

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Choline belongs to the family of water-soluble quaternary ammonium compounds [1]. Synthesis of 2-Hydroxy-N,N,N-trimethylethan-1-aminium can be achieved de novo in the human body [2]. Choline is considered an essential nutrient in diets since the body produces insufficient quantities for physiological functions [3]. The United States Institute of Medicine (IOM) has officially recognized choline as an essential nutrient and set the Adequate Intakes (AIs) for total choline as dietary reference values since 1998 [4]. Choline AIs were also estimated by the Australian National Health and Medical Research Council (NHMRC) in 2006 [5], the Chinese Nutrition Society (CNS) in 2013 [6], and the European Food Safety Authority (EFSA) in 2016 [7].
Choline and its derivatives have several important functions in the human body, including maintaining the structural integrity of cell membranes and transmembrane signaling, cholinergic neurotransmission, lipid and cholesterol transport, and methyl-group donation in methylation [8910]. Because of its varied roles in human metabolism, choline deficiency or excess intake might be involved in diverse diseases such as non-alcoholic fatty liver disease [1112], atherosclerosis [1314], neurological disorders [1516], and cancers [171819].
In the endogenous pathway for choline biosynthesis, phosphatidylethanolamine is methylated by S-adenosylmethionine as a methyl donor [2]. Thus, dietary choline requirements are affected by the metabolic methyl-exchange relationship between choline and three nutrients: methionine, folate, and vitamin B12 [8]. The necessity of choline can be determined when these nutrients are in sufficient amounts to sustain normal physiological functions [820].
A reference for choline intake is required in Korea due to the increasing interest in choline and the availability of various choline supplements and choline-added foods. However, scientific databases for choline contents in Korean daily foods and choline intake data in Koreans are still lacking, despite numerous studies in the Western countries on choline essentiality and its association with diseases. A systematic literature review on choline was conducted for addition to the 2020 Dietary Reference Intakes for Koreans (KDRIs). However, the committee withheld the setting of choline Dietary Reference Intakes (DRIs) because there was an insufficient scientific basis for establishing its reference intake. The present study aims to provide basic data by analyzing reference values of choline intake and dietary choline intake status by country.
REFERENCE VALUES OF CHOLINE INTAKE BY COUNTRY
The U.S. Food and Nutrition Board of the IOM established the AIs for total choline in 1998 as part of the reference values set for nutrient intakes for healthy populations [4]. AIs were estimated due to insufficient data to derive the Estimated Average Requirements (EARs) for choline. Similarly, the Australian NHMRC [5], the CNS [6], and the EFSA [7] also estimated the reference intake for choline as AIs (Table 1).
Table 1
DRI for choline (mg/d)
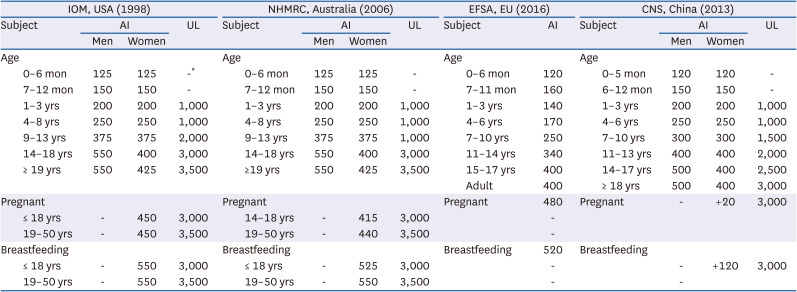
Choline AIs of the IOM were estimated to be 125 mg/day for infants aged 0–6 months based on the volume of milk consumed and its total choline content [2122], and at 150 mg/day for infants aged 7–12 mon by extrapolation from the early infancy body weight [23]. Similarly, the NHMRC set the AIs to be 125 mg/day for infants aged 0–6 mon [2122] and 150 mg/day for infants aged 7–12 mon. The EFSA estimated the AI to be 160 mg/day for infants aged 7–11 mon by upwards extrapolation by allometric scaling from choline intake of exclusively breastfed infants aged 0–6 mon with AI of 120 mg/day [24]. AIs for children and adolescents of all 3 institutions (the IOM, the NHMRC, and the EFSA) were extrapolated using the body weights of adults and growth factors [2526]. For children and adolescents, the AIs estimated by both the IOM and the NHMRC were the same, and were set according to gender. However, AIs of the EFSA were not established by gender.
For choline AIs, major difference was obtained in values for adults between the IOM and the NHMRC compared to the EFSA. The IOM and the NHMRC estimated choline AIs to be 550 mg/day for male adults and 425 mg/day for female adults based on the amount (7 mg/kg/day) that could prevent liver damage as assessed by measuring serum alanine aminotransferase levels [20]. The EFSA set a lower AI of 400 mg/day for both male and female adults based on the mean choline intake observed for healthy populations [27], which is also the amount needed to replete most of the depleted subjects with liver/muscle damage [12].
For pregnant women of all ages and any trimester, the IOM estimated the AI to be 450 mg/day based on fetal and placental choline accumulation [2829], and the EFSA set the AI to be 480 mg/day using isometric scaling and the mean gestational increase in body weight [7]. In contrast, the NHMRC set different values by age group for pregnant women: 415 mg/day for ages 14–18 yrs and 440 mg/day for ages 19 yrs or older. The IOM set the AI to be 550 mg/day for lactating women of all ages, while the NHMRC set AIs to be 525 mg/day for ages 14–18 yrs and 550 mg/day for ages 19 years and above. AIs for lactating women set by the IOM, the NHMRC, and the EFSA were calculated as AIs for non-lactating adult women plus the choline amount secreted in mature milk during the first 6 mon.
Data used to set the Tolerable Upper Intake Levels (ULs) by the IOM and the NHMRC included a single case report of hypotension [30] and several studies involving cholinergic effects and body odor effects after large choline doses [31323334]. The IOM and the NHMRC considered 7.5 g/day of choline as the Lowest Observed Adverse Effect Level (LOAEL). After application of an uncertainty factor of 2 and rounding, the UL of 3.5 g choline/day for adults was established. There are no data to suggest that there is increased susceptibility during pregnancy or lactation; therefore, the ULs remained the same. No UL was established for infants, whereas the ULs for children and adolescents were derived from adult values by allometric scaling according to reference body weights [3536]. The EFSA did not consider ULs for choline.
INTAKE OF CHOLINE IN KOREANS
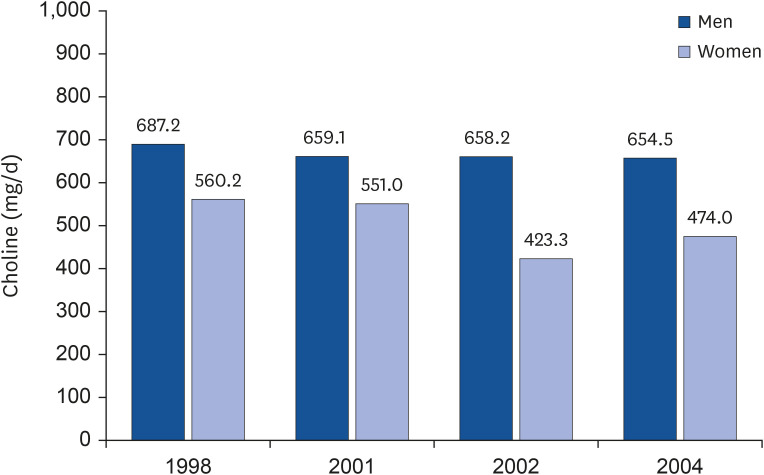
In the assessment by Jeong et al. [35], dietary choline intake of the Korean population in 1998 and 2001 was estimated by gender and age using nationwide data on per capita food intakes obtained from the Korea National Health and Nutrition Examination Survey (KNHANES) (Fig. 1). The average dietary choline intake by Koreans was 623.0 mg/day (687.2 mg/day for men and 560.2 mg/day for women) in 1998, and 602.4 mg/day (659.1 mg/day for men and 551.0 mg/day for women) in 2001. Dietary choline intakes of men were overall higher than in women. The highest consumption of choline among all age groups was 712.0 mg/day in adolescents aged 13–19 yrs in 1998, and 662.2 mg/day in adults aged 30–49 yrs in 2001. The choline database used in these results consisted of data from a total of 165 foods commonly eaten in Korea, selected using the dietary intake data of the 1998 and 2001 KNHANES, a population representative sample survey of Korea, and the 2002 and 2003 Dietary Intake and Risk Assessment of Contaminants in Korean Foods [37]. In addition, the Korea Ministry of Food and Drug Safety (MFDS)’s Food and Nutrition database contains levels of total choline and glycine betaine for processed foods.
Fig. 1
Intake of choline by age in Koreans.
Values are presented as means.
Adopted and modified data from Jeong et al. (2005) [35].
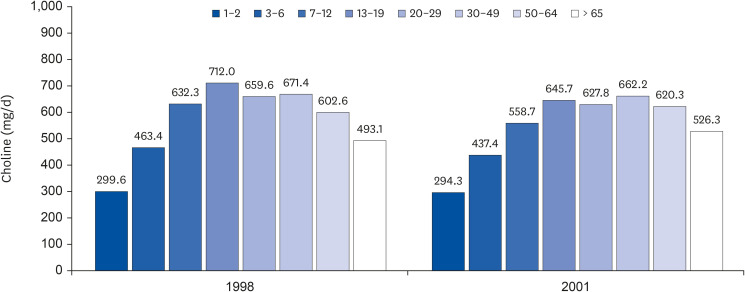
Fig. 2 presents a comparison of choline intake by year of Koreans aged 20-29 years. The dietary choline intake of Korean adults (56 college students in Daejeon area) aged 20–30 years in 2002 was determined by Chung et al. [36]. They reported that men consumed 353.5–1,222.5 mg/day of choline and women consumed 213.1–722.3 mg/day. The mean choline intake was determined to be 658.2 ± 243.9 mg/day for men and 423.3 ± 133.6 mg/day for women, indicating that choline intake in men was about 200 mg/day higher than in women. In a study of choline intake for 30 college students of the same age range in the same region in 2004, the mean intake of choline was 654.53 ± 353.68 mg for men and 473.99 ± 183.76 mg for women [38]. Compared with results for 1998 and 2001 [35], choline intakes in 2002 [36] and 2004 [38] were found to be similar for men but lower for women.
INTAKE OF CHOLINE BY COUNTRY AND RACE
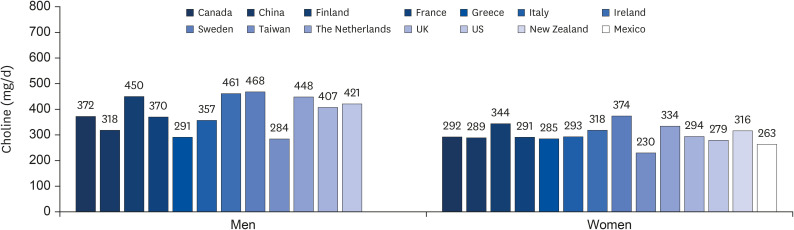
A recent report [39] describes the dietary choline intake from surveys performed in China [40], Mexico [41], New Zealand [41], Taiwan [42], and 9 European countries [27] (Fig. 3). These data show that people in the northern European countries consume higher dietary choline than the population in the Mediterranean countries [27]. Total choline intakes of Japanese adults ranged from 445 mg/day to 513 mg/day for men and from 388 to 442 mg/day for women [43] (data not shown), which were similar to values obtained in northern European countries, but higher than the Chinese [40] and Taiwanese [42] intakes.
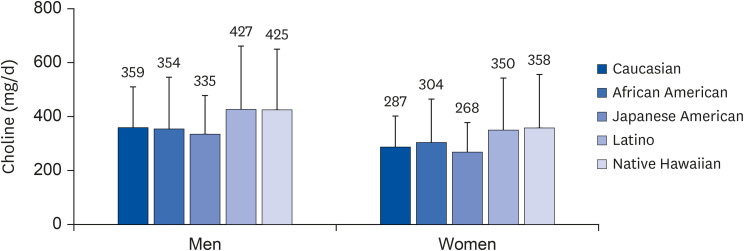
A cohort study has estimated dietary choline intakes among the ethnically diverse adults who participated in the Multiethnic Cohort (MEC) Study [44] (Fig. 4). The cohort consisted of adult men and women living in Hawaii and California, and comprised the following ethnic compositions: African American, Latino, Japanese American, Native Hawaiian, Caucasian, and other ancestries [45]. The study reported that men consumed significantly higher amounts of total choline than women. However, total choline intakes of men and women had similar levels after adjusting for daily energy intake. Furthermore, the energy-adjusted total choline intakes varied significantly by race/ethnicity in both men and women, suggesting that choline intakes could differ by ethnic background.
CONCLUSION
Human studies on Koreans are essential to establish the KDRIs as previous studies have reported differences in the levels of choline intake by race and country. Additionally, an estimate of UL would require examining intakes from supplements, as well as a comprehensive and reliable database of choline content in foods. In order to prevent adverse effects on public health due to choline deficiency and excessive intake, the following studies need to be conducted: randomized controlled trial of choline intake in Korean subjects; observational studies on choline intake in Koreans (including studies on choline metabolism-related gene polymorphisms); examining the effects of dietary choline intake levels on health parameters (including measurements of plasma and tissue choline compounds and metabolites); quantifying the increase in choline requirement, in carriers of alleles requiring an increased need for choline; biomarkers of choline status; consequences of the epigenetic modifications of genes involved in hormonal and vascular physiology, and their expressions following alterations in choline intake during pregnancy; quantitative assessment of choline transfer from mother to the fetus; quantification of the incorporated choline compounds in the body or in different organs during fetal development.
 XML Download
XML Download