

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Rapid industrialization and urbanization have brought about worldwide changes in dietary patterns and diet behaviors and have resulted in a significant phenomenon over the past decades [12]. Eating out has become a common feature of dietary patterns in many countries [12]. In Korea, it was recently reported that approximately one in 3 adults consumed their meals outside the home and that the rate of eating out continues to increase steadily [3]. The restaurant industry, which provides away-from-home foods, has reported an increase in total sales from approximately 39 billion dollars (47,917 billion won) in 2007 to nearly 87.4 billion dollars (107,483 billion won) in 2017, according to nationally representative Korean survey data [4]. Particularly, sales by the institutional foodservice industry have quadrupled from nearly 1.9 billion dollars (2,395 billion won) to approximately 7.7 billion dollars (9,509 billion won) during the same time period [4]. Institutional foodservice in Korea is legally defined as the organizational act of continuously providing meals to a specific majority without the purpose of profit. This is part of a service that assists organizations such as schools, industries, hospitals, and social welfare facilities in achieving their stated objectives. This differs from restaurants or cafeterias that provide food to people for commercial purposes. More than 25% of Koreans reported that they use institutional foodservices for their meals every day [5]. The workplace foodservice category has the second highest proportion of customers among the users of institutional foodservices in Korea [5].
Nutrition is an essential factor that influences health and well-being. A poor dietary pattern has been shown to be one of the primary underlying factors for the increasing prevalence of obesity and other related non-communicable diseases, such as cardiovascular disease and diabetes. Such diseases are the leading causes of mortality and public health concerns worldwide [67]. A healthy diet can assist people in reducing the risks of diet-related chronic diseases and can improve their quality of life, work efficiency, and economic productivity [67].
Most workers spend a significant amount of time at the workplace, which affects their dietary behavior directly or indirectly [68910]. Workplace health promotion interventions, such as dietary education, have been reported to have a positive effect on workers' dietary intake [1112]. However, studies that have compared institutional and commercial meals among workers have focused on a partial meal type, and no studies have compared the nutritional quality of workplace foodservice meals with that of homemade meals and/or meals sourced externally (“eating out”) in Korean workers, using a large, nationwide sample [13].
Therefore, we aimed to compare the nutrient intake according to the source of meals and to determine the association between workplace foodservice use and nutritional quality in Korean adult workers.
Go to : 
SUBJECTS AND METHODS
Ethics disclosure
This study was conducted in accordance with the guidelines laid down in the Declaration of Helsinki of 1975, as revised in 2013. All procedures involving human subjects were approved by the institutional review board of the Korea Centers for Disease Control and Prevention (2018-0103-PA). Written informed consent was obtained from all participants.
Data source and study participants
The Korea National Health and Nutrition Examination Survey (KNHANES) is a nationwide survey on the nutritional and health status of a representative Korean population [14]. The present study was based on data collected from the KNHANES 2016–2018.
Participants were workers aged between 20 and 64 years who completed a health interview, physical examination, laboratory tests, and a nutrition survey. Pregnant participants, those with a history of cancer, thyroid disease, and chronic kidney disease, and those treated for tuberculosis were excluded considering potential unexpected dietary patterns and nutritional requirements. Participants who reported total energy intake implausibly (< 500 kcal/day or > 4,000 kcal/day) were also excluded for the reliability of the analyses.
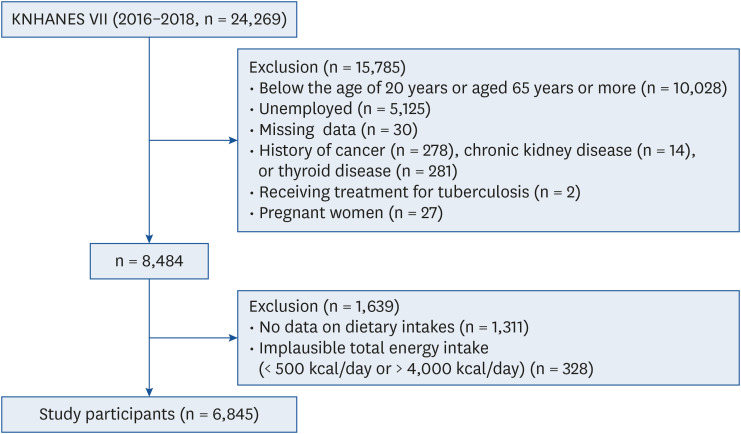
A total of 31,689 (10,806 in 2016; 10,430 in 2017; and 10,453 in 2018) Korean men and women were selected from the KNHANES VII (2016–2018) through a 2-stage stratified complex sampling method. Of these, 24,269 (8,150 in 2016; 8,127 in 2017; and 7,992 in 2018) participants who had completed health interviews, health examinations, and nutrition surveys were included. We excluded the following participants: 10,028 individuals aged < 20 years or > 65 years; 5,125 who were unemployed; 30 with missing data; 573 people with one of the following: cancer history (n = 278), thyroid disease (n = 281), or chronic kidney disease (n = 14); 2 who were treated for tuberculosis, 27 pregnant women; 1,311 who were missing their dietary intake record; and 328 individuals with an implausible reported total energy intake (< 500 kcal/d or > 4,000 kcal/d). This study included 6,845 Korean workers (Fig. 1).
Dietary behavior and nutritional assessment
A survey on dietary behavior and nutrition was conducted by professional interviewers using the 24-h dietary recall method. The interview team comprised dietitians who were acquainted with the protocols for the survey. Data for all foods and beverages consumed by the participants during the previous day were collected [15]. We classified the individuals into weekday and weekend groups according to the day of the dietary survey. The participants' dietary intakes were surveyed for each meal type, eating location, whether they purchased it, and the name and amount of food intake. The eating location was distinguished among the following options: home (household), workplace, restaurants (where food is prepared and sold), other (in the car, on the street, and so on), do not know/reject response, and not applicable (skip meals). Whether or not a meal was purchased was identified as follows: home-cooked meals; restaurant meals (including take-out or delivered meals regardless of where it was eaten), individual food (such as bread and snacks), foodservice meals (made to provide meals to specific people in certain places, such as workplace); convenience foods (a complete cooked food or something that can be eaten with minimal cooking); do not know/reject response; and not applicable (skip meals). Participants were further categorized into 3 groups based on the source of the meals they consumed: (1) the workplace foodservice group was defined as participants who consumed meals that were sourced from a workplace foodservice; (2) the eating-out meal group included those who consumed commercially prepared meals, such as restaurant meals, and convenience foods; and (3) the homemade meal group included those who consumed home-cooked meals, including lunch boxes prepared by relatives or neighbors and individual foods.
The total daily energy, nutrient intake, and intake at each meal were calculated from the collected data using a standard Korean food composition table [16]. Nutritional quality was evaluated using the index of nutritional quality (INQ) based on the nutrient density of the diets. Nutrient density was expressed as the amount of each nutrient per 1,000 kcal. We calculated the intake of each nutrient, including protein, fiber, calcium, potassium, iron, and vitamins A, B1, B2, B3, and C, as a ratio of the nutrient density of the actual food intake by the recommended nutrient intake or adequate intake (AI) from the dietary reference intakes for Koreans of the nutrient per 1,000 kcal according to age and sex [1718]. A nutrient ratio ≥ 1.0 indicated sufficient nutritional intake, whereas a value < 1.0 indicated insufficient nutritional intake. The total number of insufficiently consumed nutrients, among all 10 nutrients, was defined as the INQ score in this study. Therefore, the score ranged from 0 to 10, with a lower INQ score indicating higher nutritional quality.
Socio-demographic and health-related covariates
Information on participants' sociodemographic factors, including age, sex, marital status, household income, and occupation, was obtained through self-reported questionnaires or through face-to-face interviews. Couples who were married or who lived together were both defined as “married” for the purpose of this study. A higher educational level was designated when the participant had received at least one college degree. Based on occupation, individuals were classified into the following groups: service or sales workers, non-manual workers (professionals, general managers, and office workers), manual workers (skilled agricultural, fishery, and forestry workers, machine and plant operators or assemblers, craft and related trade workers, and simple laborers).
The health-related behaviors evaluated in this study included alcohol use, cigarette smoking, and physical activity. Men consuming 7 or more drinks and women consuming 5 or more drinks at least twice a week were considered heavy drinkers. Participants who had smoked ≥ 100 cigarettes in their lifetime and smoked at the time of the survey were defined as current smokers. Adequate physical activity was defined as moderate-intensity activity for at least 150 min, vigorous-intensity activity for at least 75 min during the week, or an equivalent combination of moderate- and vigorous-intensity activities [1920].
Health examinations, including anthropometry, blood pressure measurements, and laboratory blood analysis, were performed by trained medical personnel according to standardized protocols. All pieces of equipment were calibrated regularly. Height and body weight were measured with participants dressed in minimal clothing. Body mass index of < 18.5 kg/m2 and ≥ 25 kg/m2 were regarded as underweight and obese, respectively. A standard sphygmomanometer was used to measure blood pressure after a 5-min rest in a seated position (Baumanometer® Wall Unit 33 [0850]; W.A. Baum Co. Inc., Copiague, NY, USA). Venous blood samples were obtained for blood glucose and lipid profile measurements after 12 h of fasting. Chronic diseases were defined based on data from the participants' health examinations and self-reported medication history in this study. Chronic conditions were defined using the following criteria: hypertension, increased blood pressure (systolic ≥ 140 mmHg or diastolic ≥ 90 mmHg) or medication use for hypertension; diabetes, blood glucose concentration ≥ 126 mg/dL in fasting, a self-reported history of being diagnosed by a health professional, or receiving treatment for diabetes; and dyslipidemia, total cholesterol concentration ≥ 240 mg/dL or serum triglyceride concentration ≥ 200 mg/dL of blood samples in fasting or medication use for dyslipidemia.
Statistical analyses
Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA). Sample weights assigned to participants' data for analysis were used to arrive at estimates representative of the Korean population for the survey period. A multistage stratified and clustered randomized sampling method was used according to the National Census data [14].
Participants were categorized into 2 groups according to the consumption of workplace foodservice meals at least once daily, and the participants' characteristics were compared. Data were analyzed using weighted t-tests or weighted χ2 tests and are presented as mean values for continuous variables and as weighted percentages for categorical variables with standard errors. Nutrient intake and INQ scores were analyzed using a weighted analysis of variance according to the source of meals. The INQ scores based on the total meals consumed in 1-day were further compared among the participants using a weighted linear regression analysis according to the frequency of using workplace foodservices. Multivariate linear regression was used to determine any separate associations between each potential independent variable and INQ scores after adjusting for other covariates. Statistical significance was set at P ≤ 0.05.
Go to :
RESULTS
Baseline characteristics of the study participants
In total, 6,845 workers with complete data were included in this study. The average age was 44.6 years, and 58.5% of participants were men. Overall, 16.8% of the participants used workplace foodservices for their meals at least once a day. Table 1 shows the baseline characteristics of the participants according to workplace foodservice use. Compared with workers who did not use workplace foodservices for their meals, those who consumed at least one workplace foodservice meal in a day were younger, more likely to be men, had a higher household income, were highly educated, were more likely to be underweight, were less likely to have obesity, and had a lower prevalence of diabetes. Current smoking (P = 0.84) and heavy alcohol consumption (P = 0.06) were not significantly different between users and non-users of workplace foodservices. No other variables differed significantly between the 2 groups. The percentages of participants who skipped meals were compared between users and non-users of workplace foodservices for each type of meal (Table 1).
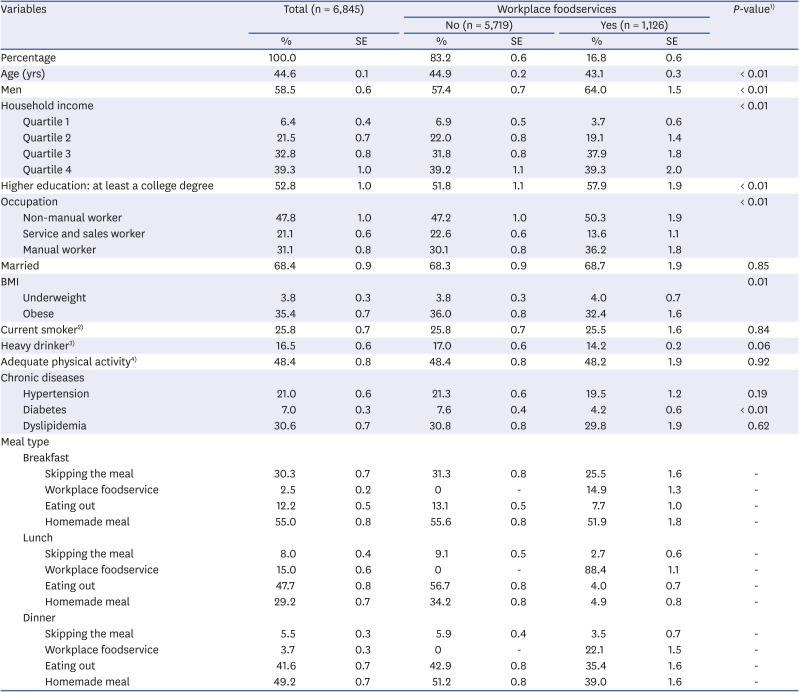
Table 1
Baseline characteristics of the study participants according to the use of workplace foodservices at least once a day
Data are expressed as weighted percentages with SEs for variables.
BMI, body mass index.
1)Analyzed using a weighted t-test or a weighted χ2 test to assess the differences between workplace foodservice non-users and those who used workplace foodservices at least once a day.
2)Participants who smoked at the time of the survey and who smoked ≥ 100 cigarettes in their lifetime.
3)Men who consumed 7 or more drinks and women who consumed 5 or more drinks at least twice a week.
4)Participants who engaged in moderate-intensity activities for at least 150 min during the week, vigorous-intensity activities for at least 75 min during the week, or an equivalent combination of moderate- and vigorous-intensity activities.
![]()
Dietary intake and nutritional quality according to the source of meal procurement
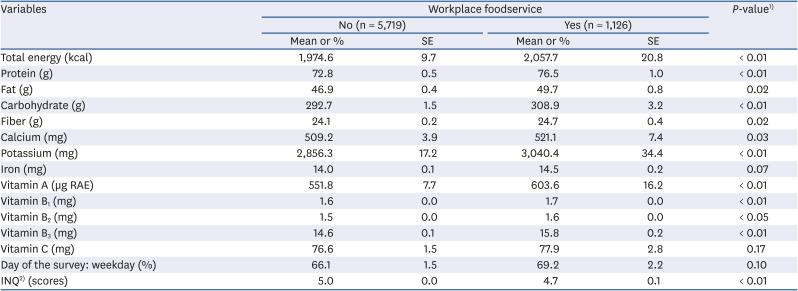
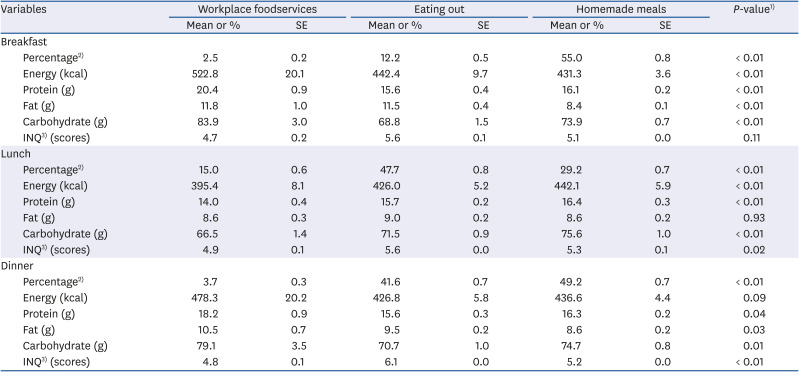
Analysis of the total daily meal data showed that workplace foodservice users had a higher intake of total energy and macronutrients (all P < 0.05) and exhibited lower INQ scores (P < 0.01) than did non-users (Table 2). The distribution of energy, intake of each macronutrient, and INQ scores for each meal type according to the meal procurement source are shown in Table 3. Workplace foodservice users had the highest intake of every macronutrient from breakfast and dinner, whereas they had the lowest intake of these macronutrients, except for fat from lunch. The INQ scores were significantly higher in the eating-out group and lowest in the workplace foodservices group for lunch and dinner. Furthermore, as shown in Fig. 2, the INQ scores from the total meals consumed in a day decreased with the frequency of workplace foodservice use among the workers (P < 0.01).
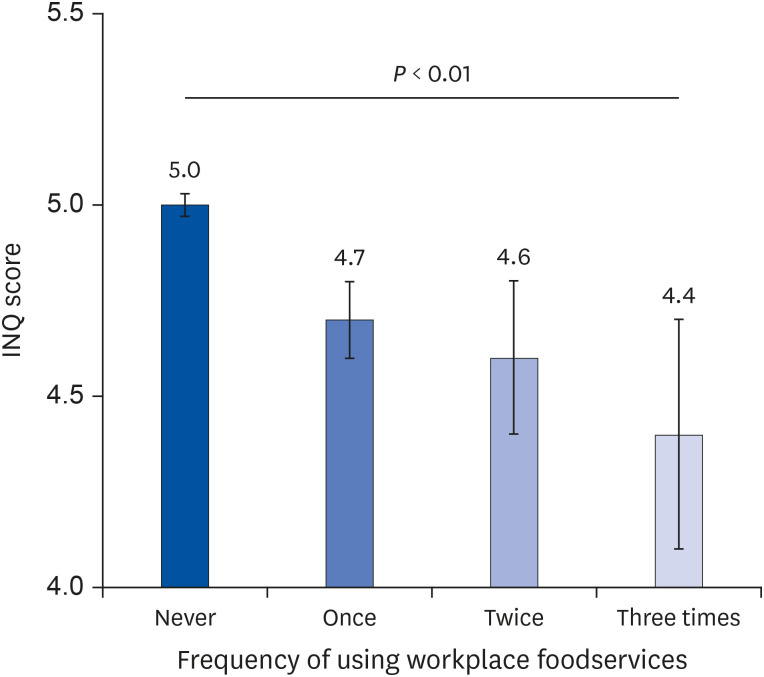 | Fig. 2Comparison of the INQ scores from total meals consumed in 1-day among study participants using a weighted linear regression analysis according to the frequency of workplace foodservices use. The intake of each nutrient, including protein, fiber, calcium, potassium, iron, and vitamins A, B1, B2, B3, and C, was calculated as a ratio of the actual consumed amount of a nutrient per 1,000 kcal to by the recommended nutrient intake or adequate intake from the dietary reference intakes for Koreans of the nutrient per 1,000 kcal according to age and sex. The ratio < 1.0 for each nutrient indicates insufficient nutrient intake, and the total number of these nutrients that were insufficiently ingested was regarded as the INQ score in this study. The mean INQ scores for the workers using workplace foodservices were as follows: never (n = 5,719), once (n = 908), twice (n = 177), and 3 times (n = 41) per day were 5.0 ± 0.03, 4.7 ± 0.1, 4.6 ± 0.2, and 4.4 ± 0.3, respectively (P < 0.01). Error bars represent the standard error of the average INQ scores.INQ, index of nutritional quality.
|
Table 2
Nutritional intake and quality of the total meals consumed in a day according to the use of workplace foodservices at least once a day (n = 6,845)
Data are expressed as weighted % for categorical variables and as mean values for continuous variables, with SEs.
RAE, retinol activity equivalents; INQ, index of nutritional quality.
1)Analyzed using a weighted t-test or a weighted χ2 test between workplace foodservice non-users and those who used workplace foodservices at least once a day.
2)The INQ of each nutrient, including protein, fiber, calcium, potassium, iron, and vitamins A, B1, B2, B3, and C, was calculated as the ratio of the nutrient density of the actual intake to by the recommended nutrient intake or adequate intake from the dietary reference intakes for Koreans of the nutrient per 1,000 kcal according to age and sex.
![]()
Table 3
Nutritional intake and quality of each type of meal according to meal procurement source (n = 6,845)
Data are expressed as weighted % for categorical variables and as mean values for continuous variables, with SEs.
INQ, index of nutritional quality.
1)Analyzed using a weighted analysis of variance according to the meal procurement source.
2)As the number of participants who consumed workplace foodservice meals, eating out meals, and homemade meals was different for each meal type (breakfast, lunch, and dinner), each percentage is indicated in the first line of the table.
3)The INQ of each nutrient, including protein, fiber, calcium, potassium, iron, and vitamins A, B1, B2, B3, and C, was calculated as the ratio of the nutrient density of the actual intake to by the recommended nutrient intake or adequate intake from the dietary reference intakes for Koreans of the nutrient per 1,000 kcal according to age and sex.
![]()
Association of workplace foodservice use with nutritional quality of the workers
A separate association was found between a lack of workplace foodservice use and INQ scores; these results are presented in Table 4 (β = 0.29, P < 0.01). We also found significantly positive associations between the INQ scores and following parameters: lower quartiles of household income (β = 0.37, quartile 1, 0.39 for quartile 2; and 0.25, quartile 3 vs. quartile 4), lower education (β = 0.16), inadequate physical activity (β = 0.35), and higher energy intake (β = 0.50 × 10−3). In contrast, negative associations of the INQ scores were found with the following parameters: older age (β = −0.02), male sex (β = −0.64), obesity (β = −0.20; vs. normal weight), history of smoking (β = −0.38), non-heavy drinker status (β = −0.59), and no history of hypertension (β = −0.30), after adjusting for all covariates.
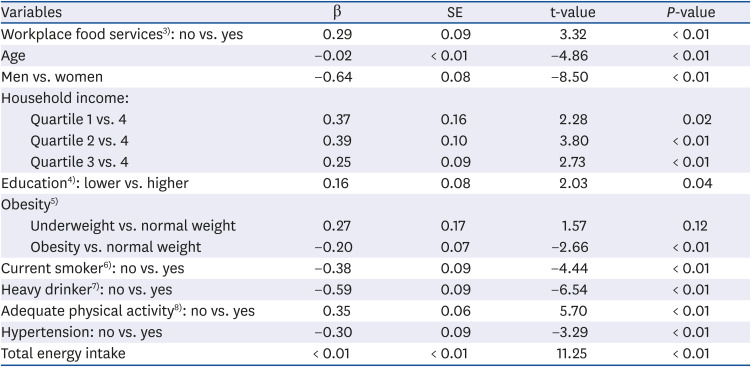
Table 4
Multivariate linear regression analysis to identify the independent clinical variables associated with index of nutritional quality1) after adjusting for all other covariates2) (n = 6,845)
Adjusted R2: 0.19.
1)The index of nutritional quality of each nutrient, including protein, fiber, calcium, potassium, iron, and vitamins A, B1, B2, B3, and C, was calculated as the ratio of the nutrient density of the actual intake to by the recommended nutrient intake or adequate intake from the dietary reference intakes for Koreans of the nutrient per 1,000 kcal according to age and sex.
2)Covariates included age, sex, household income, marital status, educational level, occupation, smoking status, heavy drinking, adequate physical activity, obesity, chronic diseases (such as hypertension, diabetes, and dyslipidemia), meal procurement source, and the day of the dietary survey.
3)Using workplace foodservices for at least one meal per day.
4)Higher education, having at least a college degree.
5)Underweight, body mass index < 18.5 kg/m2; obesity, body mass index ≥ 25 kg/m2.
6)Participants who smoked at the time of the survey and had smoked ≥ 100 cigarettes in their lifetime.
7)Men who consumed 7 or more drinks and women who consumed 5 or more drinks at least twice a week.
8)Participants who engaged in moderately intense activities for at least 150 min during the week, vigorous-intensity activities for at least 75 min during the week, or an equivalent combination of moderate- and vigorous-intensity activities.
![]()
Go to :
DISCUSSION
The present study identified differences in dietary intake and nutritional quality according to the meal procurement source and further assessed the association between the use of workplace foodservices and nutritional quality in a Korean representative sample of workers aged between 20 and 64 years. The nutritional quality of all 3 daily meals was higher in workplace foodservice users than in non-users, after adjusting for all covariates (Table 4). These findings indicate that workers may have more opportunities to meet their daily nutrient intake requirements using workplace foodservices. We further identified that the nutritional quality of the total daily meals increased significantly with the frequency of workplace foodservice use among workers, which is in line with our findings and confirms the robustness of the findings in this study.
Some previous studies have reported inverse associations between eating meals at the workplace and nutritional quality, such as more frequent consumption of energy-dense or unhealthy foods [2122]. However, food consumption in those studies was analyzed based on the location of food consumption, including workplace cafeterias in which workers could purchase fast foods, sugar-sweetened beverages, or unhealthy snacks, without classifying the place of food procurement, which may have caused a misestimation of nutritional intake and quality [2122].
Workplace foodservice users had a significantly higher intake of total energy and macronutrients as well as lower INQ scores than non-users, based on the total daily meal data. For quantitative and qualitative analyses of diets, we used the INQ scores to assess and compare nutritional quality, which can potentially reveal specific nutrient insufficiencies even if individuals have reached their total energy requirement [23]. The number of nutrients for which the intake was insufficient was used as a measure of INQ scores in this study. Therefore, higher INQ scores reflected poorer nutritional quality and signified an insufficient intake of a greater number of nutrients. Our results showed that workplace foodservice users were more likely to have sufficient nutrients to meet their individual health requirements. Although the INQ scores used in this study could not reflect the degree of nutrient overconsumption (which is unhealthy), we found that the prevalence of obesity and diabetes was lower in workplace foodservice users than in non-users. This appears to indirectly support the contention that using workplace foodservices has health benefits in terms of chronic diseases, including obesity and diabetes.
Our results are supported by those of previous studies that demonstrated the impact of workplace interventions promoting healthier food habits on health outcomes among employees [242526]. The nutritional quality of workplace foodservice meals may be higher than that of meals from other sources due to several factors. According to the Korean Food Sanitation Act, a licensed dietitian must be employed when operating a workplace meal service facility, particularly when an enterprise provides meals for > 100 individuals. The dietitians are responsible for not only the preparation and examination of meals, but also sanitary management at the facility [27]. They plan menus and help companies develop meals to ensure that the food is healthy for the employees and meets the guidelines mandated by the government and the company [28]. In addition, foodservices in the workplace are usually operated to improve employee welfare and productivity rather than profit. Thus, it is likely that the ingredients used at workplace foodservice centers may be of higher quality than those used at ordinary restaurants. Using workplace foodservices increases employee convenience and eating away from their desks allows for increased focus on their meals even during busy workdays, which is important because most adults in Korea spend a majority of their day at their workplace [2629]. In this study, we found no association between INQ scores and the day of the survey. The scores did not differ between those who participated in the diet survey on a weekend and those who participated on a weekday (P = 0.053); this could potentially be because many workers work even on weekends in Korea. The high accessibility of workplace foodservices to employees helps ensure AI of essential nutrients regularly and at the appropriate time. In fact, it has been well-established that environmental factors greatly influence the dietary behaviors of individuals. Previous studies have reported that workplace interventions regarding diet and other lifestyle factors modestly improve nutritional quality in a cost-effective and sustainable manner [1112]. Environmental strategies, such as increasing the availability of healthy foods and reducing barriers to healthy dietary intake may help individuals improve their dietary behaviors to promote their health and well-being. Given the recent trend of eating out more frequently, such interventions regarding workplace dietary environments should be a part of public health policy.
This study had some limitations. Because the dietary intake data in this study were based on self-reports using the 24-h recall method, under- or over-estimation of consumption cannot be ruled out. Although the use of this method may not result in data that fully reflect the long-term habits and dietary behaviors of adult Korean workers, this concern is mitigated by the high power of statistical tests due to the probability of revealing diverse dietary behaviors with a large sample size. Due to the cross-sectional design of this study, we could not conclude any causality. The possibility of unmeasured confounders cannot be completely ruled out and requires a strict analysis in further studies. Despite these limitations, this study was conducted using current data from a large nationally representative sample of adult Korean workers with validated measures. Our findings of a positive association between the use of workplace foodservices and nutritional quality are important with regard to public health concerns.
In a nationally representative sample of Korean workers, workplace foodservice use was associated with higher dietary nutritional quality. This finding underscores the importance of the introduction or expansion of workplace foodservices, including registered dietitians, for promoting high nutritional quality and healthy dietary habits among workers.
Go to :
 XML Download
XML Download