean population according to age and gender. This study provides fundamental data for future studies investigating the relationship between the isoflavone intake and human health.
Go to :
 XML Download
XML Download