

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Menopause is when women are no longer able to become pregnant. After menopause, called post-menopause, the circulating estradiol levels of women decline with a concomitant increase in follicle-stimulating hormone (FSH) and luteinizing hormone (LH) levels [1]. These hormonal changes lead to climacteric symptoms, such as hot flashes and night sweats, which affect the quality of life and have a high risk of osteoporosis and metabolic disorder. Hormone replacement therapy (HRT) and estrogen replacement therapy (ERT) are the most common therapies for relieving these unpleasant menopausal symptoms and preventing osteoporosis [2]. However, given the potential undesirable side effects (e.g., breast cancer and cardiovascular disease) of HRT and ERT [34], it is essential to develop alternatives to traditional HRT/ERT with little or no side effects to relieve the menopausal symptoms of postmenopausal women.
Plant-based estrogens, called phytoestrogens, and herbal derivatives have been reported to reduce menopausal symptoms and are considered alternatives to HRT/ ERT [5]. Phytoestrogens are large families of plant-derived estrogens that possess estrogen-modulating activity, share structural similarities with mammalian estrogen, and bind to estrogen receptors (ERs) to serve as agonists or antagonists. Phytoestrogens act as natural selective estrogen receptor modulators to prevent postmenopausal symptoms without adverse effects [6]. Among phytoestrogens, isoflavones, which are found mainly in legumes (particularly soybeans and red clover), are the most widely used plant-based estrogen [7]. Isoflavones usually present as glycosides, including genistin, daidzin, and glycitin, and have structural similarities to estradiol. These compounds have a high binding affinity with ERs, particularly ERb, and compete with estradiol [8]. Emerging epidemiological evidence has shown an association between high isoflavones consumption and low frequency of hot flashes in women [910]. On the other hand, some of the studies evaluated an inadequate number of participants, a short period, and high dropout rates. Therefore, the current systematic review and meta-analysis of published randomized controlled trials (RCTs) examined the effects of dietary isoflavones on symptoms of menopause (Kupperman Index and hot flashes). Furthermore, the influence of isoflavone interventions on the hormonal changes (blood estradiol, FSH, and LH) in healthy postmenopausal women was also quantified.
MATERIAS AND METHODS
Search strategy and data collection
The present study adhered to the PRISMA guidelines. The PubMed and EMBASE databases were searched until April 1st, 2018. The following keywords were used to identify candidate studies: isoflavone, isoflavones for target nutrition component, and menopausal symptoms for target conditions that are clinical endpoints of the present study. Full-text studies published in English were included. Reference lists of the related articles were also searched. Studies in abstract forms were not included.
Inclusion and exclusion criteria
The studies eligible for this meta-analysis should meet all the following criteria: 1) clinical studies with isoflavone or soy product as the main intervention; 2) yielding at least one comparative outcome of the clinical endpoints (menopausal symptoms and hormones, e.g., hot flashes, Kupperman index, estradiol, FSH, and LH related to menopause); 3) randomized controlled study. After searching the 2 databases, 2,866 publications were identified, of which 1,417 were excluded (duplication n = 1,330, no soy or isoflavone intake n = 87). The 1,449 articles were browsed initially based on title and abstract. For multiple studies from a single institution, those involving a larger number of subjects were included. A full-text review (n = 96) was then examined. The pooled analyses were performed according to each clinical endpoint. Studies with the same biological markers for the meta-analysis were then included. The exclusion criteria of this review were as follows: non-human subjects; non-intervention; non-RCT studies (cohort, case–control, cross-sectional, reviews, and commentaries); no isoflavone intake; unhealthy subjects; irrelevant outcomes. Two independent researchers screened the title/abstract reviews and accessed the full text for qualifying the eligibility. Any disagreement was resolved through scrutinized reassessment.
The studies included were heterogeneous and rarely evaluated the same biomarkers in the same way, often using different cut-off points, populations, and biomarker combinations in panels. This paper presents an overview of the available evidence, describing the key characteristics of the included studies, their populations and biomarkers, and outcome measures. The study then searched for similarities that would allow for subgroup meta-analyses, namely the same biomarker, with similar designs, outcome measures, and populations.
Data extraction and quality assessment (risk of bias)
Data extraction was performed using a predesigned form and included the following items: general information, such as the name(s) of the author(s), publication year, number of subjects, clinical information including the health status of subjects, mean age, condition of the control group, duration, detail of intervention, and quantitative results of clinical outcomes. Two independent researchers performed the data extraction process, and any disagreement after comparing the final results was resolved by re-evaluating the literature.
The quality assessment in RCTs was assessed using the Cochrane Risk of Bias Tool 2.0 (RoB 2.0) [11]. According to Cochrane Collaboration’s tool, each component was categorized as “low risk of bias (low)”, “some concerns”, or “high risk of bias (high)”. The components include the following 6 domains: i) random sequence generation, ii) allocation concealment, iii) blinding of participants and personnel, iv) blinding of outcome assessment, v) incomplete outcome data, and vi) selective reporting. Two reviewers independently evaluated the methodological quality of the eligible studies; consensus was reached on the RoB score through discussion.
Data analysis
The principal summary measures were the standardized mean differences (SMD) between the intervention and control groups for meta-analysis. Although RCTs studies were targeted, the random-effects model was used for pooled analyses because the studies were performed in different institutions in many countries and with differences in the interventions. A heterogeneity assessment was performed using I2 statistics [1213]. Significant heterogeneity was defined to be present if I2 exceeded 50% and P-value was < 0.1. For pooled analyses with more than 10 studies [14], visual funnel plot analysis and quantitative Egger’s test [15] were performed to assess the publication bias. For pooled analyses yielding statistically significant results involved high heterogeneity, sensitivity analyses were performed to determine the cause. Because the number of studies included in the present study was small, this study attempted to find the outliers referencing the basic outlier removal method reported by, but not limited to, Harrer et al. [16] (e.g., for which the upper bound of the 95% CI is lower than the lower bound of the 95% CI of the pooled effect [extremely small], or vice versa [extremely large]). All statistical analyses were performed using Comprehensive Meta-Analysis version 3 (Biostat Inc., Englewood, NJ, USA).
RESULTS
Study selection and characteristics of included RCTs
The initial search across databases identified 2,866 records. Among them, 1,330 duplicated records were removed automatically. The remaining 1,536 studies were screened using abstracts and titles. Eighty-seven studies that did not utilize isoflavone or soy isoflavone as their intervention and 1,353 with non-human studies, wrong design, and irrelevant subjects were excluded. Ninety-six studies underwent full-text review to assess eligibility. Finally, 11 studies involving 1,331 subjects were included in the present study (Fig. 1). Search terms combining the keywords in each search engine were used: for PubMed: (isoflavone[tiab] OR isoflavones[tiab] OR “soy isoflavone”[tiab] OR “soy isoflavones”[tiab] OR “isoflavone intervention”[tiab] OR "isoflavone cohort"[tiab] AND (“menopausal symptoms” OR diabetes OR diarrhea OR “metabolic syndrome” OR galactosemia OR osteoporosis OR hypertension OR “anti inflammation” OR hyperlipidemia OR “anti oxidation” OR “kidney disease” OR “breast cancer” OR “lactose intolerance”)); for EMBASE: Search ('isoflavone'/exp OR isoflavone OR 'isoflavones'/exp OR isoflavones OR 'soy isoflavone'/exp OR 'soy isoflavone' OR 'soy isoflavones' OR (soy AND ('isoflavones'/exp OR isoflavones)) OR 'isoflavone intervention' OR 'isoflavone cohort' AND ('menopausal symptoms' OR diabetes OR diarrhea OR 'metabolic syndrome' OR galactosemia OR osteoporosis OR hypertension OR 'anti inflammation' OR hyperlipidemia OR 'anti oxidation' OR 'kidney disease' OR 'breast cancer' OR 'lactose intolerance')) (Supplementary Table 1). Pooled analysis was then performed with specific clinical outcomes; menopausal symptoms and hormones (hot flashes, Kupperman index, estradiol, FSH, and LH levels). Fig. 1 shows the study selection process in detail. All studies (11 studies) were RCTs. Four studies used quantitative isoflavone supplements (e.g., daily 60 to 120 mg of isoflavone) [17181920] and the other 7 studies used soy products [212223242526] or fruit drinks [27] containing isoflavones. The duration of the intervention ranged from 3 mon to 2 yrs. Seven studies investigated the level of estradiol as the clinical outcomes [17181921232627]; 6 studies used hot flashes [202223242728]; 4 studies used the Kupperman index [17202326]; 4 studies used the FSH level [17182327]: 2 studies used LH [1718]. General information of the included studies is demonstrated in Table 1 in detail.
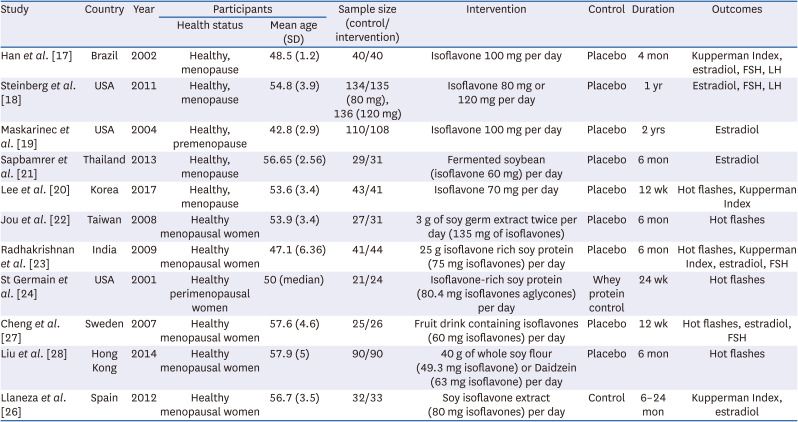
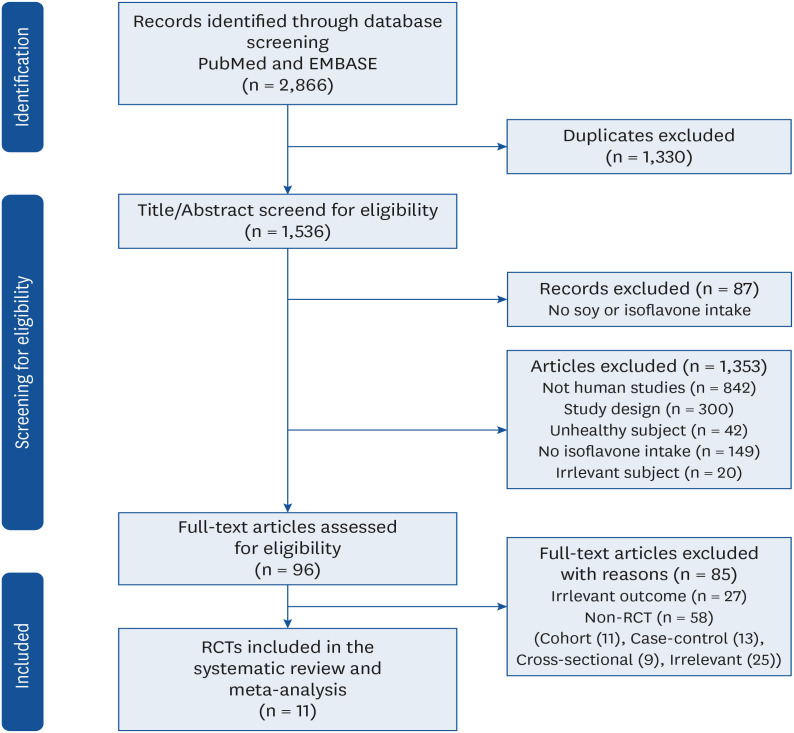
Table 1
Characteristics of the randomized controlled trial studies included
| Study | Country | Year | Participants | Sample size (control/intervention) | Intervention | Control | Duration | Outcomes | |
|---|---|---|---|---|---|---|---|---|---|
| Health status | Mean age (SD) | ||||||||
| Han et al. [17] | Brazil | 2002 | Healthy, menopause | 48.5 (1.2) | 40/40 | Isoflavone 100 mg per day | Placebo | 4 mon | Kupperman Index, estradiol, FSH, LH |
| Steinberg et al. [18] | USA | 2011 | Healthy, menopause | 54.8 (3.9) | 134/135 (80 mg), 136 (120 mg) | Isoflavone 80 mg or 120 mg per day | Placebo | 1 yr | Estradiol, FSH, LH |
| Maskarinec et al. [19] | USA | 2004 | Healthy, premenopause | 42.8 (2.9) | 110/108 | Isoflavone 100 mg per day | Placebo | 2 yrs | Estradiol |
| Sapbamrer et al. [21] | Thailand | 2013 | Healthy, menopause | 56.65 (2.56) | 29/31 | Fermented soybean (isoflavone 60 mg) per day | Placebo | 6 mon | Estradiol |
| Lee et al. [20] | Korea | 2017 | Healthy, menopause | 53.6 (3.4) | 43/41 | Isoflavone 70 mg per day | Placebo | 12 wk | Hot flashes, Kupperman Index |
| Jou et al. [22] | Taiwan | 2008 | Healthy menopausal women | 53.9 (3.4) | 27/31 | 3 g of soy germ extract twice per day (135 mg of isoflavones) | Placebo | 6 mon | Hot flashes |
| Radhakrishnan et al. [23] | India | 2009 | Healthy menopausal women | 47.1 (6.36) | 41/44 | 25 g isoflavone rich soy protein (75 mg isoflavones) per day | Placebo | 6 mon | Hot flashes, Kupperman Index, estradiol, FSH |
| St Germain et al. [24] | USA | 2001 | Healthy perimenopausal women | 50 (median) | 21/24 | Isoflavone-rich soy protein (80.4 mg isoflavones aglycones) per day | Whey protein control | 24 wk | Hot flashes |
| Cheng et al. [27] | Sweden | 2007 | Healthy menopausal women | 57.6 (4.6) | 25/26 | Fruit drink containing isoflavones (60 mg isoflavones) per day | Placebo | 12 wk | Hot flashes, estradiol, FSH |
| Liu et al. [28] | Hong Kong | 2014 | Healthy menopausal women | 57.9 (5) | 90/90 | 40 g of whole soy flour (49.3 mg isoflavone) or Daidzein (63 mg isoflavone) per day | Placebo | 6 mon | Hot flashes |
| Llaneza et al. [26] | Spain | 2012 | Healthy menopausal women | 56.7 (3.5) | 32/33 | Soy isoflavone extract (80 mg isoflavones) per day | Control | 6–24 mon | Kupperman Index, estradiol |
![]()
Risk of bias in studies
As shown in Fig. 2, the risk-of-bias assessment was evaluated and described. Nine articles showed a low risk of selection bias, including random sequence generation and allocation concealment [171819202123262728]. Eight studies possessed a low risk of blinding participants and personnel [1718192021222328], and 3 studies had some concerns of bias [242627]. Eight of the trials provided a clear description of the blinding of the outcome assessment [1718192021232628]. All articles were assessed as having a low risk of bias in incomplete outcome data [1718192021222324262728]. Except for one study [22], where there were some concerns of bias in selective reporting, the other ten studies were regarded as having a low risk of bias in judging consistency. Seven studies were considered to have a low risk of overall bias [17181920212328]. Four studies [22242627] were assessed as having some concerns about the overall risk of bias in the quality stage because ≥ 1 of their 6 key quality domains had some concerns of bias.
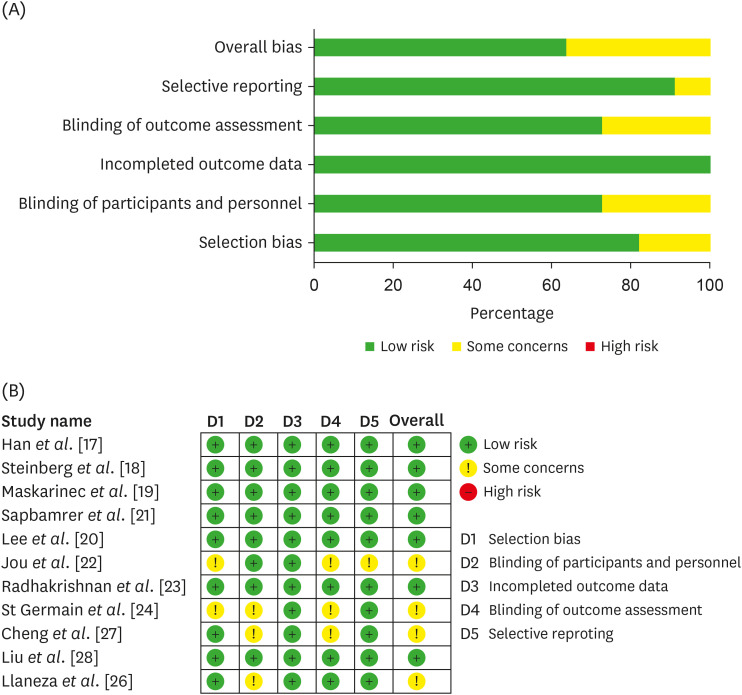
Fig. 2
Risk of bias assessment on the RCTs. Risk of bias analysis across studies (A). Risk of bias item presented as a percentage across all included trials (n = 11); Risk of bias assessment for each study included (B). Green cells with plus mean a low risk of bias; yellow cells with an exclamation point mean some concerns; red cells with a hyphen mean a high risk of bias.
![]()
Effect of isoflavone supplementation on menopausal symptoms
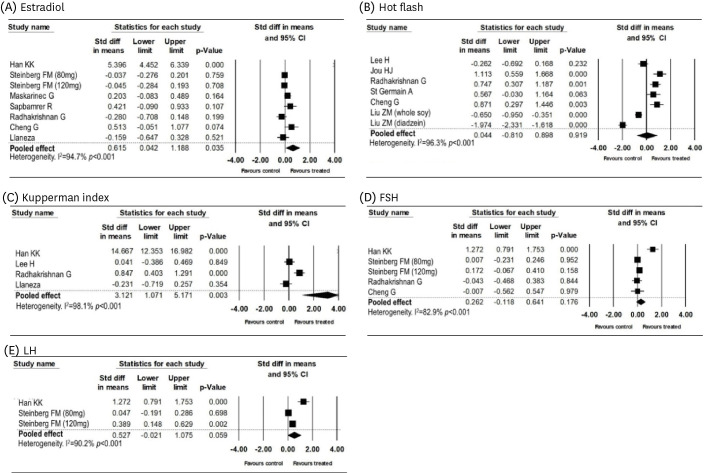
Pooled analyses were performed according to each clinical endpoint. Eight studies were pooled and analyzed for estradiol as a clinical endpoint; the pooled SMD was 0.615 (95% confidence interval [CI], 0.042–1.188; P = 0.035, Fig. 3A). Significant heterogeneity among studies was noted (I2 = 94.7%, P < 0.001). Regarding hot flashes, 6 studies, including 7 cohorts, were analyzed, and the pooled SMD was 0.044 (95% confidence interval [CI], −0.81 to −0.898; P = 0.919; Fig. 3B). The heterogeneity among studies was significant (I2 = 96.3%, P < 0.001). Four studies were available for pooled analysis regarding the Kupperman index, and the pooled SMD was 3.121 (95% CI, 1.071–5.171; P = 0.003, Fig. 3C) with significant heterogeneity (I2 = 98.1% P < 0.001). For FSH, 4 studies involving 5 cohorts were included, and the pooled SMD was 0.262 (95% CI, −0.118 to −0.641; P = 0.176; Fig. 3D) with significant heterogeneity (I2 = 82.9% P < 0.001). Regarding LH, 3 cohorts were analyzed, yielding a pooled SMD of 0.527 (95% CI, −0.021 to −1.075; P = 0.059; Fig. 3E) with significant heterogeneity among the studies (I2 = 90.2%, P < 0.001). The above results are summarized as forest plots in Fig. 3. These results showed that isoflavone intervention increased the estradiol levels significantly but had high heterogeneity among studies (Fig. 3A). On the other hand, an isoflavone intake increased the Kupperman index, a clinical menopause symptom questionnaire used worldwide, but had significant heterogeneity (Fig. 3C). Hot flashes, FSH, and LH levels showed no significant changes between participants who received isoflavones or placebo (Fig. 3B, D, and E). The changes in these indicators suggested that an intervention of isoflavones has a distinct effect on the menopausal symptoms. Quantitative and funnel plot analyses were not conducted because each pooled analysis involved fewer than 10 studies.
Sensitivity analyses for heterogeneity
Since high heterogeneity was noted from pooled analyses, sensitivity analyses were conducted to find the cause (Supplementary Fig. 1). Pooled analyses were performed on estradiol and the Kupperman index, which yielded statistically significant results. Han et al. [17] reported very different results from other studies. Regarding estradiol, the pooled SMD was 0.047 (95% CI, −0.123 to −0.218, P = 0.585), and the heterogeneity was not significant (I2 = 38.6%, P = 0.135) after removing the result by Han et al. [17] Compared to pooled analyses including all available studies, SMD and heterogeneity both became insignificant after removal of the study. Regarding Kupperman index, the pooled SMD was 0.223 (95% CI, −0.405 to −0.852, P = 0.486) with significant heterogeneity (I2 = 82.7%, P = 0.003). After removal, the SMD became insignificant, and the heterogeneity persisted.
DISCUSSION
Isoflavones, which are abundant in soybeans, are considered estrogen-like components that can relieve menopausal symptoms. Although isoflavone has weak ER binding and low potency than estrogen therapy, they have greater potential because of the high concentration in the circulating system (~10,000 times higher than estradiol) [29]. The current systematic review and meta-analysis included 11 RCTs to assess the effects of isoflavones intake on menopausal symptoms. This meta-analysis suggested that isoflavone has beneficial effects on the estradiol levels (Fig. 3A) but not on menopausal symptoms based on the Kupperman index (Fig. 3C). Furthermore, hot flashes, FSH, and LH levels did not reach statistical significance after isoflavone intervention (Fig. 3B, D, and E). Here, this study addressed 2 critical consequences of isoflavone: i) hormonal changes and ii) menopausal symptoms by isoflavone intake.
The usual estradiol levels in premenopausal women are 30 to 400 pg/mL, but these levels decreased to 0–30 pg/mL after menopause. In the present study, the first beneficial effect of isoflavone was the increased estradiol concentration compared to the placebo control group (Fig. 3A). Consistent with this result, Hooper et al., [30] performed a systematic review and meta-analysis on the association between soy protein and isoflavone intervention and circulating hormone concentration (particularly total estradiol) in postmenopausal women. Although there were no statistical significances, there was a slight increase in the total estradiol with soy or isoflavones (~14%, SMD, P = 0.07, 21 studies). By contrast, Fritz et al., [31] in their systematic review, reported that the circulating estradiol or estrogen-response target tissues showed no significant changes according to the soy or isoflavone intakes in patients with or at risk of breast cancer. These conflicting results about the soy and isoflavone intake on ovarian hormones may be due to the participants’ health status. Moreover, it is also plausible to assume that the different concentrations of isoflavones (aglycone equivalent or glycoside weight differences) and duration might have affected the result. Other hormonal changes, such as FSH and LH, were not altered by isoflavone intervention in the present analysis (Fig. 3D and E). Hooper’s systematic review showed that the isoflavone intakes reduced the FSH and LH levels significantly (by 20% SMD, P = 0.01 and 0.05, respectively) [30]. In this study, the high heterogeneity regarding FSH and LH may be due to the limited number of included studies (3 and 2 studies, respectively). Further validation with a large RCT and adequate methodology will be needed. As the underlying assumptions about the results varied among studies, the prevalence of menopausal symptoms might be affected by different ethnic groups. It was reported that Asian women generally less experienced postmenopausal symptoms than women from Western countries [323334]. Moreover, the North American Menopause Society reported the average intake of isoflavones in Caucasian, Hispanic and African women is < 0.5 mg /day, but Asian women showed ~19 times higher intake (> 9.7 mg in China, and > 18 mg in Japan) [35]. This raises the question as to whether the different isoflavone (or soy products) intake and abundance may influence the body’s response to the hormone [36], such as estradiol concentration. Subgroup analysis of Asian vs. non-Asian countries might be a good tool to understand the role of isoflavone on menopausal symptoms because the participant characteristics might have contributed to the heterogeneity.
The second outcome that we immediately noticed was the menopausal symptoms by isoflavone intake. Emerging evidence in a systematic review and meta-analysis articles showed that isoflavone reduced the major menopausal symptoms especially hot flashes and co-occurring symptoms [1037]. In the present study, hot flashes, the main symptom of peri and postmenopausal women, showed no significant changes in this meta-analysis, but the Kupperman index was significantly higher in the isoflavone-supplemented groups (Fig. 3B and C). Other systematic reviews showed that isoflavone supplementation improved hot flashes [91038]. Moreover, it was reported that dietary equol, which is made from isoflavone (particularly daidzein) by equol-producing bacteria, decreases hot flashes in postmenopausal women [39]. These conflicts and controversial conclusions may be due to a lack of evidence and consensus on their efficacy. In agreement with this notion, one report did not confirm the beneficial impact of isoflavone because of the limited number of RCTs, small sample size, and heterogeneity [40]. Various study designs and independent interventions (different forms of the isoflavones, e.g., capsule, food, and extraction methods) might also have affected the controversial results. Considering the variations of phenolic contents/compositions among the different cultivars and harvest periods, it is also difficult to standardize the isoflavone intervention. Among the 11 RCT trials, only one study reported the blood concentration of isoflavones [18]. The authors showed that the blood concentrations of daidzein (isoflavone glycosides) were dramatically higher than those at the baseline and those in the placebo group over the intervention period [18]. Many reports supported the idea that the intervention of isoflavone leads to an increase in the blood concentration of isoflavone (e.g., daidzein) [414243]. Thus, reliable biomarkers are required to support the compliance of isoflavone intervention. Future studies on correlation analysis between the blood isoflavone concentration and menopausal symptoms with a large number of RCT studies are necessary.
When the articles were first screened through systematic review, 14 studies reported adverse events of isoflavone supplementation. Among them, 6 articles reported discontinuation of participation due to serious adverse events or adverse effects of isoflavone [254344454647]. Most of the side effects were abdominal discomfort/pain, nausea, chest tenderness, constipation, skin itching, endometrial hypertrophy, and urinary tract infections. Serious adverse events were breast cancer, uterine cancer, fractures, and stroke, but these were reported to be unrelated to the intervention. The average concentration of isoflavones that reported side effects was 180 mg/day (100–300 mg/day), and the average duration was 17.5 weeks (approximately 4.3 mon) or more (12 wk to 2.5 yrs). Given that China recently set the daily upper limit for soy isoflavones at 120 mg per day when setting the China Dietary Reference Intake, a more cautious and careful review will be needed to combat these issues.
The present work revealed the effects of isoflavones on menopausal symptoms, which have been examined over the past few decades. However, certain limitations still exist in this set of studies. First, there were a limited number of studies included (Hot flash: 7, Kupperman Index: 4, Estradiol: 8, FSH: 5, and LH: 3 studies). Although 2 studies are sufficient to perform a meta-analysis from a formal point of view, it would be desirable to analyze more than 10 studies to acquire statistical power from a practical point of view [4849]. Second, each study used a different type of isoflavone intervention. The independent intervention was classified and categorized based on the isoflavone concentration and period, but it was difficult to understand whether independent intervention would have a similar delivery or bioavailability. A future study will be necessary to find reliable biomarkers representing isoflavone supplementation. Third, this study showed significant heterogeneity among studies. Based on the sensitivity analysis results and the odd results from one of the included studies [17], it is plausible to assume that these factors may be responsible for the high heterogeneity among studies. However, we did not completely figure out the exact cause of high heterogeneity. There are still many unanswered queries and limitations, and it will be meaningful and challenging to combine data accurately to evaluate the Dietary Reference Intakes for Koreans (KDRI) values. Further studies are warranted to unravel the above-mentioned issues by including high quality and a high number of RCT studies.
In conclusion, the current systematic review and meta-analysis showed that isoflavones have discrete effects on menopausal symptoms based on the Kupperman index and estradiol level in postmenopausal women. However, considering the high heterogeneity among the studies, a larger number of high-quality RCTs necessary to draw adequate conclusions.
 XML Download
XML Download