

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The Global Burden of Disease 2016 Study reported that cardiovascular diseases (CVDs) are the leading causes of global years of life lost.1 Since ischemic heart disease is projected to be the leading cause of mortality by 2040,2 CVDs are expected to become more problematic. In the United States (US), nearly half of adults have CVD, and around one in every four people die from it.3 In Korea, CVD is the second largest cause of death following cancer.4
Unhealthy lifestyle behaviors such as cigarette smoking, alcohol consumption, obesity, poor diet, and lack of exercise are widely recognized to impact blood pressure, fasting glucose levels, cholesterol levels, and metabolic syndrome (MetS), all of which are risks factors for CVDs.56789 These conditions are referred to as cardiometabolic disorders (CMDs), which are related to an increased risk of CVDs.10 In addition, a combination of these conditions multiplicatively raises the risk of death from any cause and CVD.1112 The aging population and westernized lifestyle in Korea have increased the prevalence of CMDs.1314151617 As a result, estimating the prevalence of CMDs in a nationally representative population can be an important indicator to forecast the future CVD mortality risk in Korea.
Previous studies have primarily investigated the prevalence of single or multiple CMDs in each country,1819 but no study has directly compared the prevalence of CMDs and comorbidity in Korea and the US using nationally representative population data. In addition, population-based studies in Korea that examine the prevalence of cardiometabolic comorbidities between urban and rural areas have been scarce.
Therefore, the aim of this study is to compare the prevalence of CMDs and comorbidities in Korea and the US by analyzing the US National Health and Nutrition Examination Survey (NHANES) and its counterpart in Korea (Korea National Health and Nutrition Examination Survey [KNHANES]). The Korean population will also be subdivided into a large-scale urban cohort study and a rural community cohort to estimate urban-rural inequalities in the prevalence of CMDs.
METHODS
Study population
NHANES
The NHANES is a series of multistage probability surveys designed to be representative of the non-institutionalized population in the US.20 Since 1999, the NHANES has been collecting data in 2-year phases. From 2003 to 2014, we analyzed 15,872 individuals aged 40 to 69 years to estimate the prevalence of hypertension, diabetes mellitus (DM), dyslipidemia (hypercholesterolemia and hypertriglyceridemia), obesity, and MetS.
KNHANES
The KNHANES is a nationally representative cross-sectional survey that collects data on demographic status, lifestyle habits, anthropometric measurements, and clinical profiles.21 The data is collected annually through a health questionnaire and examination done by certified physicians and medical technicians. Individuals aged 40 to 69 years old having the information on height, weight, and blood pressure measurements, blood tests, and usage of antihypertensive and antidiabetic medication recruited between 2007 to 2014 were included in this study.
Korean Genome and Epidemiology study (KoGES)
The Health Examinees-Gem Study (HEXA-G) and the Cardiovascular Disease Association Study (CAVAS) are both large population-based cohorts from the KoGES. The HEXA-G is comprised of urban residents recruited from various urban hospitals and centers between 2004 and 2013, whereas the CAVAS is composed of individuals living in rural regions in Korea from 2005 to 2011. The detailed information of the urban and rural cohorts of KoGES is described previous studies.2223 This study is eligible to 139,345 individuals from HEXA-G and 24,994 individuals from CAVAS who have information on their blood pressure, height, weight, laboratory blood tests, and usage of antihypertensive and antidiabetic medication.
Definition of CMDs
Hypertension
The American College of Cardiology/American Heart Association 2017 guideline for high blood pressure in adults was used to diagnose hypertension in this study.24 According to the guidelines, we classified hypertension as taking antihypertensive medication, having a systolic blood pressure of 130 mmHg or higher, or having a diastolic blood pressure of 80 mmHg or higher.
DM
According to the World Health Organization (WHO) and International Diabetes Federation, DM is taking antidiabetic medication, having a fasting plasma glucose level of 126 mg/dL or more, or having an HbA1C level of 6.5% or above.25 On the other hand, KNHANES defined DM using plasma glucose level after 8 hours of fasting.
Dyslipidemia (hypercholesterolemia and hypertriglyceridemia)
The two kinds of dyslipidemia, hypercholesterolemia and hypertriglyceridemia were classified using the National Cholesterol Education Program’s Adult Treatment Panel III (NCEP-ATP III) standards.26 Total cholesterol of 240 mg/dL or above was regarded as hypercholesterolemia, and a triglyceride (TG) level of 200 mg/dL or above was defined as hypertriglyceridemia.
Obesity
Different body mass index (BMI) cut-offs were used between Asians and Americans based on the WHO obesity standards.27 Obesity was defined as a BMI of 25 kg/m2 or greater in the Korean population and 30 kg/m2 or greater in the US population.
MetS
According to the NCEP-ATP III criteria,26 MetS is defined as having three of the five conditions mentioned below: 1) A blood pressure of 130/85 mmHg or more or taking antihypertensive medications; 2) a fasting glucose level above 100 mg/dL; 3) high-density lipoprotein level lower than 40 mg/dL for men and 50 mg/dL for women; 4) a TG level greater than 150 mg/dL; 5) a waist circumstance of 102 cm or higher for men and 88 cm or higher for women in the US and 90 cm or higher or for men and 85 cm or higher for women in the Korean population.28
Statistical analysis
The NHANES and KNHANES data were analyzed using relevant established survey sample weights. We used the χ2 test for categorical variables and the Student’s t-test for continuous variables to compare the baseline characteristics including lifestyle habits, and self-reported disease history of CVD and cancer across studies. We calculated the age-standardized prevalence with the 95% confidence intervals of hypertension, DM, hypercholesterolemia, hypertriglyceridemia, obesity, MetS, and the comorbidity in each study population. All estimates were based using direct age-standardized approaches29 using the WHO world standard population.30
The age-standardized rate is computed as follow (calculation of direct age-standardized rate):
wi: Number of population in the ith age group of the WHO world standard population.
ai: Age-specific rate in the ith age group.
The prevalence was further subdivided by sex, median survey years of the overall data (before 2010 and after 2010), and age groups (40–49, 50–59, and 60–69). Excess rates were estimated using the KNHANES as the reference group to assess the prevalence differences between the studies. SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA) was used to analyze the data.
RESULTS
Table 1 shows the general characteristics of the study individuals aged 40 to 69 years in the NHANES, KNHANES, HEXA-G, and CAVAS. There were 15,872 individuals in the NHANES, 26,492 in the KNHANES, 139,345 in the HEXA-G, and 24,994 in the CAVAS. The mean age in each study was 54.0, 53.9, 52.7, and 56.5 years old, respectively. The greatest BMI was shown in the NHANES at 29.3 kg/m2, while the lowest was found in the HEXA-G at 23.9 kg/m2. Individuals in the Korean study were less likely to smoke and drink alcohol than individuals in the NHANES, and they were more likely to exercise. The baseline self-reported CVD and cancer history, the prevalence of stroke, myocardial infarction, and was significantly higher in NHANES than in KNHANES and KoGES (Table 1).
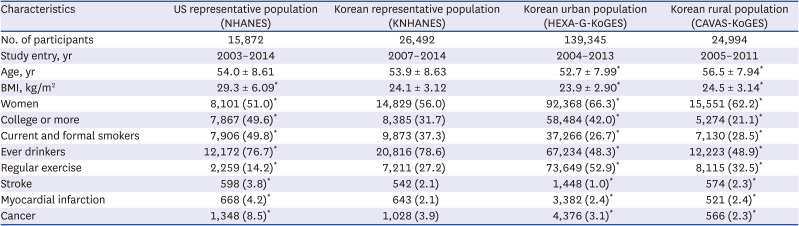
Table 1
Baseline characteristics of the four study groups
NHANES = National Health and Nutrition Examination Survey, KNHANES = Korea National Health and Nutrition Examination Survey, KoGES = Korean Genome and Epidemiology Study, HEXA-G = Health Examinees-Gem Study, CAVAS = Cardiovascular Disease Association Study.
*P < 0.001 for the test for the difference between each group and the KNHANES.
![]()
Prevalence of CMDs
We found that the prevalence of CMDs was higher in US adults and lowest among Koreans living in urban areas. Among the CMDs, hypertension had the greatest age-standardized prevalence, affecting half of the individuals in NHANES (56.8%) and Korea (KNHANES, 49.9%; HEXA-G, 51.0%; CAVAS, 60.3%). Hypertension, obesity, and MetS were more prevalent in the NHANES (56.8%, 38.6%, 36.5%) and CAVAS (60.3%, 40.9%, 33.2%) than in the KNHANES (49.9%, 36.2%, 29.4%). The lowest prevalence of dyslipidemia (hypercholesterolemia 11.3%; hypertriglyceridemia 12.8%), obesity (31.9%), and MetS (18.8%) were shown in the Korean urban population (Table 2).
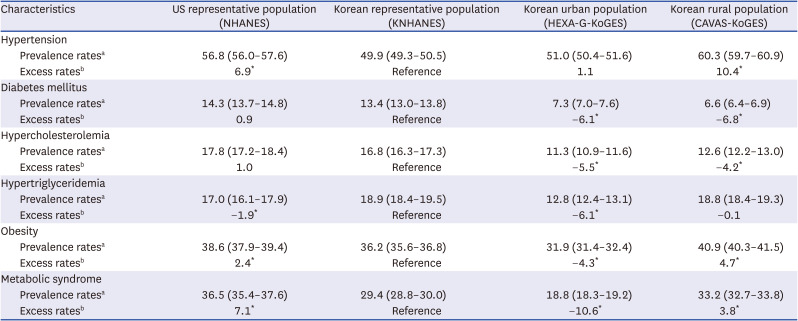
Table 2
ASPRsa of cardiometabolic disorders in the four study groups
ASPR = age-standardized prevalence rate, NHANES =National Health and Nutrition Examination Survey, KNHANES = Korea National Health and Nutrition Examination Survey, KoGES = Korean Genome and Epidemiology Study, HEXA-G = Health Examinees-Gem Study, CAVAS = Cardiovascular Disease Association Study.
aASPRs (per 100 persons) were calculated using the World Health Organization world standard population.
bExcess rates (per 100 persons) were calculated as [(ASPR in each group) − (ASPR in the KNHANES)].
*P < 0.001 for the test for the difference between each group and the KNHANES.
![]()
The sex differences in the age-standardized prevalence of CMDs were similar across the two countries. In both US and Korea, men have a larger prevalence of hypertension, DM, hypertriglyceridemia, and MetS than women, whereas women have a higher prevalence of hypercholesterolemia. Obesity was more prevalent in women than in men in the US, whereas it was more common in men in Korea (Table 3).
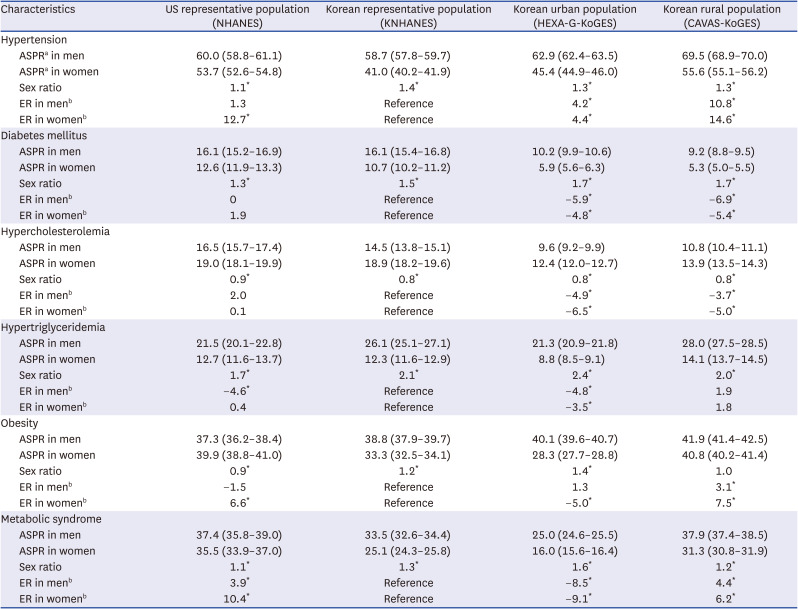
Table 3
Sex-specific ASPRsa of cardiometabolic disorders in the four study groups
ASPR = age-standardized prevalence rate, NHANES = National Health and Nutrition Examination Survey, KNHANES = Korea National Health and Nutrition Examination Survey, KoGES = Korean Genome and Epidemiology Study, HEXA-G = Health Examinees-Gem Study, CAVAS = Cardiovascular Disease Association Study, ER = excess rate.
aASPRs (per 100 persons) were calculated using the World Health Organization world standard population.
bERs (per 100 persons) were calculated as [(ASPR in each group) − (ASPR in the KNHANES)].
*P < 0.001 for the test for the difference between each group and the KNHANES.
![]()
Comparison of the prevalence rates between before and after 2010
According to the median survey years of the overall data from 2003 to 2014, the data was divided into before 2010 (from 2003 to 2009) and after 2010 (from 2010 to 2014). In both Korean and US studies, more than half of the individuals were diagnosed with hypertension after 2010. Individuals living in rural regions in Korea showed a significant decrease in the prevalence of hypertension after 2010 compared to before 2010 (CAVAS, 61.0% vs. 54.1%). We found increasing prevalence of DM in the Korean population (KNHANES, from 11.8% to 14.1%; HEXA-G, from 5.7% to 9.7%; CAVAS, from 6.4% to 8.9%). Individuals in KNHANES had increasing prevalence of hypercholesterolemia (from 13.8% to 18.2%), as opposed to those in NHANES (hypercholesterolemia, from 19.2% to 15.4%; hypertriglyceridemia, from 18.2% to 15.1%). After 2010, the prevalence of hypercholesterolemia and hypertriglyceridemia in KNHAENS (18.2% and 18.9%, respectively) became higher than that in the NHANES (15.4% and 15.1%). The prevalence of obesity increased in the individuals in NHANES (from 37.8% to 40.3%) and CAVAS (from 40.8% to 41.7%), while decreased in KNHANES (from 37.1% to 35.8%) and HEXA-G (from 32.3% to 31.3%). The prevalence of MetS, the prevalence decreased in both US and Korean (NHANES, from 37.1% to 35.5%; KNHANES, from 32.7% to 28.3%; HEXA-G, from 19.4% to 17.8%; CAVAS, from 33.8% to 28.5%) (Table 4 and Supplementary Table 1).
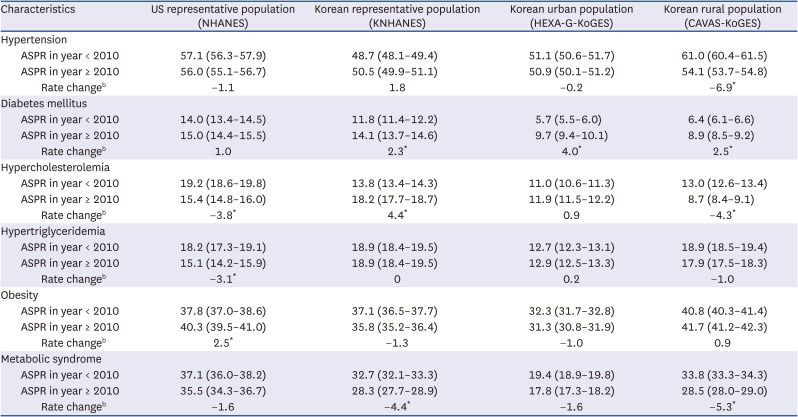
Table 4
ASPRsa of cardiometabolic disorders according to the observational year in the four study groups
NHANES = National Health and Nutrition Examination Survey, KNHANES = Korea National Health and Nutrition Examination Survey, KoGES = Korean Genome and Epidemiology Study, HEXA-G = Health Examinees-Gem Study, CAVAS = Cardiovascular Disease Association Study, ASPR = age-standardized prevalence rate.
aASPR was calculated using World Health Organization world standard population.
bRate change was calculated as [(ASPR in recent year ≥ 2010) − (ASPR in past year < 2010).
*P < 0.001 for the test for the difference between each group and the KNHANES.
![]()
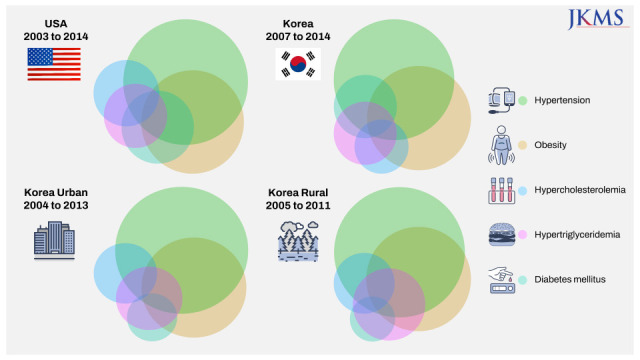
Prevalence of cardiometabolic comorbidity
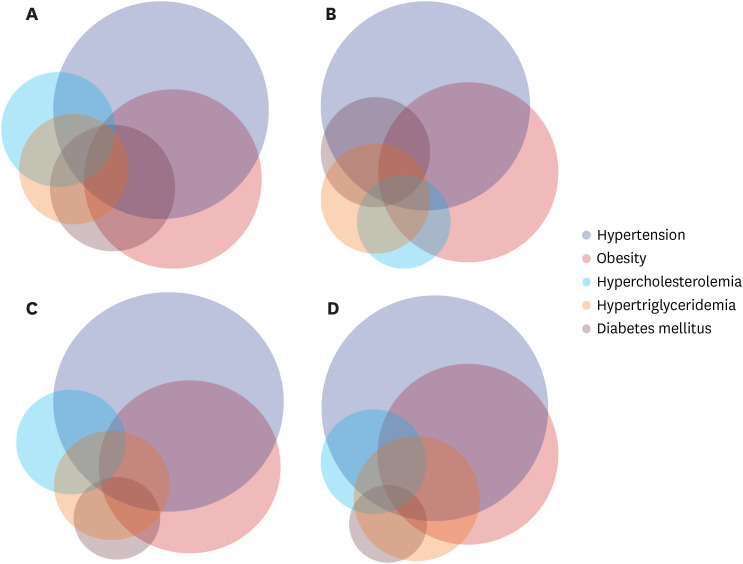
Overall, 24.4%, 29.3%, 30.9%, and 19.5% of individuals in NHANES, KNHANES, HEXA-G, and CAVAS were free of CMDs, respectively. In the KNHANES, 31.1%, 23.2%, 11.8%, and 4.6% had one, two, three, and four disorders, respectively, as opposed to 31.5%, 26.0%, 13.4%, and 4.7% in the NHANES, respectively. Individuals in rural regions were more likely to have a comorbidity than those in urban areas in Korea. In both Korean and US population, the most common combination of comorbidities was hypertension and obesity (Fig. 1 and Supplementary Table 2).
DISCUSSION
Our study found that the Korean population had a lower prevalence of hypertension, obesity, and MetS than the US population. Individuals living in rural areas had the highest prevalence of hypertension, hypertriglyceridemia, obesity, and MetS in Korean population studies. The prevalence rates of hypertension, DM, obesity, and MetS after 2010 in Korea were lower than those in the US population. However, dyslipidemia was more prevalent in Korea than the US. Korea also had a lower prevalence of cardiometabolic comorbidity than the US. Among the Korean population, individuals living in rural areas had the highest prevalence of comorbidity.
Lifestyle behaviors such as cigarette smoking, alcohol consumption, diet, and physical activity are the common triggers for CVDs.313233343536 These poor lifestyle behaviors affect blood pressure, fasting glucose levels, cholesterol levels, and obesity, all of which are intermediate risks factors for CVDs.56789 Hypertension is responsible for approximately 42.7% of coronary heart disease, 38.9% of strokes, and 21.6% of heart failure.37 DM is associated with a 19.5% population attributable risk for stroke and a 3% for coronary heart disease, respectively.38394041 Hypercholesterolemia is accountable for 18% of the risk of coronary heart disease, 31% of the risk of myocardial infarction, and a 21% higher risk of CVD mortality.414243 On the other hand, the relationship between hypertriglyceridemia and the risk of CVD and mortality has been debated.4445 Furthermore, since life expectancy has gradually increased over the last decade, the prevalence of CMDs and comorbidity has risen as well.46 Previous studies have found that having multiple CMDs is associated with a higher risk of total and cardiovascular mortality.1112
CMDs were less prevalent in the Korean population than in the US population. Theses differences might be related to variances in dietary patterns and lifestyle behaviors.47 Due to economic growth and westernization, however, the increased prevalence of CMDs has become a burden on public health in Korea.13141516 Previous studies have investigated the prevalence of CMDs in the US and Korea, respectively;1819 but there were only a few studies that evaluated the difference between the two nations. Comparing the prevalence of CMDs in Korea with the US has important implications for intervention strategies to prevent the risk of CVD mortality in Korea. In this study, we estimated and compared the prevalence of CMDs and comorbidities in the US and Korea using four independent data sources, including data representative of the US and Korea and large-scale urban and rural cohorts in Korea.
We found a significant increase in the prevalence of DM in the Korean population after 2010, which corresponded to the global increase in DM.48 In comparison to the US, Korea had a much greater prevalence of dyslipidemia after 2010. Because dyslipidemia is common in patients with hypertension and DM, the increasing prevalence of hypertension and DM in Korea might be associated with a higher prevalence of dyslipidemia.49 Korea’s carbohydrate-centered diet is another risk factor for dyslipidemia.50 Furthermore, individuals living in rural areas of Korea showed a much higher prevalence of comorbidity than those living in urban areas. This disparity is likely due to their low socioeconomic status, limited access to health care, and unhealthy lifestyle behaviors.515253 Public health program is needed to decrease the excess risk of mortality from CVDs in rural areas of Korea.
There are several strengths in our study. First, we used data from the NHANES and KNHANES, which are nationally representative data of the US and Korea, respectively. Based on the non-institutionalized population dataset, we were able to estimate the age-standardized prevalence of CMDs in both the countries. The large sample size from the KoGES data was another strength of our study. The Korean population was also subdivided into an urban and rural cohort to compare the rural-urban disparities in Korea. To our knowledge, our study was the first to compare the age-standardized prevalence of CMDs and comorbidities in Korea and the US.
This study has several limitations. Misclassification bias can occur due to the differences between each of the studies from study design, and measurement methods. We were unable to classify type 1 or type 2 DM, due to the lack of information in the dataset. Another limitation is that because the datasets we used are based on cross-sectional surveys, we were limited to capturing information from a specific point in time and were unable to examine a cause-and-effect relationship with mortality from CVDs. Further studies on the effects of CMDs on CVD events in nationally representative data will be required.
In conclusion, the comparison of the prevalence of CMDs and comorbidities in Korea and the US suggests that an effective monitoring system and prevention strategies are needed to minimize the risk of CVD events, particularly in rural areas of Korea.
 XML Download
XML Download