

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Muscle cramps are sudden painful involuntary contractions of a muscle or muscle group.1 While commonly associated with neurological disorders of the lower motor neurons or peripheral nerves, muscle cramps are also frequently encountered in diverse medical conditions including chronic liver disease. With a reported prevalence of 22–88% in patients with chronic liver disease, previous studies have reported that the presence of muscle cramps is one of the leading factors significantly associated with sleep deprivation and poor health-related quality of life in cirrhotic patients.234567
The pathophysiology of muscle cramps in liver cirrhosis is largely unknown, but may involve multiple possibly overlapping factors including altered energy metabolism, nerve dysfunction, and changes in plasma volume and electrolytes.8910 Although the exact pathogenic mechanism remains to be elucidated, muscle cramps may arise from spontaneous ectopic discharges of the peripheral motor nerves in hyperexcitable states.1112 Pathological changes of the peripheral nerves and resulting peripheral nerve hyperexcitability (PNH) have been proposed to contribute to the development of muscle cramps in patients with chronic liver disease.1314 Therefore, targeting the neuronal excitability is a reasonable therapeutic approach for muscle cramps in patients with liver cirrhosis. Current treatment options are diverse, but their efficacy remains inconclusive with a paucity of evidence from randomized controlled trials.151617181920212223242526272829 Anticonvulsants, such as carbamazepine and phenytoin, can stabilize the neuronal excitability, but the metabolism of many anticonvulsant drugs involve cytochrome P450 isoenzymes. As such, their usage is often limited in patients with chronic liver disease.
Pregabalin is an appealing option, given its mechanism of action relevant to muscle cramps and pharmacokinetic properties favorable in patients with chronic liver disease.3031 A previous open-label trial of gabapentin, another gamma-aminobutyric acid analogue, showed a significant reduction in the frequency and severity of muscle cramps originating from various neurologic causes.323334 Gabapentin and pregabalin are neither metabolized by the liver nor bound to plasma proteins, and indeed preferred anticonvulsants in cirrhotic patients with epilepsy or neuropathic pain unless renal function is severely impaired. Besides the similar therapeutic profile, pregabalin has distinct pharmacokinetic advantages over gabapentin. The bioavailability of pregabalin is higher and less variable with a rapid and nonsaturable linear absorption, which may translate into better safety and efficacy profiles. With the goal of investigating the efficacy and safety of pregabalin for the treatment of muscle cramps in patients with liver cirrhosis, we conducted a 6-week randomized, double-blind, placebo-controlled single center trial. This study was terminated early because of insufficient accrual, with 80% (n = 56) of the target number of participants (n = 70) being randomized to pregabalin (n = 29) or placebo (n = 27). With multiple problems emerging from premature termination of trial in mind, the results appeared to suggest an acceptable safety profile and favorable effect of pregabalin in reducing muscle cramps compared to placebo in cirrhotic patients.
METHODS
The primary research question of this study was whether pregabalin is safe and clinically effective against muscle cramp in patients with liver cirrhosis. This study provides class II evidence that pregabalin is safe and significantly reduce the cramp frequency in patients with liver cirrhosis. Because of premature termination of trials, however, caution should be taken with respect to the interpretation of the results.
Study design and intervention
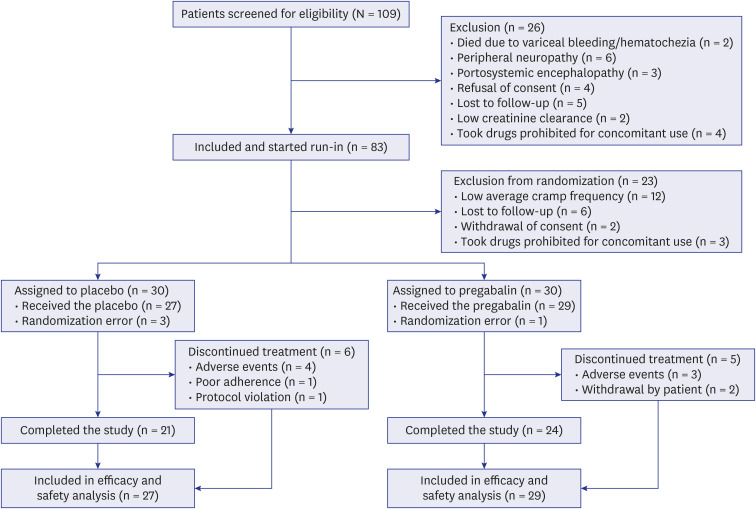
In this randomized, double-blind, placebo-controlled clinical trial, participants with liver cirrhosis received 6-week treatment with pregabalin or placebo after 4-week run-in period at single tertiary referral center (the Seoul Metropolitan Government Seoul National University Boramae Medical Center in Seoul, South Korea) (Fig. 1).
Patients
Eligible subjects were adults seen in outpatient clinic with a diagnosis of liver cirrhosis aged 75 years or younger who complained of frequent muscle cramps defined as ≥ 2 per week on average during the month before enrollment. Liver cirrhosis was diagnosed if there were either radiological and/or histological findings of liver cirrhosis or clinical signs of portal hypertension such as thrombocytopenia, splenomegaly, ascites, or esophageal varix. Patients were excluded if they had comorbid neurological disorders (peripheral neuropathy, stroke, epilepsy, inflammatory central nervous system disorders, and Parkinson’s disease), thyroid disorder, peripheral artery disease, alcohol use disorder, renal impairment (creatinine clearance < 60 mL/min) and congestive heart failure requiring medications. Neurological examination was conducted by expert neurologists in order to rule out the presence of peripheral neuropathy, and nerve conduction study as needed. Patients were also excluded if they had serious complications from liver cirrhosis, including portosystemic encephalopathy based on West-Haven criteria,3536 variceal bleeding, and ascites refractory to medical treatment within 3 months before enrollment, or used the following drugs that might potentially affect muscle cramps within 3 months before enrollment: gabapentin, carbamazepine, phenytoin, quinidine, digitalis, lithium, beta-agonist, beta-blockers, clofibrate, tricyclic antidepressants, verapamil, anti-spastic drugs, opiate, acetaminophen and NSAIDs.
Randomization and masking
Eligible subjects who provided informed consent went through 4-week run-in period, and were asked to keep the cramp diary to record the number, time of day, and severity (numerical rating scale for pain) of muscle cramps on a daily basis. If the frequency of muscle cramps is ≥ 2 per week on average during the run-in period, subjects were randomly assigned in a 1:1 ratio with a block size of four to receive either pregabalin or placebo using a web-based allocation system provided by the Medical Research Collaborating Center of Seoul National University Hospital Biomedical Institute. All study participants and investigators were blinded to all treatment allocations throughout the study period.
Procedures
The administration schedule for pregabalin included a titration dose of 75 mg twice a day for 1 week, followed by a standard dose of 150 mg twice a day for 4 weeks, and a tapered dose of 75 mg twice a day for the last 1 week. The placebo was given on the same schedule. Depending on the subject's tolerance and adverse events (AEs), dose adjustment was allowed at physician’s discretion. If intolerable symptoms persisted even after dose reduction, the study medication was discontinued. Medication adherence was checked by a pill count at each study visit after treatment allocation.
Safety assessment
AEs were assessed at each visit, through the analysis of vital signs, adverse effect, dosage reduction, and patients who were dropped out.
Outcome measures
The primary efficacy endpoint was the relative change from baseline (run-in) to treatment phase (standard dose) in the frequency of total muscle cramps. Secondary efficacy endpoints were 1) the responder rate (responders were defined as those who achieved ≥ 50% reduction from baseline in the frequency of total muscle cramps), 2) the change from baseline in the frequency of muscle cramps during sleep, 3) the change from baseline in the pain intensity (11-point numerical rating scale), and 4) the change from baseline in health-related quality of life, as measured by the Korean versions of the Short Form-36 (SF-36) and the Liver Disease Quality of Life Instrument (LDQOL).373839 To assess the effect of pregabalin on PNH, we performed the repetitive nerve stimulation (RNS) test, as described by Benatar et al.,40 with some modifications (Synergy electromyography system; Oxford Instruments, Hawthorne, NY).4142 A rationale and detailed protocol of the neurophysiologic evaluation are provided in the supplementary information (Appendix 1). All change-from-baseline endpoint analyses (except for the quality of life and neurophysiologic measures) were assessed based on the cramp diary which was filled in daily during the run-in and treatment phases. The quality of life (SF-36 and LDQOL) and neurophysiologic assessments were measured during the run-in period and at the end of standard dose treatment (week 5). Safety was assessed by vital sign measurements, physical examinations, clinical laboratory tests, and the incidences of AEs and serious AEs.
Sample size calculation
The sample size of 70 study subjects (35 per each group) was estimated to provide 80% statistical power to detect a difference of 3 in the mean rank regarding the change from baseline in cramp frequency between the pregabalin and placebo groups at a two-sided type I error of 5%, assuming a common SD of 4 and 10% of study subjects dropping out. The prespecified mean rank difference and SD were based on the results of previous quinidine and gabapentin trials.2632
Statistical analysis
Baseline characteristics of the treatment groups were compared by the Wilcoxon rank sum test and Fisher’s exact test as appropriate. Data obtained from the cramp diary were aggregated to weekly averages. The primary efficacy endpoint was assessed using the Wilcoxon rank sum test to compare the percentage change from baseline between the pregabalin and placebo treatment groups.
The prespecified responder analysis compared the proportion of subjects who achieved at least a 50% reduction in total cramp frequency from baseline using the Fisher’s exact test. To assess the effect of different thresholds, post hoc analysis was performed with varying thresholds (30%, 40%, 60%, and 70%). We also conducted post hoc exploratory analyses using rank ANCOVA, accounting for the effects of potential confounders (presence of ascites, use of diuretics, Child-Pugh class, age, and sex). For each subject, the rank was assigned on the basis of the change from the run-in phase to the standard dose treatment phase (4 weeks per each). The same approach was followed to assess the changes from baseline in cramp frequency during sleep and pain intensity per cramp.
The results of electrophysiological evaluation (RNST) were expressed by the cramp potential threshold frequency (TF). Cramp potential was defined as the continuous, high-frequency motor unit potential firings that occur immediately following RNS. The cramp potential TF is the minimum electrical stimulation frequency (Hz) at which the cramp potentials occur. It was categorized in the following order: 5 Hz, 10 Hz, and 15 Hz. If cramp potential does not occur until the stimulation frequency is increased to the maximum (15 Hz), TF was designated as “no cramp potential”. TF values were then converted into interval data with equal distance between all adjacent levels such that the changes from baseline could be scored by the degree of changes. The changes in TF from baseline to week 5 were compared between the pregabalin and placebo groups using the linear-by-linear association test for trend (ordinal χ2 test).
Efficacy and safety analyses were performed with the modified intention-to-treat population, defined as all randomized study participants who received at least one dose of the study drug. Neurophysiologic efficacy analysis used all available data that met blinded electrophysiologic data quality review. Missing data were imputed with the principle of baseline observations carried forward. Safety data were summarized using descriptive statistics. All statistical analyses were performed with the statistical software R (version 3.5). Tests with a two-sided significance level of less than 5% were considered statistically significant.
Role of the funding source
This is an investigator-initiated study, and the funder had no role in the study design, data collection, analysis, interpretation, or writing of the report. All authors have access to the data and assumed responsibility for the integrity and completeness of the reported data. Corresponding authors (WK and YHH) vouch for the integrity of the data analyses and have final responsibility for the decision to submit the manuscript for publication.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Seoul Metropolitan Government Seoul National University Boramae Medical Center (approval No. 06-2010-132). Written informed consent was obtained from all the participants. All authors had access to the study data and reviewed and approved the final manuscript. This study is registered at ClinicalTrials.gov, number NCT01271660.
RESULTS
Participants
This study was terminated early because of insufficient accrual. Between July 2011 and December 2017, a total of 109 patients were screened for eligibility, and 83 individuals consented to participate. Twenty-three participants (27.7%) were excluded from randomization after 4-week run-in phase (Fig. 1 for the reasons of exclusion). Of 60 participants, 4 were inadvertently randomized despite poor compliance with cramp diary during the run-in phase (3 in the placebo group, and 1 in the pregabalin group). Excluding these randomization errors, 80% (n = 56) of the target number of participants (n = 70) were randomized to pregabalin or placebo, and these 56 participants were included in the modified intention-to-treat analysis population (29 in the pregabalin group and 27 in the placebo group, respectively). Of the 56 participants, 45 completed the study and the other 11 dropped out prematurely. The most common reason for discontinuation was the occurrence of AEs.
Overall, treatment groups were well matched in terms of baseline characteristics regarding the demographic features, the etiology and severity of liver cirrhosis, and the medical history (Table 1, Supplementary Tables 1 and 2). The median baseline frequency of muscle cramps was 6.2 per week, and the median pain intensity per cramp was 4.8.
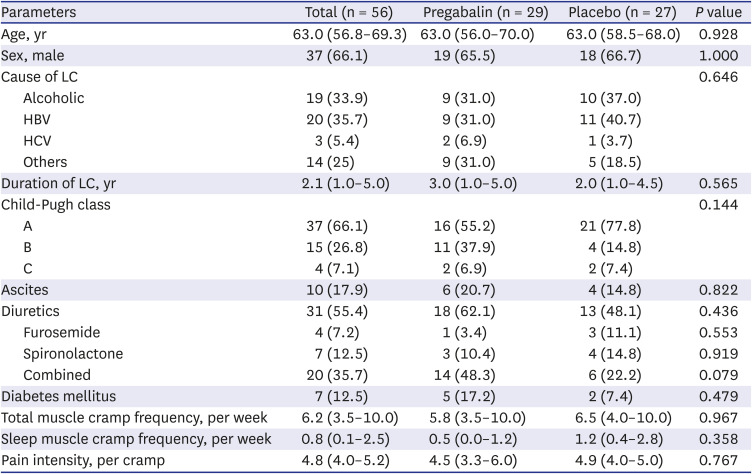
Table 1
Baseline characteristics
Data are expressed as the number of subjects (%) or median (interquartile range) as appropriate.
LC = liver cirrhosis, HBV = hepatitis B virus, HCV = hepatitis C virus.
![]()
Efficacy
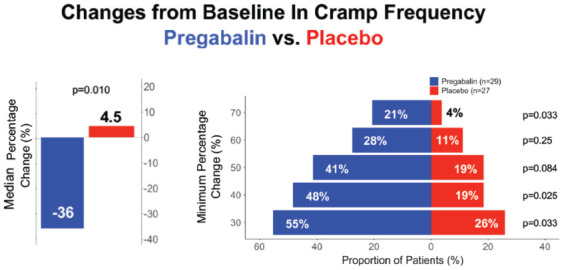
Primary endpoint analysis showed a benefit with pregabalin treatment compared to placebo (−36% vs. 4.5% for the percentage change, P = 0.010, Wilcoxon rank sum test) (Table 2 and Fig. 2A). Post hoc analysis using rank ANCOVA was in line with the primary endpoint analysis (rank-based difference −11 [95% confidence interval, −19.8, −2.2], P = 0.016). In the prespecified responder analysis, a higher proportion of participants achieved 50% reduction in cramp frequency with pregabalin treatment compared to placebo (41% vs. 19%, P = 0.080, Fisher’s exact test). Post hoc exploratory responder analyses with a range of thresholds were also in favor of pregabalin compared to placebo (Fig. 2B).
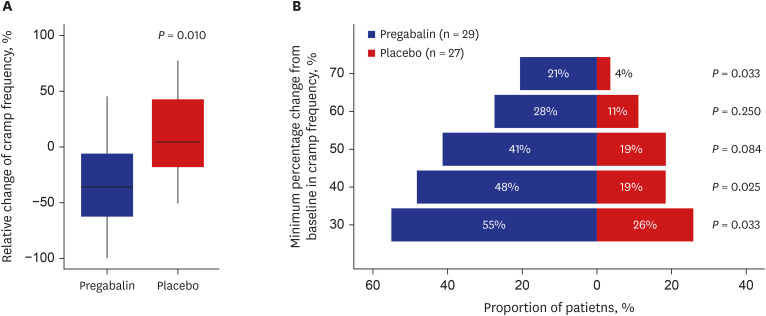
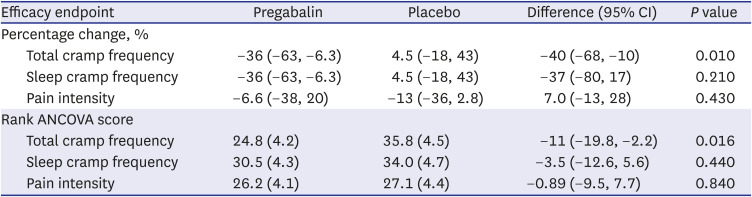
Fig. 2
Changes in the relative frequency of muscle cramps. (A) Box plots of the relative change in the frequency of muscle cramps from baseline (run-in phase) to the standard dose treatment phase (4 weeks per each) (P = 0.010 by the Wilcoxon rank sum test). (B) Responder analyses over a range of cut-off points for the minimum percentage change. P values calculated using the Fisher's exact test.
![]()
Table 2
Efficacy analyses
Data are the changes from the run-in phase to the standard dose treatment phase. The percentage changes were compared between the pregabalin and placebo treatment groups, using the Wilcoxon rank sum test. Estimates of the treatment effect were presented with medians (with interquartile ranges) for the percentage change, while they were given the least-squares means (with standard errors) in rank ANCOVA. For the rank-based ANCOVA, each subject was ranked from 1 (best) to 56 (worst), whereby the subject who had greater improvement was ranked higher according to the change in each efficacy parameter. Possible confounders were entered as covariates in ANCOVA, which included ascites, use of diuretics, Child-Pugh class, age, and sex.
CI = confidence interval.
![]()
The changes in sleep cramp frequency, average pain intensity, and health-related QOL measures did not differ significantly between the two groups (Table 2, Supplementary Tables 3 and 4). Electrophysiologic evaluation was not performed in 7 participants, and the results from 2 participants were excluded due to poor quality data at baseline (movement artifacts). We observed the occurrence of RNS-evoked cramp potentials in 26 participants (55%) at baseline, and 19 participants (40%) at week 5 (Supplementary Fig. 1 as a representative example). There was a significant association between the electrophysiological measure of PNH (e.g., TF for cramp potentials) and the frequency of clinical muscle cramps (P = 0.006 for the run-in phase, P = 0.003 for the treatment phase, ANOVA, Supplementary Fig. 2). A higher proportion of participants in the pregabalin group had a lower TF compared to placebo at baseline, although the difference was not statistically significant (P = 0.360, χ2 test). The change in PNH did not differ significantly between the two groups, although there was a tendency favoring pregabalin treatment (P = 0.140, ordinal χ2 test for the change in TF, Supplementary Fig. 3).
Safety
Thirty-four (60.7%) participants had at least one treatment-emergent AE. There was no significant difference in the rates of overall AEs between the pregabalin and placebo groups (Table 3). The most common AEs were dizziness and lethargy in the pregabalin group, and gastrointestinal discomfort and sleepiness in the placebo group. Most AEs were mild to moderate in severity. Serious AEs occurred in 2 participants in the placebo group (liver transplantation in one and hepatocellular carcinoma in the other). Another two in the placebo group discontinued treatment due to generalized weakness, and three participants in the pregabalin group discontinued the study drug because of dizziness. Four participants (two per each group) required dose reduction due to AEs; dizziness in the pregabalin group and gastrointestinal discomfort in the placebo group, respectively.
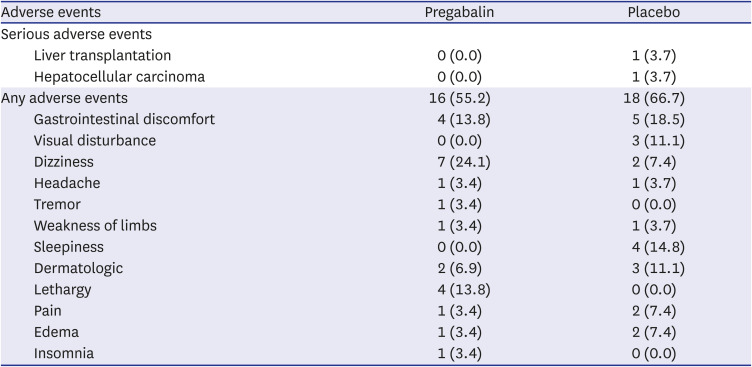
Table 3
Treatment-emergent serious adverse events and adverse events
![]()
DISCUSSION
This trial was terminated early due to poor accrual of participants. In modified intention-to-treat analysis with 80% of original target number of participants, we observed 40% difference in the relative change of total cramp frequency over 6 weeks treatment of pregabalin vs. placebo. In the responder analyses with varying thresholds for defining clinically meaningful change in the frequency of muscle cramps, twice to five times as many participants responded to pregabalin treatment compared to placebo. Secondary endpoints did not differ significantly between the two groups. We acknowledge that the results should be interpreted with caution because of premature termination of the trial. With multiple problems emerging from premature termination in mind, the results seem to suggest an acceptable safety profile and favorable effect of pregabalin in reducing muscle cramps compared to placebo in cirrhotic patients.
Despite the high prevalence and considerably negative impact, there is no standardized, approved pharmacotherapy against muscle cramps in patients with liver cirrhosis. Current therapeutic options for muscle cramps have not been rigorously assessed in the setting of a prospective randomized placebo-controlled study for cirrhotic patients. To our knowledge, there have been only 6 randomized controlled trials of pharmacologic agents or dietary supplements that include quinidine, vitamin E, branched chain amino acids, baclofen, taurine, and methocarbamol.171920242643 Although likely effective to some degree, quinidine and quinine derivatives are not generally recommended because of their potential toxicities such as hepatotoxicity and arrhythmogenic propensity.44454647 Vitamin E was not effective in the management of muscle cramps.17 Nocturnal administration of branched chain amino acids was demonstrated to reduce muscle cramps but failed to improve patients' quality of life in a small-scale study.48 Baclofen was shown to decrease the frequency and duration of muscle cramps, but the impact on quality of life was not assessed with formally validated tools.24 Taurine resulted in a significant improvement of muscle cramps in patients with chronic liver disease.20 This crossover study, however, was limited by a high attrition rate (19/49, 39%), and the efficacy analysis was restricted to those participants who completed the protocol. Methocarbamol might be an effective therapy for muscle cramps, but has been studied only for patients with hepatitis C-related liver cirrhosis.43
The present study was conducted with a rigorous randomized placebo-controlled study design, the use of validated outcome measures, including health-related QOL, neurophysiologic assessment, and multiple approaches for statistical analysis. We used a cramp diary throughout the study period instead of relying on patients' reports at study visits which might be prone to recall bias. To overcome the subjective nature of patient-reported outcome measures,242643 we also conducted neurophysiologic evaluation to assess the presence and degree of PNH. Of note, the electrophysiological feature of PNH was observed in unexpectedly large proportion of the patients (55% at baseline) with a significant association between the degree of hyperexcitability and the frequency of clinical muscle cramps. While these findings certainly require further validation in a larger independent cohort, our results suggest that electrophysiological evaluation using RNS may be useful for assessing the clinical predisposition to muscle cramps in cirrhotic patients. Furthermore, the TF for RNS-evoked cramp potentials tended to be reduced with pregabalin compared to placebo, corroborating the clinical effect of pregabalin against muscle cramps. Given the potential usefulness of RNS, it would be worthwhile to apply the electrophysiological test for appropriate stratification or selection of patients in future therapeutic trials.
Limitations of the present study should be acknowledged. This trial was terminated early because of insufficient accrual. We could not exclude the possibility that the treatment effect might be overestimated because of large variations among individuals. Other limitations include the small sample size, short duration of study, single center cohort, and the restricted inclusion criteria. Of note, participants in the placebo group had higher cramps frequency and pain severity at baseline, although the differences were not statistically significant. It also should be pointed out that the exclusion of 4 inadvertently randomized participants might entail the risk of bias and decrease in statistical power. With multiple problems emerging from premature termination of trial in mind, the results seemed to suggest an acceptable safety profile and favorable effect of pregabalin in reducing muscle cramps compared to placebo in cirrhotic patients. Larger studies are warranted to evaluate the efficacy and safety of pregabalin in the management of muscle cramps in patients with cirrhosis. Our results should stimulate further research into the pathophysiologic role of PNH in muscle cramps.
 XML Download
XML Download