

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Depression is one of the most common mental disorders and can affect the quality of life [1]. In severe cases, it can lead to suicide. Depression is regarded as a public health problem worldwide and is a major contributor to the global burden of disease [2]. However, its pathogenesis remains unclear. Recently, dietary factors have been regarded as modifiable risk factors for depression, with improvements in dietary intake contributing to the prevention of depression [34].
Sugar-sweetened beverages (SSBs), which contain large amounts of sugar, are emerging as an important dietary factor that affects mental health; several studies have been conducted on the association between SSBs and a variety of health outcomes, including those in mental health [56789]. It is well known that SSBs are associated with hypertension, type 2 diabetes mellitus, metabolic syndrome, and cardiovascular disease (CVD) [56]. In terms of mental health, frequent SSB consumption was associated with a higher prevalence of depression, suicidal ideation, and other mental disorders in several studies among the Western and Asian populations [789].
The consumption of SSBs is increasing globally, and in Korea, the number of people who reported consuming SSBs doubled from 1998 to 2009 [10]. The socioeconomic burden of drinking more than one cup of SSBs was estimated to be approximately 633 billion won in Korea [11]. In one meta-analysis, the risk of depression showed a nonlinear dose-response relationship with SSB consumption [12]. However, the analysis did not include studies performed in Korea. Regarding the Korean population, a few studies reported that SSBs are associated with depression and suicidal ideation in people aged 12–28 years [1314]. Most studies in the Korean population are limited to children and adolescents, thus, evidence of the association between SSB consumption and depression or suicidal ideation is still limited among Korean adults.
Therefore, the aim of this study was to investigate the association between SSB consumption and depression and suicidal ideation among Korean adults.
Go to : 
SUBJECTS AND METHODS
Study participants
Data were drawn from the Korean National Health and Nutritional Examination Survey (KNHANES). The KNHANES is a cross-sectional survey that has nationally representative data of the non-institutional Korean population using a complex, stratified, multistage probability-sampling model. The design of the KNHANES has previously been described in detail [15]. We included two years of data from 2014 and 2016 in the study because both the Food Frequency Questionnaire (FFQ) and Patient Health Questionnaire-9 (PHQ-9) were investigated in these years. The 2014 KNHANES protocol was approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (2013-12EXP-03-5C), whereas the 2016 KNHANES were exempted from research ethics review based on the Bioethics and Safety Act.
From a total of 6,788 participants aged ≥ 20 years who completed the FFQ data collection, we excluded those who were pregnant or lactating women (n = 61), those who did not complete the data collection for PHQ-9 (n = 692), or those with a history of depression (n = 287), stroke, CVD or cancer (n = 283). The final cross-sectional study population comprised 5,465 participants.
Assessment of depression and suicidal ideation
The KNHANES used the Korean version of the PHQ-9 to assess the degree of depression in participants. The PHQ-9, which consists of nine criteria, was regarded as a reliable and valid diagnostic tool for screening for depression and is widely used in clinical practice [16]. This tool evaluates the severity of depression (loss of interest, depressed mood, trouble sleeping, tiredness or lack of energy, change in appetite, feelings of guilt or uselessness, trouble concentrating, being retarded or agitated, and suicidal ideation or self-inflicted thoughts). The cut-off for depression using the Korean version of the PHQ-9 was set to a score of 5 for this study [17].
To assess the suicidal ideation of the participants, we used the ninth question of the PHQ-9, which was “Thoughts that you would be better off dead, or of hurting yourself.” If the score of the PHQ-9 ninth item was ≥ 1, the participant was defined as having suicidal ideation.
Assessment of SSB intake
In the current study, the FFQ was used to assess the intake of beverages. SSB consumption was evaluated using the following questions: “During the past year, how often have you consumed each drink?” and “What was your average intake at one time?” Participants were asked to choose their frequency of SSB consumption among the following nine categories: none, once/month, 2–3 times/month, once/week, 2–4 times/week, 4–6 times/week, once/day, 2 times/day, and ≥ 3 times/day. The average intake amount consisted of the following three responses: consumption of 0.5 cup, 1 cup (200 mL), and 1.5 cups. SSB consumption was estimated using the sum of each beverage consumed, including soft drinks (i.e., coke and sprite, fruity soda), fruit juices, and sweetened rice drinks (i.e., grain powder drinks and Korean sweet rice punches), based on previous studies [18]. SSB consumption was classified into four categories: non-SSB drinkers, those who drank SSBs ≤ 2 cups/week, 3–6 cups/week, and SSBs ≥ 1 cup/day.
Confounding variables
The confounding variables included sociodemographic, health behavior and dietary variables obtained from a self-reported questionnaire. The sociodemographic variables included age, sex, body mass index (BMI), household income level, educational level, marital status, employment status, and living status. Household income level was classified into 2 groups (low and high) depending on the quartile of household income. Educational level was divided into three categories: below middle school graduate, high school graduate, college graduate and above. Marital status was categorized into 3 groups: single, living with a spouse after marriage, or living alone after divorce or bereavement. Employment and living status were categorized into two groups: unemployed or employed and living alone or living together.
Health behavior variables included smoking status (non-smokers, including those who had smoked less than five packs of cigarettes in their lifetime, Ex-smokers, and current smokers), alcohol consumption, physical activity (PA), and other comorbidities (hypertension, diabetes mellitus, thyroid disease). Alcohol consumption was divided into three categories: none, moderate, and risky. Drinking was defined as risky when the average amount of alcohol consumed at one time was more than 7 glasses for men, more than 5 glasses for women, and more than twice a week [19]. Moderate drinking was classified as the consumption of less than the risky alcohol intake level. The Global Physical Activity Questionnaire developed by World Health Organization was used in the KNHANES to assess aerobic PA. Vigorous intensity of PA was defined as the status of being out of breath or having a very fast heart rate for ≥ 10 min. Moderate intensity PA was defined as the status of being out of breath slightly or having a slightly fast heart rate for ≥ 10 min. Aerobic PA was defined as performing a moderate-intensity PA for more than 150 min/week, a vigorous-intensity PA for more than 75 min/week, or equivalent amounts of mixed aerobic PA based on the national guidelines for PA [20].
Dietary variables based on previous studies included consumption of coffee, green tea, and total energy intake from the FFQ data [921]. We categorized the participants into three groups according to the frequency of the consumption of coffee and green tea: non-drinkers and those who drank < 1 cup/day or ≥ 1 cup/day of coffee or green tea.
Statistical analysis
All statistical analyses were performed using the STATA 16 software (StataCorp, College Station, TX, USA). The analysis of this study was conducted considering cluster variables, strata, and the weighted value related to the complex sampling of the KNHANES.
The general characteristics of the participants according to SSB consumption categories are presented as the mean values (with standard errors) or as numbers (with percentages). The χ2 analysis was used to compare categorical variables, and one-way analysis of variance (ANOVA) was used to compare continuous variables.
The odds ratio (OR) for depression and suicidal ideation associated with SSB consumption was tested using logistic regression analysis, with the non-SSB drinker group as the reference group. For Model 1, a logistic regression analysis was used without adjustment. For Model 2, a multiple logistic regression analysis was used with adjustments for age and sex; for Model 3, all the above variables were used in addition to BMI, smoking, alcohol consumption, physical activity, marital status, household income level, employment status, educational level, and living status; for Model 4, all the variables used in Model 3 were used in addition to consumption frequencies of green tea, coffee, and total energy intake; We performed a trend analysis using multiple logistic regression. Statistical significance was set at 2-sided P < 0.05.
Go to :
RESULTS
Participant characteristics
Participant characteristics according to SSB consumption categories are presented in Table 1. In this study, about 30% of the participants reported that they had never consumed SSBs. The mean age of the non-SSB drinker group was 48.8 ± 10.4 years and that of the group with highest SSB consumption (≥ 1/day) was 34.7 ± 11.6 years. Participants with a higher intake of SSBs were more likely to be younger (P < 0.001), male (P < 0.001), current smokers (P< 0.001), unmarried (P < 0.001), employed (P = 0.032), and have a higher education level (P < 0.001) compared to non-SSB drinkers. The mean total energy intake significantly increased with SSB consumption. (P < 0.001). On the other hand, there were no significant differences in BMI, household income level, living status, or coffee consumption for SSB consumption.
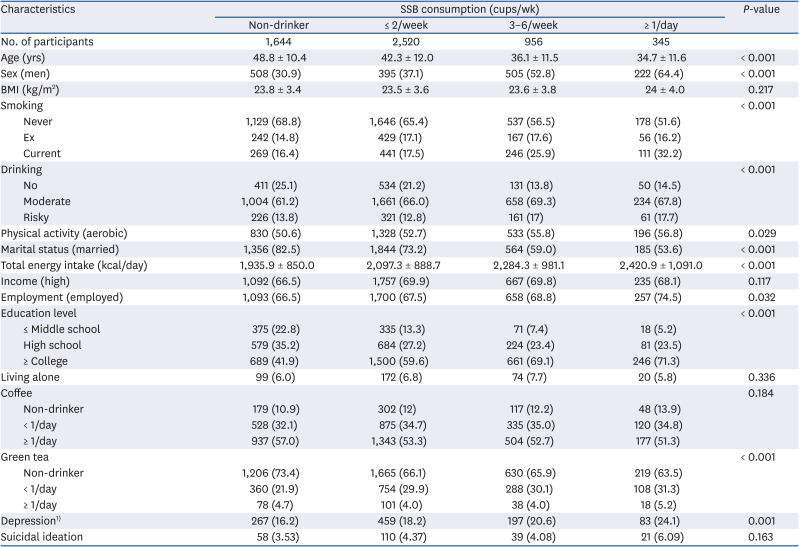
Table 1
Participant characteristics according to categories of SSB consumption
SSB, sugar-sweetened beverage; BMI, body mass index; ANOVA, analysis of variation; PHQ-9, Patient Health questionnaire-9.
P-values were calculated using ANOVA for continuous variables and χ2 tests for categorical variables. Values are presented as mean ± SEs or number (%).
1)Depression was defined as more than a score of 5 in the Korean version of the PHQ-9 questionnaire.
![]()
Association of SSB consumption with depression and suicidal ideation
The association between SSB consumption and depression is shown in Table 2. In all the models, the ORs for depression increased with an increase in SSB consumption. Even after adjusting for multiple confounding factors, the overall trend of the positive relationship did not change. In the final multiple logistic models, the adjusted values of the OR for depression across the SSB consumption categories were 1.00 (reference group) for non-SSB drinkers, 1.14 (95% confidence interval [CI], 0.94–1.39) for those who consumed less than 2 cups of SSBs/week, 1.36 [95% CI, 1.08–1.72] for those who consumed 3-6 cups of SSBs/week, and 1.58 [95% CI, 1.16–2.16] for those who consumed one or more cups of SSBs/day, with a P for trend < 0.001.

Table 2
ORs and 95% CI of depression according to SSB consumption
Statistical differences were tested using logistic regression analysis using following 4 models:
1) Not adjusted (Model 1), 2) Adjusted for age, sex (Model 2), 3) Model 2 with additional adjustment for BMI, smoking, alcohol, physical activity, marital status, household income, employment status, education level, living status (Model 3) 4) Model 3 with additional adjustment for consumption frequencies of green tea, coffee, total energy intake (Model 4).
OR, odds ratio; CI, confidence interval; SSB, sugar-sweetened beverage.
*P < 0.05 and **P < 0.01.
![]()
The ORs for suicidal ideation according to SSB consumption are shown in Table 3. Similar to the trend of depression across the SSB consumption categories shown above, the ORs for suicidal ideation increased with an increase in SSB consumption, except in the unadjusted model (P = 0.143). In Model 4, the adjusted values of the OR for suicidal ideation for the SSB consumption categories were 1.00 (reference) for non-SSB drinker, 1.63 (95% CI, 1.11–2.41) for those who consumed less than 2 cups of SSBs/week, 1.66 (95% CI, 0.96–2.87) for those who consumed 3–6 cups of SSBs/week, 2.20 (95% CI, 1.13–4.28) for those who consumed one or more cups of SSBs/day with P for trend < 0.001.

Table 3
ORs and 95% CI of suicidal ideation according to SSB consumption
Statistical differences were tested using logistic regression analysis using following 4 models:
1) Not adjusted (Model 1), 2) Adjusted for age, sex (Model 2), 3) Model 2 with additional adjustment for BMI, smoking, alcohol, physical activity, marital status, household income, employment status, education level, living status (Model 3) 4) Model 3 with additional adjustment for consumption frequencies of green tea, coffee, total energy intake (Model 4).
OR, odds ratio; CI, confidence interval; SSB, sugar-sweetened beverage.
*P < 0.05.
![]()
In other words, participants in the group with the highest SSB consumption (≥ 1/day) had a higher risk of depression by 54% (OR, 1.54; 95% CI, 1.08–2.18; P < 0.001) and a higher risk of suicidal ideation by 120% (OR, 2.20; 95% CI, 1.13–4.28; P < 0.001) compared to those in the non-SSB drinker group.
Notably, further analysis of the association of each SSB item (soft drinks, fruit juices, sweetened rice drinks) with depression revealed that soft drinks were mainly responsible for the association of SSB consumption with depression (Table 4).

Table 4
ORs and 95% CI of depression according to soft drinks, fruit juices, sweetened rice drinks consumption
Statistical differences were tested using multiple logistic regression analysis adjusted for age, sex, body mass index, smoking, alcohol consumption, physical activity, marital status, household income level, employment status, education level, living status, consumption frequencies of green tea, coffee, total energy intake. Values are presented as ORs (95% CI).
OR, odds ratio; CI, confidence interval; SSB, sugar-sweetened beverage.
**P < 0.01.
![]()
Subgroup analysis
After finding a positive association between SSB consumption and depression, we performed several subgroup analyses. Due to the differences in the number of participants in each group, the subgroup analyses were conducted after reclassifying the participants into three groups: non-SSB drinkers, those who consumed less than 2 cups of SSBs/week, and those who consumed more than 3 cups of SSBs/week. We performed a subgroup analysis according to age, sex, BMI, household income and education level using Model 4, which adjusted for sociodemographic, health behavior, and dietary variables. Table 5 presents the results of these analyses.
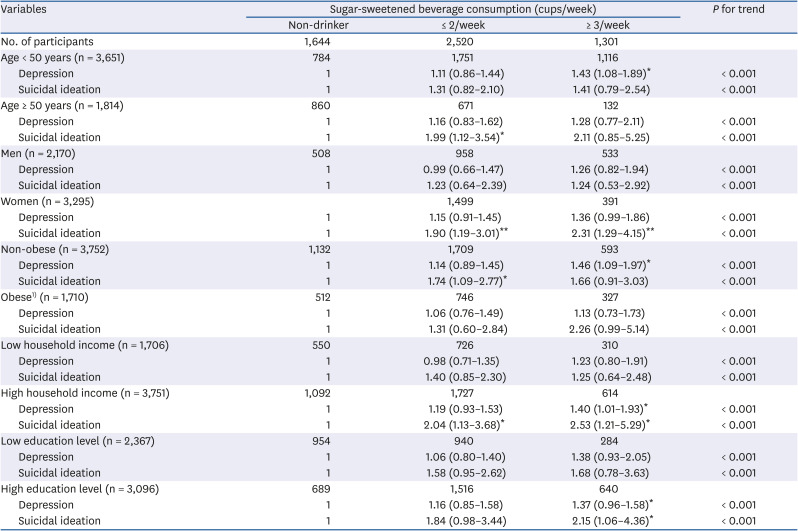
Table 5
Subgroup analysis
Statistical differences were tested using multiple logistic regression analysis adjusted for age, sex, BMI, smoking, alcohol consumption, physical activity, marital status, household income level, employment status, education level, living status, consumption frequencies of green tea, coffee, total energy intake. Values are presented as odd ratios (95% confidence interval).
BMI, body mass index.
1)Obese group defined as BMI ≥ 25 kg/m2.
*P < 0.05 and **P < 0.01.
![]()
Although the strength of the relationship between SSB consumption and depression and suicidal ideation varied, as shown by the different values of the ORs in each subgroup analysis, the overall trend of the positive relationship remained unchanged regardless of age, sex, BMI, household income level, and education level (P for trend < 0.001).
In the case of depression, the non-obese group had the highest ORs for SSB consumption (OR, 1.46; 95% CI, 1.09–1.97), and for suicidal ideation, the group with a high household income showed the highest ORs for SSB consumption (OR, 2.53; 95% CI, 1.21–5.29).
Go to :
DISCUSSION
Our study revealed a positive relationship between SSB consumption and depression, and SSB consumption and suicidal ideation in Korean adults. Those consuming ≥ 1 SSB/day had a significantly higher risk of depression and suicidal ideation compared with those who did not consume SSBs. SSB consumption was associated with depression and suicidal ideation after adjusting for sociodemographic, health behavior and dietary variables. In this study, participants who consumed ≥ 1 SSB/day had a higher risk of depression by 54% and higher risk of suicidal ideation by 120% when compared to non-SSB drinkers. The results of this study are consistent with the results of a previous meta-analysis of observational studies [12].
A cross-sectional study in Brazil reported that consumption of ≥ 16 glasses of SSBs/week was associated with severe depressive symptoms among women (prevalence ratio, 1.71; 95% CI, 1.06–4.12) [22]. In a prospective study in the US, participants who consumed ≥ 4 cans/day of soft drinks or fruit drinks had a higher risk of depression by 30% and 38%, respectively [21].
Few similar studies have been conducted in Asia; however, in one cross-sectional study in China, participants who consumed 4 cups/week of soft drinks had double the risk of depressive symptoms than those who consumed < 1 cup of soft drinks/week [9]. A recent prospective study in Japan also reported that those who consumed 4 cups/week of soft drinks had a higher risk for depressive symptoms by 91% when compared to those who consumed < 1 cup/week [8]. There are OR differences between the studies; however, the results of our study in the Korean population are consistent with previous studies conducted in Asia and support the hypothesis that a higher consumption of SSBs may increase the risk for depression.
There are several potential mechanisms underlying the relationship between SSB consumption and depression. First, SSBs contain a large amount of sugar. A high-fructose diet increases corticosterone levels [23], leading to dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis [24]. This HPA axis dysfunction may affect the development or course of depression and several other mental disorders [25]. Second, SSBs may cause symptoms of depression by increasing the circulating cytokine concentration through hyperglycemia [26]. In a meta-analysis, elevated levels of inflammatory markers such as C-reactive protein and interleukin-6 were significantly associated with the development of depressive symptoms [27]. Third, a study in the Netherlands showed that men who followed a high-fat, high-sugar diet for 6 weeks showed a significant decrease in level of serotonin transporter-binding in the hypothalamic region, that is, by 30%, in single photon emission computed tomography scans [28]. This decrease in serotonin level may increase the possibility of the development of anxiety and depression [29]. Fourth, the intake of sugar causes neurobiological changes in the reward system, compelling the individual to consume more sugar; it can affect negative emotional symptoms, similar to other substance-related addictive disorders [3031]. SSBs contain sugar in liquid form, which could cause both incomplete compensation for liquid calories and addictive eating, including loss of control [32].
In subgroup analysis, the association between SSB consumption and depression was stronger in the non-obese group and in the groups with high household income and education level. A high household income, high education level, and nonoccurrence of obesity may protect against depression by avoiding risk factors and harmful exposures. We believe that those with a relatively low risk of depression may be more significantly affected by consumption of SSBs than those at a high risk for depression.
This study has several advantages, including a large sample from a nationally representative survey conducted in Korea. To the best of our knowledge, this is the first cross-sectional study to examine the association between SSB consumption and depression and suicidal ideation among adults in a Korean population.
Our study also had some limitations: First, due to the cross-sectional design, we could not conclude whether higher SSB consumption increased the prevalence of depression or whether depression led to higher consumption of SSBs. Second, because we used the FFQ, participants were likely to underreport SSB consumption. In addition, due to the unavailability of the data, we evaluated total SSB consumption only by the sum of soda drinks, fruit juices, and sweetened rice drinks consumed, without considering of the type of SSBs. Third, only beverages were chosen as the dietary confounding factors because we aimed to examine the association between depression and sugar-containing drinks, not solid sugar. Therefore, we were unable to adjust for potential confounders such as the total sugar intake through solid food (e.g., fruits and candy), vegetables and family history of mental disorders. Finally, because the PHQ-9 is mainly used as a screening tool for depression, the results of this study may differ from the outcomes obtained if participants had a diagnosis of clinical depression. Further prospective studies are required to confirm the causality and the exact mechanism underlying the association of SSB consumption with depression and suicidal ideation.
In conclusion, SSB consumption is positively associated with depression and suicidal ideation among Korean adults. Our findings show that there is a need to continuously monitor SSB intake for mental health management. Further prospective studies or randomized controlled trials are required to confirm the impact of SSB consumption on mental health in the Korean population in the future.
Go to :
 XML Download
XML Download