

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pneumonia is a leading cause of mortality and morbidity1; its rank has risen from 10th to 3rd in recent decades. In South Korea, pneumonia was 6th most common cause of death in 2010, with 14.9 deaths per 100,000 population, but in 2020, it was the 3rd most common cause of death, and the rate of mortality from pneumonia increased to 43.3 deaths per 100,000 population.2 Attention should be paid to pneumonia in patients with stroke. Pneumonia and urinary tract infection commonly occur after stroke and have a considerable impact on clinical outcome.34 Because of the high mortality rate associated with pneumonia, it is vital to determine strategies to prevent pneumonia in patients with stroke.
As hypertension is the biggest risk factor for stroke, antihypertensives are frequently prescribed to patients with stroke. Associations between the use of antihypertensives, particularly angiotensin converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs), and the risk of pneumonia have been reported in the past 2 decades.567 Despite numerous studies on this topic, the effects of antihypertensives on pneumonia remain controversial. Moreover, no study has been conducted on the effect of antihypertensives on pneumonia in a Korean population.
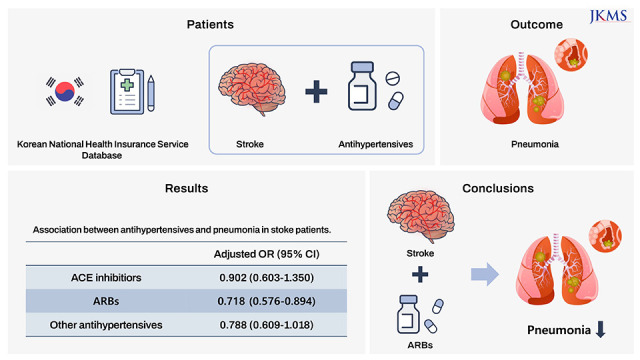
By using a national sample cohort comprising 1 million South Korean individuals, we aimed to assess the association between the use of antihypertensives and the incidence of hospitalized pneumonia in patients with a history of stroke. Additionally, we investigated the effects of antihypertensive use according to age, diabetes mellitus status, and disability. By doing so, we attempted to identify antihypertensives that can help prevent post-stroke hospitalized pneumonia.
METHODS
Data source
We obtained data from the Korean National Health Insurance Service-National Sample Cohort database.8 It contains information from 2002 to 2015 on 1 million South Korean individuals, accounting for 2.2% of the entire population of 50 million. It primarily contains anonymized data on the diagnosis, medications, degree of disability, income (socio-economic variables), and history of hospitalization, including duration of hospitalization, date of admission and discharge, and medical examination findings. The approved database access request ID was REQ000025162-001.
Study design and participants
In this case-crossover study, we included patients aged over 18 years with a diagnosis of ischemic stroke (International Classification of Diseases 10th Revision [ICD-10] codes: I60, I61, I62, I63, and G45), who had been hospitalized due to pneumonia (ICD-10 codes: J12-18) after stroke between 2002 and 2013.
We assessed the association between 3 categories of antihypertensives (ACE inhibitor, ARB, and others) and the incidence of hospitalized pneumonia in stroke survivors. A case-crossover study design is used to evaluate associations of incidences of acute disease and specific exposures. Each patient served as their own control. Thus, confounding factors that could arise from personal characteristics were minimized.9
The date of the first incidence of pneumonia was defined as the “index date.” The case period was defined as the 30-day period before the index date. The status of exposure to antihypertensive drugs in this period was considered to affect the incidence of pneumonia. We defined the 2 control periods as the periods 90–120 days and 150–180 days before the index date. We considered the status of exposure to antihypertensive drugs in the control periods to be irrelevant to the incidence of pneumonia (Fig. 1). Considering the possibility of poor medication adherence, a washout period was included between the case and control periods.
Fig. 1
The case-crossover study design. The case period was defined as 30 days before the index date of first onset pneumonia. Two control periods were defined as 30 days with 30 day intervals, 90 to 120 days and 150 to 180 days before the index date, respectively.

In each participant, we adjusted for confounding factors, including time-varying confounding factors such as the history of exposure to other medications that could affect the incidence of pneumonia and the number of outpatient visits.
Medication history
We investigated the use of ACE inhibitors, ARBs, or other antihypertensives during each case and control period. We classified drug combinations including ACE inhibitors as “ACE inhibitors” and those including ARBs as “ARBs.” Other antihypertensives included calcium channel blockers, alpha blockers, beta blockers, alpha-beta blockers, and diuretics. In addition, we assessed concomitant use of medications such as statins, antipsychotics, and benzodiazepines, which could affect the incidence of pneumonia,1011121314 using the 2019 Korea medication list published by the National Health Insurance Review and Assessment Service (Supplementary Table 1).
Sensitivity and subgroup analyses
To increase the robustness of the study findings, we conducted sensitivity analysis by changing the duration of each period from 30 to 60 days (Fig. 2). This was done because prescription could be delayed in patients who do not regularly use their medication, and this could be misclassified as exposure to the medication. The case period was defined as the 60-day period before the index date. The 2 control periods were defined as the periods 120–180 days and 210–270 days before the index date.
Fig. 2
The sensitivity test design. The time period of the case period and two control periods were changed from 30 days to 60 days.

We conducted subgroup analysis in individuals with a high risk of pneumonia, such as those with diabetes, documented disability due to brain lesions, and age over 65 years. We identified individuals with diabetes based on their ICD-10 codes (E10–14). We used the National Disability Registry System to identify stroke survivors with documented disability due to brain lesions. In South Korea, people with disabilities are registered through their local government as having 1 of 15 types of disabilities. If the severity of disability due to brain lesions such as stroke is high, the patient might be registered in the National Disability Registry System according to the brain lesion rather than the type of disability. Therefore, we classified individuals with severe disability due to brain disorders into a “documented disability” subgroup.
Statistical analyses
We performed conditional logistic regression analysis to estimate the association between antihypertensive use and the incidence of hospitalized pneumonia. Crude odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for the association between pneumonia and ACE inhibitors, ARBs, and other antihypertensives. Following adjustment for confounding factors, we calculated the adjusted OR. Confounding factors included statin, antipsychotic, and benzodiazepine use and outpatient visits. The crude and adjusted ORs were calculated using similar methods in the sensitivity and subgroup analyses. All statistical analyses were conducted using SAS software for Windows (SAS Institute Inc., Cary, NC, USA). A P value < 0.05 was deemed statistically significant.
RESULTS
Risk of hospitalized pneumonia
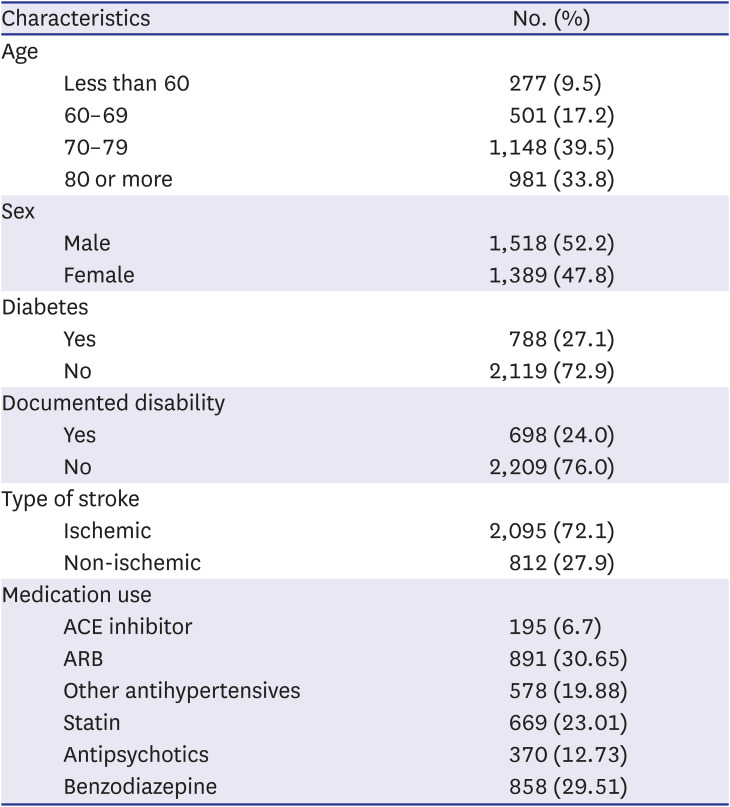
We obtained the data of 2,907 stroke survivors who had been hospitalized for first-onset pneumonia. Table 1 summarizes their general characteristics.
Table 1
General characteristics of the patients with history of stroke (N = 2,907)
The use of ARBs lowered the risk of hospitalized pneumonia (adjusted OR [95% CI]: 0.718 [0.576–0.894]) in the patients with history of stroke. However, the use of ACE inhibitors and other antihypertensives were not associated with a change in the incidence of hospitalized pneumonia (adjusted ORs [95% CIs]: 0.902 [0.603–1.350] for ACE inhibitors and 0.788 [0609–1.018] for other antihypertensive drugs; Table 2).
Table 2
Association between antihypertensives and pneumonia in stroke patients

We obtained similar results in the sensitivity analysis (adjusted ORs [95% CIs]: 0.783 [0.619–0.992] for ARBs, 0.955 [0.635–1.436] for ACE inhibitors, and 0.884 [0.680–1.149] for other antihypertensive drugs; Table 3).

Subgroup analysis
The results of the subgroup analysis are presented in Table 4. In individuals aged > 65 years, a protective effect against hospitalized pneumonia was observed only in those who received ARBs (adjusted ORs [95% CIs]: 0.687 [0.536–0.880] for ARBs, 0.941 [0.596–1.487] for ACE inhibitors, and 0.857 [0.646–1.136] for other antihypertensives). This finding was similar to that of the primary analysis. However, a reduced risk of hospitalized pneumonia in stroke survivors with diabetes mellitus was not noted for any type of antihypertensive (adjusted ORs [95% CIs]: 0.707 [0.481–1.040] for ARBs, 0.920 [0.460–1.840] for ACE inhibitors, and 0.864 [0.549–1.360] for other antihypertensives) and those with documented disability (adjusted ORs [95% CIs]: 0.841 [0.538–1.317] for ARBs, 1.410 [0.571–3.481] for ACE inhibitors, and 0.581 [0.334–1.011] for other antihypertensives).
Table 4
Subgroup analysis between antihypertensives and pneumonia in people with diabetes, documented disability, and over 65 years old
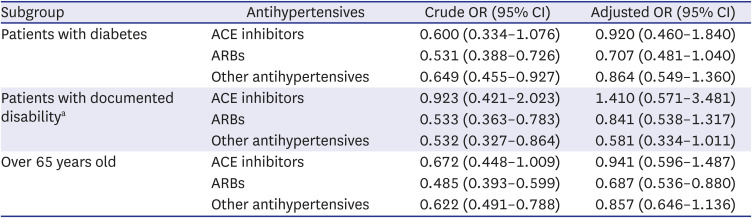
Adjusted for ACE inhibitor, ARB, other antihypertensives, statin, antipsychotics, benzodiazepine, and outpatient visits.
ACE = angiotensin-converting enzyme, ARB = angiotensin II receptor blockers, OR = odds ratio, CI = confidence interval.
aPatients registered for National Disability Registry System were classified as “documented disability” group.
DISCUSSION
The use of ARBs was associated with a reduced incidence of hospitalized pneumonia in patients with a history of stroke, while the use of ACE inhibitors and other antihypertensives did not exert any effect. Similar results were obtained in stroke survivors aged over 65 years. However, none of the antihypertensives reduced the risk of hospitalized pneumonia in stroke survivors with diabetes and documented disability. ARBs are commonly prescribed to patients with hypertension and cardiovascular diseases. They have been reported to have greater protective effects on pneumonia or lung injury than ACE inhibitors,15161718 which is consistent with our results. The exact mechanism remains unclear. However, the following mechanisms have been suggested for the effects of ACE inhibitors and ARBs in preventing pneumonia: ACE inhibitors act by blocking the conversion of angiotensin I to angiotensin II. This in turn inhibits the breakdown of bradykinin and substance P into inactive peptides, and elevated concentrations of bradykinin and substance P reportedly promote coughing and facilitate the swallowing reflex.1019202122 In addition, ACE inhibitors and ARBs affect the renin-angiotensin system (RAS), which plays a major role in inflammation.2324 The protective effect of ARBs could be explained by their role in the modulation of the inflammatory response via RAS blockade.17 Angiotensin II increases vascular permeability and promotes the production of inflammatory molecules and recruitment of leukocytes. ARBs block these actions, resulting in improvement in inflammatory or infectious lung conditions.25 Kim et al.17 and Lai et al.18 reported an association between ARB and a decreased incidence of pneumonia in patients with chronic obstructive pulmonary disease (COPD). This decreased incidence could be due to blockage of the renin-angiotensin system, which induces the release of inflammatory cytokines, or due to immunomodulation of the T-cell responses that mediate lung injury in COPD. Attenuation of bleomycin-induced pulmonary fibrosis via a decrease in the concentrations of inflammatory agents following ARB administration has been reported in mice.26 The protective effect of ARBs on pneumonia in stroke survivors could be explained by its anti-inflammatory effect on the lung.
However, subgroup analysis revealed different results from the primary analysis. ARBs did not reduce the incidence of pneumonia in patients with diabetes and documented disability. Diabetes is a risk factor for pneumonia requiring hospitalization.27 This can be attributed to the negative effect of hyperglycemia on innate immunity; hyperglycemia eventually leads to inflammation and provides a conducive environment for pathogens because of glucose secretion in the airways.2829 Stroke survivors with documented disability have severe disability, and they are likely to have several risk factors for pneumonia, including dysphagia, cognitive impairment, or loss of consciousness. These results imply that the protective effect of ARBs might be decreased in patients with stroke who have a high risk of pneumonia.
As observed in the subgroup analysis, several studies have reported differences in the protective effects of antihypertensives depending on the population groups. Two case-crossover studies conducted in Taiwan using data from the Taiwanese Longitudinal Health Insurance Database reported that the use of ACE inhibitors and ARBs did not reduce the risk of pneumonia in the general population.30 However, ACE inhibitors have been found to exert significant protective effects against pneumonia requiring hospitalization in stroke survivors.5 Likewise, van de Garde et al. reported that the use of ACE inhibitors was not beneficial for reducing pneumonia in the general White population,31 but it exhibited a protective effect against pneumonia in patients with diabetes.27 Lee at al.24 reported that the hazard ratio of ARBs in patients with hospitalized pneumonia in the general population is 0.853 (0.820–0.887), but this potential beneficial effect was not observed in patients with coronavirus disease 2019.
In our study, the use of ACE inhibitors was not associated with a reduced incidence of hospitalized pneumonia in patients with stroke. Several studies have reported beneficial effects of ACE inhibitors on the risk of pneumonia in stroke survivors, which is inconsistent with our findings. A systematic review and meta-analysis of 18 randomized controlled trials, 11 cohort studies, 2 nested case-control studies, and 6 case-control studies of patients with a history of stroke reported that ACE inhibitors reduced the risk of pneumonia by 34% (OR, 0.66).7 In contrast, a randomized controlled trial showed that the use of ACE inhibitors increased the incidence of pneumonia in patients with neurologic dysphagia6; tube-fed patients with neurologic dysphagia allocated to the lisinopril group (2.5 mg daily) (n = 38) and placebo group (n = 33) were compared, and the treatment group was found to have a higher 6-month mortality and probability of pneumonia or death than the placebo group. Therefore, further investigation is needed to identify factors that can reduce the incidence of pneumonia.
According to the results of previous studies and our study, the use of ARBs or ACE inhibitors cannot reduce the risk of pneumonia in healthy individuals or those with a high degree of comorbidity, but they could exhibit a protective effect in patients with a minor degree of comorbidity.15630323334 However, the results differ from study to study.
This study has several limitations. First, we only included patients with pneumonia who required hospitalization and excluded those who were treated on an outpatient basis. Thus, patients with stroke who had atypical pneumonia, which can be treated in an outpatient clinic, were not included. In addition, we could not determine whether the patients were vaccinated against pneumonia and the cause of the pneumonia, such as community-acquired pneumonia, aspiration pneumonia, ventilator-associated pneumonia, or bacterial or viral pneumonia. Third, we did not consider the use of corticosteroids or immune-suppressants as confounding factors, although these factors could increase the incidence of pneumonia. Nevertheless, this was the first study to show an association between antihypertensive use and the incidence of hospitalized pneumonia using data from a Korean national database of stroke survivors.
In conclusion, the use of ARBs was associated with a reduced incidence of hospitalized pneumonia in Korean patients with history of stroke. However, there was no significant preventive effect in patients with severe post-stroke disability. Further large-scale studies on healthy individuals are needed to investigate the relationship between antihypertensive use and the incidence of pneumonia.
 XML Download
XML Download