

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The change in the texture of solid food by chewing can influence the nutritional status of older individuals by encouraging eating and providing pleasure via the sensory perception of food [1]. The properties of the bolus are crucial for safe swallowing and digestion [2]. Although chewing and swallowing behaviors are controlled by the central nervous system, they can also be affected by internal and external factors, such as impaired dental functions, including loss of natural teeth; weakened muscles; decreased jaw movement, saliva production, and tongue pressure [2345]; age [14]; sex [6]; and textural and other properties of food [2]. Food hardness and dryness can increase the number of chewing cycles (NCs), oral processing time (OPT), and surface electromyographic (sEMG) activity of the masseter and temporalis [1278]. Food texture modification promotes safe oral intake and prevents malnutrition when the modification corresponds to the chewing and swallowing risk severity [8910]. In Japan, the concept of Universal Design Foods (UDF) was established and commercialized. Specifically, it classifies foods into four categories according to their hardness and ease of chewing [8]. Recently, the Japanese government established a new policy on nursing foods called “Smile Care Food” [11]. In South Korea, the Korean Industrial Standard (KS) Certification for “Seniors Friendly Food” was announced in late 2017 and revised in 2020 [12]. The International Dysphagia Diet Standardization Initiative (IDDSI) proposed global standardized terminology and definitions to elucidate the viscosity and/or texture of texture-modified foods [13]. Despite these initiatives, most older adults or their caregivers still experience difficulties in food preparation [14]. The effect of aging on chewing and swallowing has been described using various foods, including steamed rice, rice cakes [915], or meat [16], in sEMG and videofluoroscopic swallowing studies (VFSS). However, chewing patterns are highly individualistic, with strong dependence on oral and sensory feedback. Therefore, a standardized test based on the degree of hardness or other textural properties can provide optimal comparability among individuals and ensure validity and reproducibility [171819]. In this study, we examined whether texture-modified model foods can reduce the difference in chewing and swallowing parameters between community-dwelling healthy older and young individuals.
SUBJECTS AND METHODS
Participants
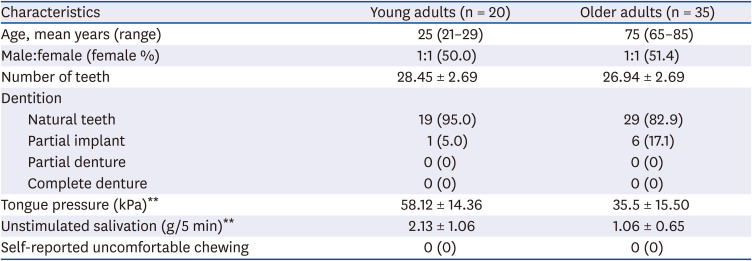
In total, 35 older adults (mean age, 75 years; range, 65–85 years) and 20 young adults (mean age, 25 years; range, 21–29 years) were included. None of them had any severe masticatory dysfunction or significant past medical history that might have influenced their chewing and swallowing function (Table 1). The young group was recruited through advertisements in and around the Chung-Ang University School of Medicine campus. The older adult group was recruited through voluntary participation requests from senior citizen centers located in Dongjak-gu, Seoul, South Korea. Therefore, the older adults who participated in this study represented healthy older adults living in their own homes rather than those living in nursing homes or other special facilities. All participants provided informed consent for the assessment of their masticatory and swallowing kinetics using sEMG and VFSS.
Table 1
Characteristics of participants
This study was approved by the Ethics Committee of the Chung-Ang University Hospital Institutional Review Board (1703-006-00275) and was conducted in accordance with the ethical standards of the Declaration of Helsinki.
Number of teeth and dentition
Chewing performance is greatly affected by dentition [1]. Information regarding dentition, including the number of teeth and dentition of natural teeth, implants, and dentures, was obtained from questionnaires and confirmed via inspection by the researchers. All participants had > 26 teeth, and no mastication or swallowing disorders were observed (Table 1).
Measurement of tongue pressure
Tongue pressure was measured using the Iowa Oral Performance Instrument (IOPI, model 2.1; IOPI Medical LLC, Carnation, WA, USA). Briefly, the tube was placed on the tongue bulb on the maxillary anterior lingual hard palate area, and the participant was asked to press the bulb with their tongue in maximal force for 2 s. Tongue pressure was measured three times with 1-min rest.
Measurement of salivation
The saliva plays a key role in bolus formation. Salivation is induced by food in the oral cavity and is stimulated further by chewing [12]. To investigate the difference in unstimulated salivation between young and old adults, participants were asked to drink water (200 mL) 30 min before starting measurement and then hold a gauze in their mouth. After 5 min, the salivary flow amount was calculated by subtracting the initial gauze weight from the final gauze weight.
Preparation of model food
Model food with four levels of hardness was prepared using soy milk according to the standardized criteria for solid food textures by the UDF [12] and KS [13]. Briefly, the model food was prepared with different ratios of gelling agents (gellan and locust bean gum). Subsequently, gluco-delta lactone was added to soy milk at 80°C and mixed well for 10 min. It was then left at 24°C for 1 h to cool and hardened at 4°C for 24 h to prepare gels with the same dimensions. The formulations of the gelling agents used in the model food are described in Table 2. As shown in Table 2, when participants consumed model food, they were also asked to record the actual foods that they considered the most similar to the model food. The first (highest hardness), second, third, and fourth levels of the model food comprised raw chestnuts, tofu or steamed chestnuts, boiled, soft radish, and buckwheat jelly or soft tofu, respectively. The first, second, third, and fourth levels of the model food were similar to the IDDSI levels 7, 6, 5, and 4, respectively [13].
Table 2
Level of hardness of model food and references
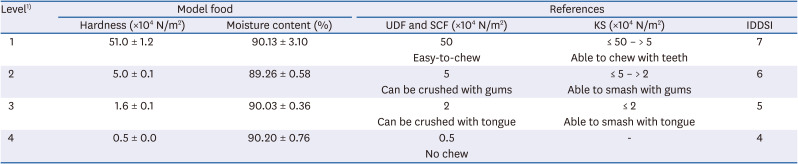
Values are presented as the mean ± SD.
UDF, Universal Design Foods; SCF, Smile Care Food; KS, Korean Industrial Standard; IDDSI, International Dysphagia Diet Standardization Initiative.
1)Formulations of gelling agents of level 1 (% of gellan gum, locust bean gum, and gluco-delta lactone: 5.605, 0.295, and 0.3, respectively), level 2 (% of gellan gum, locust bean gum, and gluco-delta lactone: 0.665, 0.285, and 0.3, respectively), level 3 (% of gellan gum and locust bean gum: 0.630 and 0.270, respectively); and level 4 (% of gellan gum and locust bean gum: 0.476 and 0.204, respectively).
Measurement of properties of model foods
Texture profile analysis was performed using a TAXT-plus Stable Micro Systems Texture analyzer (Stable Micro Systems Ltd., Surrey, UK) according to Bourne's method [20]. Test samples of cubes (16.3 mm height × 76.16 mm width × 76.16 mm length) were prepared from each sample with different hardness levels. A double compression cycle was performed using a cylindrical plunger (diameter: 25 mm) at room temperature. The plunger speed was 10.0 mm/s, and the final deformation was 70% strain. Measurements were performed in triplicate. Hardness was defined as the force at maximum compression during the first compression. The moisture content of the model food was analyzed using JSVO-60T (JSR Corp., Tokyo, Japan).
Measurement of chewing performance
Chewing performance was recorded by attaching pairs of surface electrodes (T246H; Bioprotech, Wonju, Korea) on both the masseter muscles using an sEMG recording system (LXM5308®; Laxtha Inc., Daejeon, Korea) [21]. The mandibular angle and zygomatic bone body were determined by palpation to facilitate electrode placement over the masseter muscle. The point of electrode placement was the midpoint between the lower posterior border of the zygomatic bone and the zygomatic arch, determined by palpation [22]. Further, the electrode position was confirmed by palpation of the masseter belly. A reference electrode was fixed over the frontal bone skin, and a ground strap was connected to the wrist. sEMG signals were recorded on a 16-bit A/D converter board with a frequency of 2048 Hz and digitally filtered at 13–430 Hz. Subsequently, the root mean squares (RMSs) were calculated [23].
One test food cube (2 cm × 2 cm) for each level was provided to participants in random order at ambient temperature. While participants chewed the test samples in an upright seated position, chewing parameters were recorded from the food ingestion point of the oral cavity. To establish comparability among individuals and minimize inter-personal differences, raw data were normalized by the ratio of each RMS of sEMG to the maximal voluntary contraction activity of each participant. Maximal voluntary isometric dental contraction (MVC) was performed in triplicate. MVCs were recorded for 3 s, with 2-min rest between contractions. All data are reported as a percentage of the RMS mean values obtained during MVCs to enable comparison among participants [23].
Measurement of swallowing kinetics
Swallowing kinetics for each model food among participants were recorded using a VFSS based on a previous study [24] with slight modification. Each participant was seated comfortably and asked to chew and swallow the test foods as usual. Lateral radiographic images were captured using fluoroscopic diagnostic equipment (Collimator type R-50; Shimadzu Co., Kyoto, Japan) while the participants consumed 8 g of model food in an upright seated position. Barium paste (1–2 mL) was spread on each food to enhance its radiopacity. Videofluorographic recordings started when the food touched the lips and continued until the last swallow after complete pharyngeal removal. The transmission voltage of the X-rays was set to a peak of 40-kV, allowing visualization of the soft tissue of the pharyngeal structures. Digital videofluoroscopy data were recorded at 30 frames/s using a digital video capture device. A 24-mm diameter coin was taped under the chin, at the midline, as a reference length scale for radiographic magnification.
The video files were analyzed using digital image processing software (ImageJ; U.S. National Institutes of Health, Bethesda, MD, USA) [24]. The anterior–superior margin of the hyoid bone, epiglottis base-to-tip margin, and the bolus head were digitally coordinated in each frame, and the mental protuberance was in the resting position frame. To determine the coordinates for each point, the Y-axis was defined as a straight line connecting the anterior–inferior border of the fourth cervical vertebra (“zero” point) to the anterior–inferior border of the second cervical vertebra; the X-axis was a straight line perpendicular to the Y-axis crossing the “zero” point. Data were selected unanimously by three researchers, a dysphagia expert, and a VFSS procedure interpretation specialist.
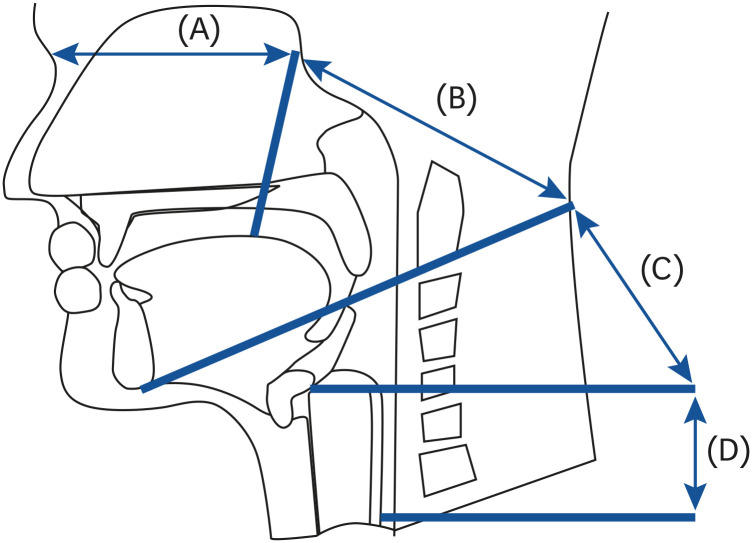
The NCs was measured until just before the start of swallowing. Sequential parameters of bolus transit are classified in Fig. 1, based on previous studies [924]—(a) the interval began with food entry in the oral cavity and ended when the leading edge of the bolus reached the posterior nasal spine (OPT); (b) the leading edge of the forming bolus passed through the pillars of the fauces before initiation of swallowing and then reached lower mandible border (post-faucial aggregation time); (c) the leading edge passed through the lower mandible border and then reached the valleculae (vallecula aggregation time, VAT); and (d) the time elapsed from the moment when the leading edge of the bolus left the valleculae to the time when the trailing edge entered the esophagus (hypopharyngeal transit time). The first subsequence duration (FSD) was defined as the total duration of the (a)–(d) sequence. The second subsequence duration (S–S2) was defined as repeated swallowing times when complete swallowing was not achieved with the first swallow. The total ingestion duration (TD) was defined as the time period from the time when the food reached the oral cavity to the end of complete swallow.
Statistical analysis
Data are presented as means and standard deviations. Data normality was confirmed using the Shapiro–Wilk test prior to statistical analysis of parametric data. Comparison of means between the young and older adult groups was performed using Student's t-test. Analysis of variance and Duncan correction were performed to compare the mastication values and swallowing parameters among the hardness levels of model foods at a significance level of α = 0.05. We used analysis of covariance (ANCOVA) with fixed factors of mastication and swallowing parameters as well as covariates of salivation and tongue pressure that were corrected to avoid affecting the results. Data were analyzed using Statistical Package for the Social Sciences version 18.0 (IBM Inc., Armonk, NY, USA).
RESULTS
Difference in factors affecting chewing function between the age groups
The sex ratio was equally distributed among the age group (Table 1). Differences in the number of teeth and dentition between the age groups were not found. Particularly, 95% and 82.9% participants in the young and older adult groups, respectively, had natural teeth; the remaining 5% and 17.1% participants in the young and older groups, respectively, had partial implants; none had dentures. The mean tongue pressure of the older participants was 35.5 kPa. This was greater than the value of 30 kPa proposed as the maximum cutoff criterion for oral function deterioration in older adults by the Japanese Society of Gerontology. Significant differences were observed in the average tongue pressure and unstimulated salivation between young and old adults (P < 0.001). The average tongue pressure and unstimulated salivation among older adults were 61% and 49.7%, respectively, of the corresponding values observed in young adults.
There was no significant difference in the moisture content of the model food according to the hardness level (Table 2).
Difference in chewing characteristics according to the food hardness level between the age groups
The normalized maximum peak amplitude (MPA) of the masseter muscle was significantly (P < 0.05) higher in the older adult group than in the young adult group, except that of the hardest food model (Fig. 2A). NC was clearly (P < 0.05) greater in the older adult group than in the young adult group, regardless of food hardness (Fig. 2B). However, the age effect on OPT did not exist for levels 2–4; it existed only for the hardest food (Fig. 2C).
Fig. 2
Differences in chewing parameters between young and older adults according to food hardness. (A) MPA; (B) NC; (C) OPT. Different letters a-c or A-C above a bar indicate statistically differences among the level of food hardness on the post hoc Duncan test within a group of participants.
MPA, normalized maximum peak amplitude; NC, number of chewing cycle; OPT, oral processing time.
*P < 0.05.

Difference in swallowing kinetics according to the level of food hardness between the age groups
A significant difference in swallowing kinetics was observed between the young and older adult groups, as shown in Fig. 3. VAT was very short in the young adult group; however, the older adult group always needed much more time to transit each bolus than the young adult group (Fig. 3A, P < 0.05). A significant age effect was measured according to the VAT (P < 0.05) for each food level, although there was great variation among individuals in the older adult group.
Fig. 3
Differences in swallowing behaviors between young and older adults according to food hardness. (A) VAT; (B) FSD; (C) S–S2; (D) TD. Different letters a-b or A-B above a bar indicate statistically differences among the level of food hardness on the post hoc Duncan test within a group of participants.
VAT, vallecula aggregation time; FSD, first subsequence duration; S–S2, second subsequence duration; TD, total duration of intake.
*P < 0.05.

Moreover, there was a significant difference in FSD according to age when eating relatively harder foods (levels 1 and 2) (Fig. 3B, P < 0.05); however, there was no difference in FSD when eating relatively softer foods (levels 3 and 4).
S–S2 also increased in the older adult group compared to that in the young adult group, although the difference was not significant (Fig. 3C), which could be attributed to the great variation observed among individuals in the older adult group.
The effect of age on the TD of food intake was significant (P < 0.05), regardless of food hardness (Fig. 3D).
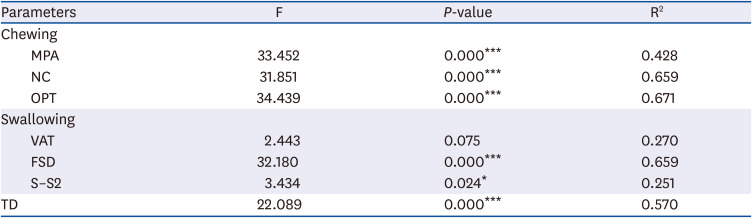
In the older adult group, the unstimulated salivation and tongue pressure were significantly lower than those in young adults (Table 1). Therefore, we checked whether there was a difference in chewing and swallowing parameters according to the food hardness level. After controlling for the salivation and tongue pressure effect in the older adult group, chewing and swallowing parameters, including MPA, NC, OPT, FSD, and TD, were significantly associated with the food hardness level (ANCOVA, P < 0.05) (Table 3).
Table 3
Relations between chewing and swallowing parameters and the level of food hardness after controlling unstimulated salivation and tongue pressure in older adults
DISCUSSION
In our study, the effects of food hardness on chewing parameters were well differentiated by masseter muscle activity. The older adult group used relatively more muscle force during chewing than the young adult group, suggested reduced muscular strength and a reduced functional reservoir. Moreover, the difference in masseter muscle activity between the age groups was maintained even when consuming food with the lowest level of hardness. According to the 2015 Korea National Health and Nutrition Examination Survey (KNHNES) study, 43.3% of the Korean older adult population complained of inconvenience in chewing [25], and the risk of inadequate dietary intake and malnutrition increased with increasing age. Although the older adults who participated in KNHNES study were healthy and had no subjective chewing discomfort, the effect of aging on chewing muscle activity was evident [26]. Tomography observation was performed in previous studies to examine the effect of aging on bite force. The results revealed a serious chewing impairment in older adults because of a decrease in the muscular cross-sectional area [2728]. A strong age effect on chewing pattern, originating from the loss of muscle activity, has also been reported [1829]. In our study, when participants masticated food with the highest level of hardness, there was no significant difference in normalized masseter muscle activities between the age groups; however, the NC was considerably higher and the OPT was much longer in the older adult group. Moreover, the chewing duration increased regardless of the food type, which can be considered an adaptive or compensatory behavior developed to overcome small but consistent muscular weakness; this finding is in line with previous reports [192930]. Although food bolus properties were not examined, significantly fewer comminuted boli have been reported in older adults than in young adults [31].
The consistently higher proportional activation of the masseter muscle in the older adult group than in the young adult group can be explained by the reduction in sensitivity to changes in the food hardness level. Young adults can more precisely control masseter muscle activity depending on the food hardness level, while older individuals are unable to differentiate between these levels and, thus, have increased relative masseter activity or increased variability irrespective of the hardness level of the consumed food. To better understand this phenomenon, it is necessary to further analyze whether older adults can perceive and express the textural differences among the four hardness levels in sensory evaluation. Therefore, food texture perception and acceptability may be affected by texture and other factors, such as moisture content, smell, palatability, and preference. However, another study found that texture perception was relatively stable with age, and texture was an important sensory property of food, along with scent and taste [32]. As there was no difference in scent and taste among the standard model food in this study, it can be inferred that the sensitivity to food texture changes was lower in the older adult group than in the young adult group.
Chewing and swallowing are closely related, and simultaneous assessment is important to understand the effect of food texture on eating behavior. Changes in swallowing physiology with aging are predisposing factors for dysphagia in older adults [4]. Swallowing difficulties among older adults were demonstrated by the significant increase in VAT in the pharyngeal phase, although it was not proportional to food hardness. Similar to our results, previous studies have shown that food hardness increases the OPT, which significantly extends the total swallowing time in young [33] and older adults [9]. In contrast to our results regarding the effect of food texture on the pharyngeal phase, one study [34] asserted that pharyngeal bolus transit is not dependent on food hardness, but rather on its viscosity. Swallowing difficulties with advancing age can negatively impact the effective and efficient flow of the food bolus through the upper aerodigestive tract. The prevalence of dysphagia has been reported to be 37.6% in community-dwelling adults aged 65–94 years; among them, 5.2% reported using a feeding tube at some point in life and 12.9% reported the use of nutritional supplements to achieve adequate daily caloric intake [4].
All participants in our study had an average of >26 of 32 permanent teeth. This number is relatively high for older adults aged 65–85 years, considering that a recent cross-sectional survey [35] reported that the average number of teeth required to eat all kinds of food was at least 20. Additionally, a US survey conducted among individuals aged 65–69 years found that the participants had only 18 teeth remaining on average [36]. There were no significant differences in the number of teeth between the age groups in our study.
Nevertheless, in our study, tongue pressure and unstimulated salivation in the older adult group were almost half of those observed in the young adult group. The most important characteristics of the tongue that are required for the chewing process are the positioning, perception of consistency and particle size, and supporting the changeover from left to right.
Sufficient salivary production is indispensable for good chewing. During chewing, the saliva lubricates food, helping to form a bolus before swallowing. The optimal NC to swallow is dependent on the amount of saliva produced [1]. Moreover, the saliva plays an important role in recognizing the taste and flavor of the food matrix. In our study, even after controlling for the effects of saliva secretion and tongue pressure, food hardness affected chewing and swallowing parameters, such as normalized MPA, NC, OPT, first and second subsequence duration, and TD of food intake.
There are some limitations to our study. First, this was a cross-sectional study, and there were large variations between individuals’ chewing and swallowing behaviors. Second, the number of participants was not equal in each age group. In general, the health and physical condition of older adults is more individual than that of young adults. In addition, there were limitations in the selection of study subjects in terms of cost and participation rate; therefore, a larger number of older adults was included in the study according to previous studies [19]. Third, we did not directly compare bolus properties, including the size of particles, between the age groups, which may explain the large variances observed between the participants [30].
However, the model foods used in this study were of the same size and shape and differed only in texture characteristics; this can be used as a strategy for reproducibility and reliability to understand the differences in chewing and swallowing behaviors between different age groups. As the size or shape of food samples in previous studies varied, it might have affected the masticatory duration and NC of individuals [2830]. The sex-matched study design allowed us to exclude differences in chewing habits observed between men and women, as reported previously [6]. To our knowledge, this is the first study to examine whether texture-modified model foods can reduce the difference in chewing and swallowing parameters between community-living healthy older adults and young adults in South Korea.
In conclusion, our results confirmed that there are clearly measurable differences in the process of chewing and swallowing food between young and older adults. In particular, although older adults had a sufficient number of teeth to eat food without chewing problems, there was a difference in the process of chewing and swallowing. Moreover, the differences between the age groups could decrease when food hardness is relatively low. The latter indicates that changes in chewing can be observed in older patients before diagnostic pathology. However, any sudden change in the health status of older individuals could have dramatic effects on the ability to chew, and there may be a need for diet modifications to maintain nutrition and prevent weight loss. Therefore, community-dwelling healthy older adults may need preventive efforts to promote good nutrition by adjusting food hardness.
 XML Download
XML Download