INTRODUCTION
The Dietary Reference Intakes for Koreans (KDRIs) are population estimates for daily nutrient requirements and dietary recommendations set by the Korean Ministry of Health and Welfare (MOHW) to maintain the health of the general population by eliminating nutritional deficiencies and reducing the risk of chronic diseases. First established by the Korean Nutrition Society (KNS) in 2005, the KDRIs consist of Estimated Average Requirement (EAR), Recommended Nutrient Intake (RNI), Adequate Intake (AI), Tolerable Upper Intake Level for nutrients, Estimated Energy Requirement for energy, and Acceptable Macronutrient Distribution Range of macronutrients [
12]. The first revision of the KDRIs was in 2010. Since creating the National Nutrition Management Act in 2010, the task to establish and revise the KDRIs has been assigned to the MOHW. The task of revising the KDRIs was thus assigned to the KNS, and in 2015, the KDRIs were first published at the national level [
3]. The 2015 KDRIs comprised life-stage subgroups to be considered when assessing the growth and stages of human development. The KDRI framework has 13 age groups which include the following categories: infants (0–5 and 6–11 mon), toddlers (1–2 and 3–5 yrs), children (6–8 and 9–11 yrs), adolescents (12–14 and 15–18 yrs), adults (19–29, 30–49, and 50–64 yrs), and older adults (65–74 and ≥75 yrs). Moreover, due to physiological characteristics, the age groups ≥ 6 yrs are further classified by gender (male and female) and additional recommendations are given for pregnant and lactating women. The latest version of the KDRIs was released in 2020, following which the necessity to discuss the age subgroups for older adults was broached.
The population of older adults is rapidly increasing around the world. According to the 2015 World Health Organization (WHO) data, Japan was the only country where the proportion of people aged ≥ 60 exceeded 30%. However, by 2050, the proportion of people aged ≥ 60 is expected to exceed 30% in Asia, Europe, and North and South America [
4]. In particular, Korea is one of the countries with the highest growth rate of the elderly population. Statistics published by the Korea National Statistical Office show steady growth in the proportion of older adults aged ≥ 65 yrs in Korea, which is expected to increase to 24.3% by 2030 to become a ‘super-aged society’ [
5]. With the rapidly growing population of the elderly in Korea, it is necessary to reconsider the classification of the older adult age group by scrutinizing domestic and international data and examining the nutritional intake status according to the age of older adults. This article aims to perform a reality check and decipher the reason for the KDRI modifications in the age range for adults ≥ 65 yrs (65–74 and ≥ 75 yrs).
Go to :

AGE GROUP FOR OLDER ADULTS IN THE NATIONAL STATISTICAL DATA OF KOREA
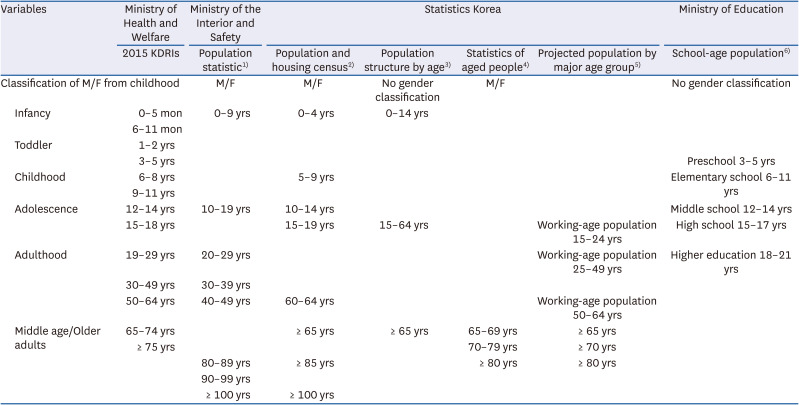
Based on the data obtained from the Ministry of the Interior and Safety of South Korea (MOIS) and Statistics Korea (KOSTAT), including the 2015 KDRIs which used age classification data, we investigated the current status of age classification in domestic statistical data (
Table 1). The age group of older adults in the 2015 KDRIs is subdivided into the age groups 65–74 and ≥ 75 yrs [
3]. Korea’s official population statistics of resident registration categorized males and females separately (by gender) and by 10-yr age intervals (0–9, 10–19, … 70–79, 80–89, 90–99, and ≥ 100 yrs) [
6]. The Korean Statistical Information Service (KOSIS) of KOSTAT divided males and females separately and by age: below 65 yrs were grouped by 5-yr intervals, and ≥ 65 yrs were divided into 3 groups (≥ 65, ≥ 85, and ≥ 100 yrs) [
8]. The KOSTAT ‘Statistics of Aged People’ divided males and females separately and classified the ages into 65–69, 70–79, and ≥ 80 yrs [
9]. The KOSTAT ‘Projected Population by Major Age Group’ classification included the working-age population (15–24, 25–49, and 50–64 yrs) and the aged population (65–74, 75–84, and ≥ 85 yrs), with 3 subgroups each [
10]. The Korean Ministry of Education divided the school-age population into preschool (3–5 yrs), elementary school (6–11 yrs), middle school (12–14 yrs), high school (15–17 yrs), and higher education (18–21 yrs), but did not distinguish between genders [
11]. In addition, the ‘Korean National Survey on Elderly’ conducted by the Korea Institute for Health and Social Affairs classified age ≥ 65 yrs into 5-yr intervals (65–69, 70–74, 75–79, 80–84, and ≥ 85 yrs) [
12]. In the field of geriatric medicine, such as the Korean Academy of Clinical Geriatrics and the Korean Gerontological Nursing Society, age is divided into 5- or 10-yr intervals and includes the subgroups 80, 85, and ≥ 100 yrs. The Korea Centers for Disease Control and Prevention (KCDC) divides the seniors into 60–69 and ≥ 70 yrs by 10-yr intervals in the ‘Korea Community Health Survey’ [
13], whereas the Korea National Health and Nutrition Examination Survey (KNHANES) divides the older adults into 60–69 and > 70 or > 65 yrs [
14].
Table 1
Comparison of age segments in the national statistics of Korea
|
Variables |
Ministry of Health and Welfare |
Ministry of the Interior and Safety |
Statistics Korea |
Ministry of Education |
|
2015 KDRIs |
Population statistic1)
|
Population and housing census2)
|
Population structure by age3)
|
Statistics of aged people4)
|
Projected population by major age group5)
|
School-age population6)
|
|
Classification of M/F from childhood |
M/F |
M/F |
No gender classification |
M/F |
|
No gender classification |
|
Infancy |
0–5 mon |
0–9 yrs |
0–4 yrs |
0–14 yrs |
|
|
|
|
6–11 mon |
|
|
|
|
|
|
|
Toddler |
1–2 yrs |
|
|
|
|
|
|
|
3–5 yrs |
|
|
|
|
|
Preschool 3–5 yrs |
|
Childhood |
6–8 yrs |
|
5–9 yrs |
|
|
|
Elementary school 6–11 yrs |
|
9–11 yrs |
|
|
|
|
|
|
Adolescence |
12–14 yrs |
10–19 yrs |
10–14 yrs |
|
|
|
Middle school 12–14 yrs |
|
15–18 yrs |
|
15–19 yrs |
15–64 yrs |
|
Working-age population 15–24 yrs |
High school 15–17 yrs |
|
Adulthood |
19–29 yrs |
20–29 yrs |
|
|
|
Working-age population 25–49 yrs |
Higher education 18–21 yrs |
|
30–49 yrs |
30–39 yrs |
|
|
|
|
|
|
50–64 yrs |
40–49 yrs |
60–64 yrs |
|
|
Working-age population 50–64 yrs |
|
|
Middle age/Older adults |
65–74 yrs |
|
≥ 65 yrs |
≥ 65 yrs |
65–69 yrs |
≥ 65 yrs |
|
|
≥ 75 yrs |
|
|
|
70–79 yrs |
≥ 70 yrs |
|
|
80–89 yrs |
≥ 85 yrs |
|
≥ 80 yrs |
≥ 80 yrs |
|
|
90–99 yrs |
|
|
|
|
|
|
≥ 100 yrs |
≥ 100 yrs |
|
|
|
|

Go to :
AGE GROUP FOR OLDER ADULTS IN OTHER COUNTRIES
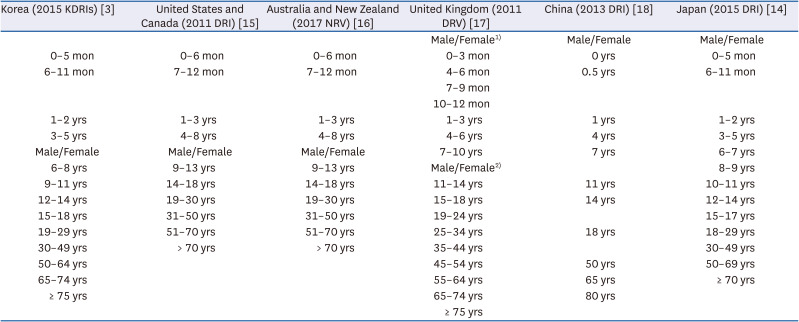
When comparing the age range for Dietary Reference Intakes (DRIs) with other countries, the older adult age group of the United Kingdoms (UK), China, and South Korea was the most subdivided (
Table 2). The 2015 DRIs in Japan [
15], the 2011 DRIs in the United States and Canada [
16], and the 2017 Nutrient Reference Values in Australia and New Zealand [
17] do not classify age ranges over 70 yrs, while the 2011 Dietary Reference Values in the UK [
18] and the 2015 DRIs in South Korea [
3] are presented for ages up to > 75 yrs. The 2013 DRI of China [
19] divides older adults into the groups 65–79 and ≥ 80 yrs. In addition, the United Nations classifies the age ranges of older adults as ≥ 60 or ≥ 65 yrs. WHO’s ‘World Report on Ageing and Health’ presents age ranges up to 85 or 100 yrs by dividing the age into 5- or 10-yr intervals [
4]. The WHO 2000–2025 standard population is divided by age range into 5-yr periods and 9 subgroups for older adults (60–64, 65–69, 70–74, …, 90–94, 95–99, and ≥ 100 yrs) [
4]. The 2011 DRIs of the United States and Canada [
16] do not classify age groups over 70 yrs, but suggest that for adults aged over 70 yrs, the DRIs should reflect the variations in the calculation of EAR and AI because of the large variation in physical activity and individual differences in functional capacity. In addition, the WHO’s ‘World Report on Aging and Health’ [
4] reports that with progressing age, there is a decrease in the physical capacity, which is reported to vary greatly from person to person due to the individual environment interaction. Several foreign countries have presented the necessity to examine the classification of the age group of older adults, but since no grounds for changing the age range have been provided, the age range for older adults remains unchanged.
Table 2
Comparison of age groups for DRIs of Korea with other countries
|
Korea (2015 KDRIs) [3] |
United States and Canada (2011 DRI) [15] |
Australia and New Zealand (2017 NRV) [16] |
United Kingdom (2011 DRV) [17] |
China (2013 DRI) [18] |
Japan (2015 DRI) [14] |
|
|
|
Male/Female1)
|
Male/Female |
Male/Female |
|
0–5 mon |
0–6 mon |
0–6 mon |
0–3 mon |
0 yrs |
0–5 mon |
|
6–11 mon |
7–12 mon |
7–12 mon |
4–6 mon |
0.5 yrs |
6–11 mon |
|
|
|
7–9 mon |
|
|
|
|
|
10–12 mon |
|
|
|
1–2 yrs |
1–3 yrs |
1–3 yrs |
1–3 yrs |
1 yrs |
1–2 yrs |
|
3–5 yrs |
4–8 yrs |
4–8 yrs |
4–6 yrs |
4 yrs |
3–5 yrs |
|
Male/Female |
Male/Female |
Male/Female |
7–10 yrs |
7 yrs |
6–7 yrs |
|
6–8 yrs |
9–13 yrs |
9–13 yrs |
Male/Female2)
|
|
8–9 yrs |
|
9–11 yrs |
14–18 yrs |
14–18 yrs |
11–14 yrs |
11 yrs |
10–11 yrs |
|
12–14 yrs |
19–30 yrs |
19–30 yrs |
15–18 yrs |
14 yrs |
12–14 yrs |
|
15–18 yrs |
31–50 yrs |
31–50 yrs |
19–24 yrs |
|
15–17 yrs |
|
19–29 yrs |
51–70 yrs |
51–70 yrs |
25–34 yrs |
18 yrs |
18–29 yrs |
|
30–49 yrs |
> 70 yrs |
> 70 yrs |
35–44 yrs |
|
30–49 yrs |
|
50–64 yrs |
|
|
45–54 yrs |
50 yrs |
50–69 yrs |
|
65–74 yrs |
|
|
55–64 yrs |
65 yrs |
≥ 70 yrs |
|
≥ 75 yrs |
|
|
65–74 yrs |
80 yrs |
|
|
|
|
≥ 75 yrs |
|
|
Go to :
NUTRITIONAL INTAKE STATUS OF OLDER ADULTS
Data from the 6th and 7th KNHANES (2013–2017), a cross-sectional, nationally representative survey carried out by the KCDC, were examined to clarify characteristics of the nutritional intake status of older adults. The KNHANES uses a stratified, multistage sampling method and comprises 3 surveys: a health interview, a health examination, and a nutrition survey. Detailed information of KNHANES is available on the website (
https://knhanes.kdca.go.kr). The study population encompassed males and females aged ≥ 50 yrs who responded to the 2013–2017 KNHANES (n = 16,410). The following exclusion criteria were applied: subjects without the 24-h dietary recall data (n = 4,347), pregnant or lactating women (n = 11), subjects with a self-reported doctor-diagnosed disease such as hypertension, dyslipidemia, stroke, myocardial infarction or angina pectoris, arthritis, and various cancers (n = 10,431), subjects who consumed differently than the usual intake (n = 1,056), and subjects with daily calorie intake levels less than 500 kcal/day or more than 5,000 kcal/day (n = 33). A total of 3,213 participants (1,685 males and 1,528 females) were included in the final analysis. The 2013-2014 KNHANES protocol was approved by the Institutional Review Board of the KCDC (2013-07CON-03-4C and 2013-12EXP-03-5C), whereas the 2015-2017 KNHANES were exempted from research ethics review based on the Bioethics and Safety Act. Written informed consent was obtained from all participants.
The nutrient adequacy ratio (NAR) was calculated for each of the 9 nutrients (protein, vitamin A, thiamine, riboflavin, niacin, vitamin C, calcium, phosphorus, and iron) using the following formula: NAR = Subject’s Daily Intake of a Nutrient/RNI of that nutrient according to the subject’s gender and age. For a given nutrient, the NAR is the ratio of the subject’s intake to the RNI but is limited not to exceed 1. The nutrient consumed is less than the RNI when the NAR is < 1; the nutrient consumed is greater than or equal to the RNI when the NAR is 1 [
20]. To evaluate the overall dietary adequacy, the mean adequacy ratio (MAR), which is the mean value of 9 NARs, was calculated using the following formula: MAR = ƩNAR (each truncated at 1)/Number of Nutrients. In this study, nutrient intake was assessed based on the 2015 KDRIs [
3].
All statistical analyses were performed using the SAS software (version 9.4; SAS Institute, Inc., Cary, NC, USA). Due to the complex sampling design of the KNHANES study, our analysis considered the relevant primary sampling units, stratification, and sample weights. Nutrient intake status (MAR) in older adults is expressed as weighted means and SEMs using the procedures of SURVEYMEANS. A 3-yr moving average was applied to smooth the mean ages against the nutrient intake trends using the PROC EXPAND procedure. A piecewise linear regression model (using the PROC GLIMMIX procedure) [
2122] was used to observe significant changes in the linear regression slope of nutrient intakes across 2 age groups (under or over a specific age). All dietary nutrient intake variables (carbohydrate, protein, fat, vitamin A, thiamine, riboflavin, niacin, vitamin C, calcium, phosphorus, iron, sodium, and potassium) were energy-adjusted using the residuals method, before applying a piecewise linear regression model.
We first examined the association between energy-adjusted nutrient intake and age group across each gender using the piecewise linear regression model. In this model, the scatter plot is divided into 2 parts (at each point of age 65, 70, and 75 yrs), and 2 separate and connected lines fitted, one for each piece function connected at the knot point. The piecewise linear regression model where 2 pieces are connected at χ = 65, χ = 70, χ = 75 can be formulated as follows:
This formula is for the age 65 years as the knot point and can be simplified as follows:
where χ1 is age, and ß1 is the slope of age. The interaction effect term (ß2) shows the difference in intake by age group, while χ2 is a dummy variable (0 if χ1 < 65, and 1 if χ1 ≥ 65). χ2* denotes ß2 (χ1 − 65) χ2, the interaction effect term.
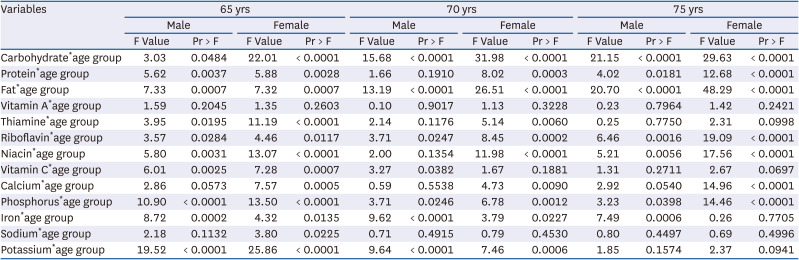
Results of the piecewise linear regression for each of the 13 nutrients (carbohydrate, protein, fat, vitamin A, thiamine, riboflavin, niacin, vitamin C, calcium, phosphorus, iron, sodium, and potassium) revealed maximum interaction effect in the groups aged under and over 65 yrs (50–64 and 65–80; 10 and 12 nutrients were significant in males and females, respectively), as compared to the groups aged under and over 70 yrs (50–69 and 70–80; 7 and 10 nutrients were significant in males and females, respectively), and under and over 75 yrs (50–74 and 75–80; 7 nutrients were significant in both males and females).
None of the nutrients showed an interaction effect on the groups aged under and over 65 yrs (50–64 and 65–80), whereas groups aged under and over 70 yrs (50–69 and 70–80), or under and over 75 yrs (50–74 and 75–80) showed an interaction effect on nutrient intake (
Table 3).
Table 3
The association between energy-adjusted nutrient intake and age group across each gender using piecewise linear regression model; age group (under and over a specific age)
|
Variables |
65 yrs |
70 yrs |
75 yrs |
|
Male |
Female |
Male |
Female |
Male |
Female |
|
F Value |
Pr > F |
F Value |
Pr > F |
F Value |
Pr > F |
F Value |
Pr > F |
F Value |
Pr > F |
F Value |
Pr > F |
|
Carbohydrate*age group |
3.03 |
0.0484 |
22.01 |
< 0.0001 |
15.68 |
< 0.0001 |
31.98 |
< 0.0001 |
21.15 |
< 0.0001 |
29.63 |
< 0.0001 |
|
Protein*age group |
5.62 |
0.0037 |
5.88 |
0.0028 |
1.66 |
0.1910 |
8.02 |
0.0003 |
4.02 |
0.0181 |
12.68 |
< 0.0001 |
|
Fat*age group |
7.33 |
0.0007 |
7.32 |
0.0007 |
13.19 |
< 0.0001 |
26.51 |
< 0.0001 |
20.70 |
< 0.0001 |
48.29 |
< 0.0001 |
|
Vitamin A*age group |
1.59 |
0.2045 |
1.35 |
0.2603 |
0.10 |
0.9017 |
1.13 |
0.3228 |
0.23 |
0.7964 |
1.42 |
0.2421 |
|
Thiamine*age group |
3.95 |
0.0195 |
11.19 |
< 0.0001 |
2.14 |
0.1176 |
5.14 |
0.0060 |
0.25 |
0.7750 |
2.31 |
0.0998 |
|
Riboflavin*age group |
3.57 |
0.0284 |
4.46 |
0.0117 |
3.71 |
0.0247 |
8.45 |
0.0002 |
6.46 |
0.0016 |
19.09 |
< 0.0001 |
|
Niacin*age group |
5.80 |
0.0031 |
13.07 |
< 0.0001 |
2.00 |
0.1354 |
11.98 |
< 0.0001 |
5.21 |
0.0056 |
17.56 |
< 0.0001 |
|
Vitamin C*age group |
6.01 |
0.0025 |
7.28 |
0.0007 |
3.27 |
0.0382 |
1.67 |
0.1881 |
1.31 |
0.2711 |
2.67 |
0.0697 |
|
Calcium*age group |
2.86 |
0.0573 |
7.57 |
0.0005 |
0.59 |
0.5538 |
4.73 |
0.0090 |
2.92 |
0.0540 |
14.96 |
< 0.0001 |
|
Phosphorus*age group |
10.90 |
< 0.0001 |
13.50 |
< 0.0001 |
3.71 |
0.0246 |
6.78 |
0.0012 |
3.23 |
0.0398 |
14.46 |
< 0.0001 |
|
Iron*age group |
8.72 |
0.0002 |
4.32 |
0.0135 |
9.62 |
< 0.0001 |
3.79 |
0.0227 |
7.49 |
0.0006 |
0.26 |
0.7705 |
|
Sodium*age group |
2.18 |
0.1132 |
3.80 |
0.0225 |
0.71 |
0.4915 |
0.79 |
0.4530 |
0.80 |
0.4497 |
0.69 |
0.4996 |
|
Potassium*age group |
19.52 |
< 0.0001 |
25.86 |
< 0.0001 |
9.64 |
< 0.0001 |
7.46 |
0.0006 |
1.85 |
0.1574 |
2.37 |
0.0941 |
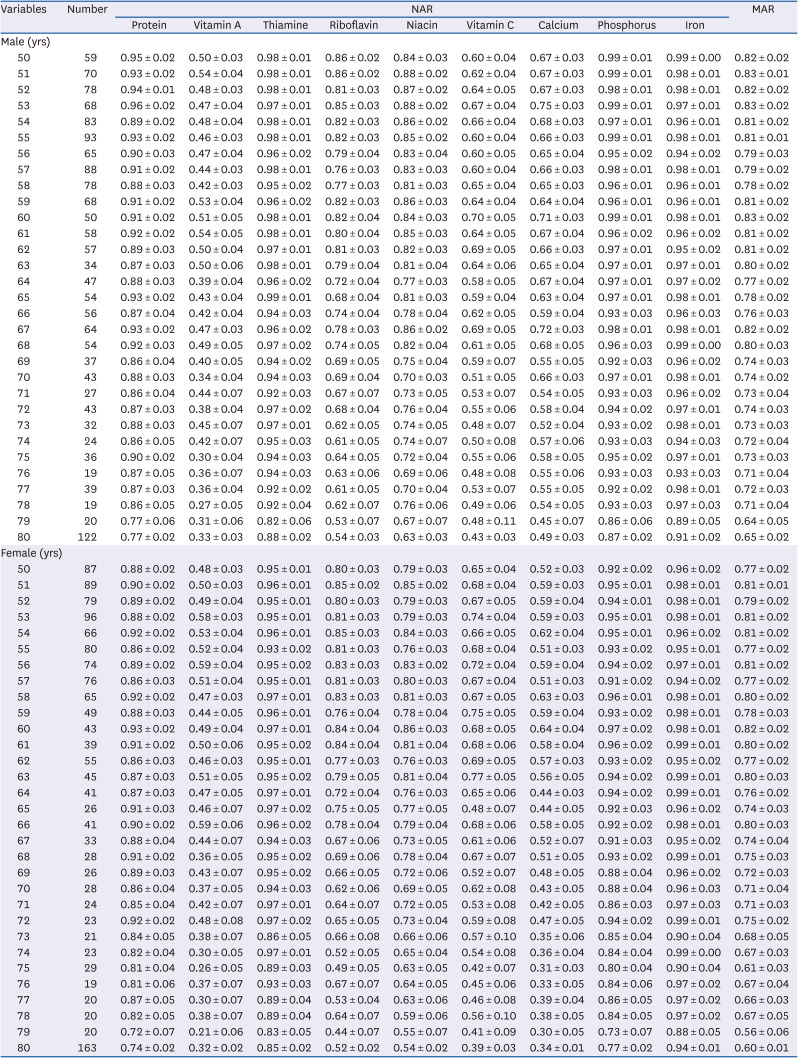
Next, we calculated the MAR and observed the change (reduction) in overall nutrient intake (measured by MAR) trends (whether smooth or not) in older age groups across each gender, using the 3-yr (age) moving average method. Our results revealed an overall decrease in MAR in males, regardless of the age junction (at the age 65, 70, and 75 yrs); in females, the MAR tended to remain constant until 65 yrs of age after which there was a tendency to decrease (
Fig. 1). In addition, in the comparison of MAR by 1-yr interval of age, the age at which MAR started to fall below 0.75 (the standard value indicating nutrient intake adequacy [
23]) was determined to be 69 yrs for males and 65 yrs for females (
Table 4).
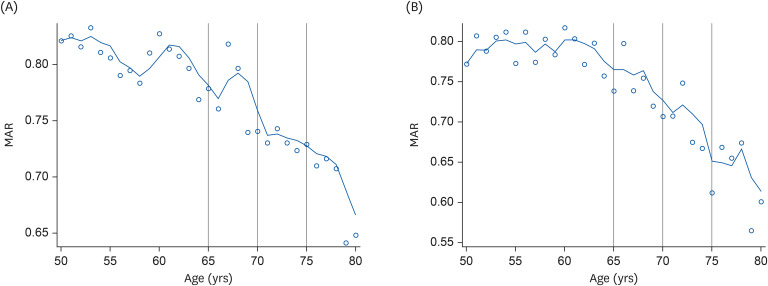 | Fig. 1
Trends of MAR in older adults in South Korea. The smoothed curves were obtained by the 3-yr moving average. X-axis, age (yrs); Y-axis, MAR. (A) Males; (B) Females.
MAR, mean adequacy ratio.

|
Table 4
The NAR and MAR in older adults in South Korea
|
Variables |
Number |
NAR |
MAR |
|
Protein |
Vitamin A |
Thiamine |
Riboflavin |
Niacin |
Vitamin C |
Calcium |
Phosphorus |
Iron |
|
Male (yrs) |
|
|
|
|
|
|
|
|
|
|
|
|
50 |
59 |
0.95 ± 0.02 |
0.50 ± 0.03 |
0.98 ± 0.01 |
0.86 ± 0.02 |
0.84 ± 0.03 |
0.60 ± 0.04 |
0.67 ± 0.03 |
0.99 ± 0.01 |
0.99 ± 0.00 |
0.82 ± 0.02 |
|
51 |
70 |
0.93 ± 0.02 |
0.54 ± 0.04 |
0.98 ± 0.01 |
0.86 ± 0.02 |
0.88 ± 0.02 |
0.62 ± 0.04 |
0.67 ± 0.03 |
0.99 ± 0.01 |
0.98 ± 0.01 |
0.83 ± 0.01 |
|
52 |
78 |
0.94 ± 0.01 |
0.48 ± 0.03 |
0.98 ± 0.01 |
0.81 ± 0.03 |
0.87 ± 0.02 |
0.64 ± 0.05 |
0.67 ± 0.03 |
0.98 ± 0.01 |
0.98 ± 0.01 |
0.82 ± 0.02 |
|
53 |
68 |
0.96 ± 0.02 |
0.47 ± 0.04 |
0.97 ± 0.01 |
0.85 ± 0.03 |
0.88 ± 0.02 |
0.67 ± 0.04 |
0.75 ± 0.03 |
0.99 ± 0.01 |
0.97 ± 0.01 |
0.83 ± 0.02 |
|
54 |
83 |
0.89 ± 0.02 |
0.48 ± 0.04 |
0.98 ± 0.01 |
0.82 ± 0.03 |
0.86 ± 0.02 |
0.66 ± 0.04 |
0.68 ± 0.03 |
0.97 ± 0.01 |
0.96 ± 0.01 |
0.81 ± 0.02 |
|
55 |
93 |
0.93 ± 0.02 |
0.46 ± 0.03 |
0.98 ± 0.01 |
0.82 ± 0.03 |
0.85 ± 0.02 |
0.60 ± 0.04 |
0.66 ± 0.03 |
0.99 ± 0.01 |
0.98 ± 0.01 |
0.81 ± 0.01 |
|
56 |
65 |
0.90 ± 0.03 |
0.47 ± 0.04 |
0.96 ± 0.02 |
0.79 ± 0.04 |
0.83 ± 0.04 |
0.60 ± 0.05 |
0.65 ± 0.04 |
0.95 ± 0.02 |
0.94 ± 0.02 |
0.79 ± 0.03 |
|
57 |
88 |
0.91 ± 0.02 |
0.44 ± 0.03 |
0.98 ± 0.01 |
0.76 ± 0.03 |
0.83 ± 0.03 |
0.60 ± 0.04 |
0.66 ± 0.03 |
0.98 ± 0.01 |
0.98 ± 0.01 |
0.79 ± 0.02 |
|
58 |
78 |
0.88 ± 0.03 |
0.42 ± 0.03 |
0.95 ± 0.02 |
0.77 ± 0.03 |
0.81 ± 0.03 |
0.65 ± 0.04 |
0.65 ± 0.03 |
0.96 ± 0.01 |
0.96 ± 0.01 |
0.78 ± 0.02 |
|
59 |
68 |
0.91 ± 0.02 |
0.53 ± 0.04 |
0.96 ± 0.02 |
0.82 ± 0.03 |
0.86 ± 0.03 |
0.64 ± 0.04 |
0.64 ± 0.04 |
0.96 ± 0.01 |
0.96 ± 0.01 |
0.81 ± 0.02 |
|
60 |
50 |
0.91 ± 0.02 |
0.51 ± 0.05 |
0.98 ± 0.01 |
0.82 ± 0.04 |
0.84 ± 0.03 |
0.70 ± 0.05 |
0.71 ± 0.03 |
0.99 ± 0.01 |
0.98 ± 0.01 |
0.83 ± 0.02 |
|
61 |
58 |
0.92 ± 0.02 |
0.54 ± 0.05 |
0.98 ± 0.01 |
0.80 ± 0.04 |
0.85 ± 0.03 |
0.64 ± 0.05 |
0.67 ± 0.04 |
0.96 ± 0.02 |
0.96 ± 0.02 |
0.81 ± 0.02 |
|
62 |
57 |
0.89 ± 0.03 |
0.50 ± 0.04 |
0.97 ± 0.01 |
0.81 ± 0.03 |
0.82 ± 0.03 |
0.69 ± 0.05 |
0.66 ± 0.03 |
0.97 ± 0.01 |
0.95 ± 0.02 |
0.81 ± 0.02 |
|
63 |
34 |
0.87 ± 0.03 |
0.50 ± 0.06 |
0.98 ± 0.01 |
0.79 ± 0.04 |
0.81 ± 0.04 |
0.64 ± 0.06 |
0.65 ± 0.04 |
0.97 ± 0.01 |
0.97 ± 0.01 |
0.80 ± 0.02 |
|
64 |
47 |
0.88 ± 0.03 |
0.39 ± 0.04 |
0.96 ± 0.02 |
0.72 ± 0.04 |
0.77 ± 0.03 |
0.58 ± 0.05 |
0.67 ± 0.04 |
0.97 ± 0.01 |
0.97 ± 0.02 |
0.77 ± 0.02 |
|
65 |
54 |
0.93 ± 0.02 |
0.43 ± 0.04 |
0.99 ± 0.01 |
0.68 ± 0.04 |
0.81 ± 0.03 |
0.59 ± 0.04 |
0.63 ± 0.04 |
0.97 ± 0.01 |
0.98 ± 0.01 |
0.78 ± 0.02 |
|
66 |
56 |
0.87 ± 0.04 |
0.42 ± 0.04 |
0.94 ± 0.03 |
0.74 ± 0.04 |
0.78 ± 0.04 |
0.62 ± 0.05 |
0.59 ± 0.04 |
0.93 ± 0.03 |
0.96 ± 0.03 |
0.76 ± 0.03 |
|
67 |
64 |
0.93 ± 0.02 |
0.47 ± 0.03 |
0.96 ± 0.02 |
0.78 ± 0.03 |
0.86 ± 0.02 |
0.69 ± 0.05 |
0.72 ± 0.03 |
0.98 ± 0.01 |
0.98 ± 0.01 |
0.82 ± 0.02 |
|
68 |
54 |
0.92 ± 0.03 |
0.49 ± 0.05 |
0.97 ± 0.02 |
0.74 ± 0.05 |
0.82 ± 0.04 |
0.61 ± 0.05 |
0.68 ± 0.05 |
0.96 ± 0.03 |
0.99 ± 0.00 |
0.80 ± 0.03 |
|
69 |
37 |
0.86 ± 0.04 |
0.40 ± 0.05 |
0.94 ± 0.02 |
0.69 ± 0.05 |
0.75 ± 0.04 |
0.59 ± 0.07 |
0.55 ± 0.05 |
0.92 ± 0.03 |
0.96 ± 0.02 |
0.74 ± 0.03 |
|
70 |
43 |
0.88 ± 0.03 |
0.34 ± 0.04 |
0.94 ± 0.03 |
0.69 ± 0.04 |
0.70 ± 0.03 |
0.51 ± 0.05 |
0.66 ± 0.03 |
0.97 ± 0.01 |
0.98 ± 0.01 |
0.74 ± 0.02 |
|
71 |
27 |
0.86 ± 0.04 |
0.44 ± 0.07 |
0.92 ± 0.03 |
0.67 ± 0.07 |
0.73 ± 0.05 |
0.53 ± 0.07 |
0.54 ± 0.05 |
0.93 ± 0.03 |
0.96 ± 0.02 |
0.73 ± 0.04 |
|
72 |
43 |
0.87 ± 0.03 |
0.38 ± 0.04 |
0.97 ± 0.02 |
0.68 ± 0.04 |
0.76 ± 0.04 |
0.55 ± 0.06 |
0.58 ± 0.04 |
0.94 ± 0.02 |
0.97 ± 0.01 |
0.74 ± 0.03 |
|
73 |
32 |
0.88 ± 0.03 |
0.45 ± 0.07 |
0.97 ± 0.01 |
0.62 ± 0.05 |
0.74 ± 0.05 |
0.48 ± 0.07 |
0.52 ± 0.04 |
0.93 ± 0.02 |
0.98 ± 0.01 |
0.73 ± 0.03 |
|
74 |
24 |
0.86 ± 0.05 |
0.42 ± 0.07 |
0.95 ± 0.03 |
0.61 ± 0.05 |
0.74 ± 0.07 |
0.50 ± 0.08 |
0.57 ± 0.06 |
0.93 ± 0.03 |
0.94 ± 0.03 |
0.72 ± 0.04 |
|
75 |
36 |
0.90 ± 0.02 |
0.30 ± 0.04 |
0.94 ± 0.03 |
0.64 ± 0.05 |
0.72 ± 0.04 |
0.55 ± 0.06 |
0.58 ± 0.05 |
0.95 ± 0.02 |
0.97 ± 0.01 |
0.73 ± 0.03 |
|
76 |
19 |
0.87 ± 0.05 |
0.36 ± 0.07 |
0.94 ± 0.03 |
0.63 ± 0.06 |
0.69 ± 0.06 |
0.48 ± 0.08 |
0.55 ± 0.06 |
0.93 ± 0.03 |
0.93 ± 0.03 |
0.71 ± 0.04 |
|
77 |
39 |
0.87 ± 0.03 |
0.36 ± 0.04 |
0.92 ± 0.02 |
0.61 ± 0.05 |
0.70 ± 0.04 |
0.53 ± 0.07 |
0.55 ± 0.05 |
0.92 ± 0.02 |
0.98 ± 0.01 |
0.72 ± 0.03 |
|
78 |
19 |
0.86 ± 0.05 |
0.27 ± 0.05 |
0.92 ± 0.04 |
0.62 ± 0.07 |
0.76 ± 0.06 |
0.49 ± 0.06 |
0.54 ± 0.05 |
0.93 ± 0.03 |
0.97 ± 0.03 |
0.71 ± 0.04 |
|
79 |
20 |
0.77 ± 0.06 |
0.31 ± 0.06 |
0.82 ± 0.06 |
0.53 ± 0.07 |
0.67 ± 0.07 |
0.48 ± 0.11 |
0.45 ± 0.07 |
0.86 ± 0.06 |
0.89 ± 0.05 |
0.64 ± 0.05 |
|
80 |
122 |
0.77 ± 0.02 |
0.33 ± 0.03 |
0.88 ± 0.02 |
0.54 ± 0.03 |
0.63 ± 0.03 |
0.43 ± 0.03 |
0.49 ± 0.03 |
0.87 ± 0.02 |
0.91 ± 0.02 |
0.65 ± 0.02 |
|
Female (yrs) |
|
|
|
|
|
|
|
|
|
|
|
|
50 |
87 |
0.88 ± 0.02 |
0.48 ± 0.03 |
0.95 ± 0.01 |
0.80 ± 0.03 |
0.79 ± 0.03 |
0.65 ± 0.04 |
0.52 ± 0.03 |
0.92 ± 0.02 |
0.96 ± 0.02 |
0.77 ± 0.02 |
|
51 |
89 |
0.90 ± 0.02 |
0.50 ± 0.03 |
0.96 ± 0.01 |
0.85 ± 0.02 |
0.85 ± 0.02 |
0.68 ± 0.04 |
0.59 ± 0.03 |
0.95 ± 0.01 |
0.98 ± 0.01 |
0.81 ± 0.01 |
|
52 |
79 |
0.89 ± 0.02 |
0.49 ± 0.04 |
0.95 ± 0.01 |
0.80 ± 0.03 |
0.79 ± 0.03 |
0.67 ± 0.05 |
0.59 ± 0.04 |
0.94 ± 0.01 |
0.98 ± 0.01 |
0.79 ± 0.02 |
|
53 |
96 |
0.88 ± 0.02 |
0.58 ± 0.03 |
0.95 ± 0.01 |
0.81 ± 0.03 |
0.79 ± 0.03 |
0.74 ± 0.04 |
0.59 ± 0.03 |
0.95 ± 0.01 |
0.98 ± 0.01 |
0.81 ± 0.02 |
|
54 |
66 |
0.92 ± 0.02 |
0.53 ± 0.04 |
0.96 ± 0.01 |
0.85 ± 0.03 |
0.84 ± 0.03 |
0.66 ± 0.05 |
0.62 ± 0.04 |
0.95 ± 0.01 |
0.96 ± 0.02 |
0.81 ± 0.02 |
|
55 |
80 |
0.86 ± 0.02 |
0.52 ± 0.04 |
0.93 ± 0.02 |
0.81 ± 0.03 |
0.76 ± 0.03 |
0.68 ± 0.04 |
0.51 ± 0.03 |
0.93 ± 0.02 |
0.95 ± 0.01 |
0.77 ± 0.02 |
|
56 |
74 |
0.89 ± 0.02 |
0.59 ± 0.04 |
0.95 ± 0.02 |
0.83 ± 0.03 |
0.83 ± 0.02 |
0.72 ± 0.04 |
0.59 ± 0.04 |
0.94 ± 0.02 |
0.97 ± 0.01 |
0.81 ± 0.02 |
|
57 |
76 |
0.86 ± 0.03 |
0.51 ± 0.04 |
0.95 ± 0.01 |
0.81 ± 0.03 |
0.80 ± 0.03 |
0.67 ± 0.04 |
0.51 ± 0.03 |
0.91 ± 0.02 |
0.94 ± 0.02 |
0.77 ± 0.02 |
|
58 |
65 |
0.92 ± 0.02 |
0.47 ± 0.03 |
0.97 ± 0.01 |
0.83 ± 0.03 |
0.81 ± 0.03 |
0.67 ± 0.05 |
0.63 ± 0.03 |
0.96 ± 0.01 |
0.98 ± 0.01 |
0.80 ± 0.02 |
|
59 |
49 |
0.88 ± 0.03 |
0.44 ± 0.05 |
0.96 ± 0.01 |
0.76 ± 0.04 |
0.78 ± 0.04 |
0.75 ± 0.05 |
0.59 ± 0.04 |
0.93 ± 0.02 |
0.98 ± 0.01 |
0.78 ± 0.03 |
|
60 |
43 |
0.93 ± 0.02 |
0.49 ± 0.04 |
0.97 ± 0.01 |
0.84 ± 0.04 |
0.86 ± 0.03 |
0.68 ± 0.05 |
0.64 ± 0.04 |
0.97 ± 0.02 |
0.98 ± 0.01 |
0.82 ± 0.02 |
|
61 |
39 |
0.91 ± 0.02 |
0.50 ± 0.06 |
0.95 ± 0.02 |
0.84 ± 0.04 |
0.81 ± 0.04 |
0.68 ± 0.06 |
0.58 ± 0.04 |
0.96 ± 0.02 |
0.99 ± 0.01 |
0.80 ± 0.02 |
|
62 |
55 |
0.86 ± 0.03 |
0.46 ± 0.03 |
0.95 ± 0.01 |
0.77 ± 0.03 |
0.76 ± 0.03 |
0.69 ± 0.05 |
0.57 ± 0.03 |
0.93 ± 0.02 |
0.95 ± 0.02 |
0.77 ± 0.02 |
|
63 |
45 |
0.87 ± 0.03 |
0.51 ± 0.05 |
0.95 ± 0.02 |
0.79 ± 0.05 |
0.81 ± 0.04 |
0.77 ± 0.05 |
0.56 ± 0.05 |
0.94 ± 0.02 |
0.99 ± 0.01 |
0.80 ± 0.03 |
|
64 |
41 |
0.87 ± 0.03 |
0.47 ± 0.05 |
0.97 ± 0.01 |
0.72 ± 0.04 |
0.76 ± 0.03 |
0.65 ± 0.06 |
0.44 ± 0.03 |
0.94 ± 0.02 |
0.99 ± 0.01 |
0.76 ± 0.02 |
|
65 |
26 |
0.91 ± 0.03 |
0.46 ± 0.07 |
0.97 ± 0.02 |
0.75 ± 0.05 |
0.77 ± 0.05 |
0.48 ± 0.07 |
0.44 ± 0.05 |
0.92 ± 0.03 |
0.96 ± 0.02 |
0.74 ± 0.03 |
|
66 |
41 |
0.90 ± 0.02 |
0.59 ± 0.06 |
0.96 ± 0.02 |
0.78 ± 0.04 |
0.79 ± 0.04 |
0.68 ± 0.06 |
0.58 ± 0.05 |
0.92 ± 0.02 |
0.98 ± 0.01 |
0.80 ± 0.03 |
|
67 |
33 |
0.88 ± 0.04 |
0.44 ± 0.07 |
0.94 ± 0.03 |
0.67 ± 0.06 |
0.73 ± 0.05 |
0.61 ± 0.06 |
0.52 ± 0.07 |
0.91 ± 0.03 |
0.95 ± 0.02 |
0.74 ± 0.04 |
|
68 |
28 |
0.91 ± 0.02 |
0.36 ± 0.05 |
0.95 ± 0.02 |
0.69 ± 0.06 |
0.78 ± 0.04 |
0.67 ± 0.07 |
0.51 ± 0.05 |
0.93 ± 0.02 |
0.99 ± 0.01 |
0.75 ± 0.03 |
|
69 |
26 |
0.89 ± 0.03 |
0.43 ± 0.07 |
0.95 ± 0.02 |
0.66 ± 0.05 |
0.72 ± 0.06 |
0.52 ± 0.07 |
0.48 ± 0.05 |
0.88 ± 0.04 |
0.96 ± 0.02 |
0.72 ± 0.03 |
|
70 |
28 |
0.86 ± 0.04 |
0.37 ± 0.05 |
0.94 ± 0.03 |
0.62 ± 0.06 |
0.69 ± 0.05 |
0.62 ± 0.08 |
0.43 ± 0.05 |
0.88 ± 0.04 |
0.96 ± 0.03 |
0.71 ± 0.04 |
|
71 |
24 |
0.85 ± 0.04 |
0.42 ± 0.07 |
0.97 ± 0.01 |
0.64 ± 0.07 |
0.72 ± 0.05 |
0.53 ± 0.08 |
0.42 ± 0.05 |
0.86 ± 0.03 |
0.97 ± 0.03 |
0.71 ± 0.03 |
|
72 |
23 |
0.92 ± 0.02 |
0.48 ± 0.08 |
0.97 ± 0.02 |
0.65 ± 0.05 |
0.73 ± 0.04 |
0.59 ± 0.08 |
0.47 ± 0.05 |
0.94 ± 0.02 |
0.99 ± 0.01 |
0.75 ± 0.02 |
|
73 |
21 |
0.84 ± 0.05 |
0.38 ± 0.07 |
0.86 ± 0.05 |
0.66 ± 0.08 |
0.66 ± 0.06 |
0.57 ± 0.10 |
0.35 ± 0.06 |
0.85 ± 0.04 |
0.90 ± 0.04 |
0.68 ± 0.05 |
|
74 |
23 |
0.82 ± 0.04 |
0.30 ± 0.05 |
0.97 ± 0.01 |
0.52 ± 0.05 |
0.65 ± 0.04 |
0.54 ± 0.08 |
0.36 ± 0.04 |
0.84 ± 0.04 |
0.99 ± 0.00 |
0.67 ± 0.03 |
|
75 |
29 |
0.81 ± 0.04 |
0.26 ± 0.05 |
0.89 ± 0.03 |
0.49 ± 0.05 |
0.63 ± 0.05 |
0.42 ± 0.07 |
0.31 ± 0.03 |
0.80 ± 0.04 |
0.90 ± 0.04 |
0.61 ± 0.03 |
|
76 |
19 |
0.81 ± 0.06 |
0.37 ± 0.07 |
0.93 ± 0.03 |
0.67 ± 0.07 |
0.64 ± 0.05 |
0.45 ± 0.06 |
0.33 ± 0.05 |
0.84 ± 0.06 |
0.97 ± 0.02 |
0.67 ± 0.04 |
|
77 |
20 |
0.87 ± 0.05 |
0.30 ± 0.07 |
0.89 ± 0.04 |
0.53 ± 0.04 |
0.63 ± 0.06 |
0.46 ± 0.08 |
0.39 ± 0.04 |
0.86 ± 0.05 |
0.97 ± 0.02 |
0.66 ± 0.03 |
|
78 |
20 |
0.82 ± 0.05 |
0.38 ± 0.07 |
0.89 ± 0.04 |
0.64 ± 0.07 |
0.59 ± 0.06 |
0.56 ± 0.10 |
0.38 ± 0.05 |
0.84 ± 0.05 |
0.97 ± 0.02 |
0.67 ± 0.05 |
|
79 |
20 |
0.72 ± 0.07 |
0.21 ± 0.06 |
0.83 ± 0.05 |
0.44 ± 0.07 |
0.55 ± 0.07 |
0.41 ± 0.09 |
0.30 ± 0.05 |
0.73 ± 0.07 |
0.88 ± 0.05 |
0.56 ± 0.06 |
|
80 |
163 |
0.74 ± 0.02 |
0.32 ± 0.02 |
0.85 ± 0.02 |
0.52 ± 0.02 |
0.54 ± 0.02 |
0.39 ± 0.03 |
0.34 ± 0.01 |
0.77 ± 0.02 |
0.94 ± 0.01 |
0.60 ± 0.01 |
Summarizing the above results, we could not find any scientific evidence for changing the age group of older adults because the number of subjects aged over 70 yrs was too small (424 males and 390 females) and showed inconsistent patterns. Even if the age group is subdivided, it is considerably difficult to secure the necessary scientific evidence when setting the KDRIs for the segmented age group. The limitations of this analysis are as follows. First, the number of subjects is too small. Second, it is currently difficult to comprehensively evaluate age-related changes in the physical and morphological functions of older adults, and to understand the scientific basis for estimating nutritional requirements in older adults. Third, there is insufficient evidence to determine truly healthy older people. In the future, it is necessary to reorganize the concept of how “health,” as defined by the KDRIs, is applied to older adults. In particular, although the KDRIs are standards for a healthy population, further research is required to interpret the meaning of “health” in older adults as the absence of disease, which is not realistic due to the characteristics of this population. Nevertheless, this study is meaningful in that it attempts to reconsider the classification of older adults by examining domestic and international data on the elderly and by examining the consumption patterns by age through various statistical analyses.
Go to :


 PDF
PDF Citation
Citation Print
Print



 XML Download
XML Download