

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic low back pain (CLBP) is one of the most prevalent problems worldwide. It restricts employees from working for at least 23 days in a year [1234]. There is no obvious patho-anatomical diagnosis for almost 85% of CLBP sufferers [5]. This type of low back pain is called non-specific chronic low back pain (NCLBP). It is a multifactorial condition associated with various dysfunctions such as gait abnormality [56]. Various studies have reported that patients with CLBP have altered movement pattern and control strategy to avoid painful motion during gait [27]. Abnormal lumbo-pelvic and thorax-pelvic movement pattern has been demonstrated in NCLBP patients due to changes in control strategy during gait [689]. Thus, gait analysis has been performed to understand the movement pattern and coordination of the lumbar and thorax relative to the pelvis [10].
In clinical settings, gait evaluation is carried out by observation and functional tests [11] or specific disability questionnaires [12] which can only provide limited information. Image-based three-dimensional (3D) motion capture system has been introduced to understand kinematic patterns during gait [13], although it is time consuming. Kinematic assessments using this precise system can potentially give useful outcome measures and quantify kinematic data during gait to assess the efficacy of rehabilitation approaches including core stabilization exercise and manual therapy or manipulative therapy [14]. However, reliability of kinematic parameters is not the same for all conditions and diseases [15]. As with any analysis tool, reliability and measurement error emerge as critical factors in their applicability to clinical decision-making [16]. Since low reliability in clinical research may lead to underestimation or failed detection of significant effect sizes [10], we need to strive for good reliability. Knowledge of error's magnitude can minimize the risk of over-interpretation of small differences as meaningful [17]. It can contribute to the certainty that a measured intervention effect exceeds the measurement error.
It is known that different regions of the lumbar spine move differently during gait [1] and other functional tasks [1819]. Gender differences also exist in total lumbar spine range of motion during simple tasks in CLBP and healthy participants [20]. These regional and gender differences can lead to differences in error magnitude and test-retest reliability [2122]. Dvorak et al. [20] have evaluated the effect of gender difference on lumbar spine kinematics during simple flexion-extension, lateral bending, and rotation tasks in healthy participants. Their results revealed minor gender differences for these simple trunk tasks [20]. However, after evaluating the reliability of a 3D-measurement device during simple flexextension, lateral bending, and rotation tasks in CLBP, Harsted et al. [22] and Mieritz et al. [23] have found that male participants exhibit greater ICCs and lower measurement errors in three planes than female participants. They used a CA-6000 Spine Motion Analyzer system (OSI, Union City, CA, USA) which consisted of six potentiometers, not an image-based motion analyzer [202223]. They also evaluated total lumbar spine normal range of motion [20]. In gait studies, only one study has provided absolute measures of measurement error and MDCs for spine kinematic parameters in healthy individuals. Fernandes et al. [24] have reported acceptable intraclass correlation coefficient (ICC, 0.51–0.95) for most joint angles with a standard error of measurement (SEM) ≤4° [24]. In a recent study, they have evaluated the reliability of trunk during gait in CLBP and reported that the obtained ICCs demonstrate high test-retest reliability for most joint angles, with low SEM (<2.58) [25]. However, they did not evaluate the effect of gender difference or multi-segmental lumbar spine on reliability and measurement error. They have suggested that further research is needed to evaluate the effect of gender difference and lumbar spine upper and lower segment assessment on reliability.
Data on reliability and measurement error of the 3D motion analyzing system during gait are lacking when gender difference and two upper and lower lumbar spine segments are noted in CLBP patients. A few studies have evaluated the reliability of 3D spinal motion analysis in CLBP during gait [2425]. However, they focused on total lumbar spine as a rigid segment without reporting gender differences. It is known that the reliability of measurement tools is closely dependent on the population [26], regional segment [21], and the task being assessed [24]. Therefore, the aim of this study was to evaluate test-retest reliability of the 3D motion capture system to assess thorax, total lumbar, and upper and lower lumbar segment kinematics relative to the pelvis in two groups (males and females) of patients with NCLBP during gait.
Go to : 
MATERIALS AND METHODS
Study design
This was a test-retest (within assessor) prospective observational study designed to investigate the reliability of the 3D motion capture system to assess trunk and lumbar and pelvis kinematics during gait in two groups (males and females) of patients with NCLBP during gait. This study was approved by the Ethical Committee of the Iran University of Medical Sciences (Ethical Approval No. IR.IUMS.REC 1395.9211342205; IRCT No. IRCT2016080829264N1).
Participants
A total of 40 participants (20 males and 20 females) who were diagnosed with NCLBP by a physician between August 2016 and November 2016 from orthopedics and physiotherapy clinics of Iran University of Medical Sciences were recruited into this study. Participants were patients who met the inclusion criteria and who agreed to participate in this study via a convenience sampling method. Participants were recruited through posters displayed in frequently-visited areas of the university and surrounding locality. Patients were also referred by several physicians in three large hospitals in Tehran. Mean height of females is lower relative to that of males in Iran [27]. Accordingly, this large CLBP community in the recruitment phase required the inclusion of a sample of 20 females with sufficient mean height to match with 20 males. The purpose of this study and examination involved in this project were explained to participants. Written informed consent was obtained from each participant. Sample size calculation was performed according to studies of Fernandes et al. [2425]. To achieve a 5% level of significance with 80% power, Fernandes et al. [2425] calculated that 17 subjects were required to set the reliability coefficient at 0.90 with a minimum reliability of 0.70. However, they evaluated 23 NCLBP patients and 23 healthy subjects. Therefore, we included a minimum of 20 subjects in each group. Inclusion criteria were: age of 30–40 years, low back pain lasting for more than 12 weeks, and pain score of 3 to 6 according to visual analogue scale (VAS). Participants were excluded if they had sciatic nerve root involvement, presence of pain radiating to the leg below the knee, paresthesia in the feet, motor deficits in lower extremity muscles, acute spinal disc herniation, previous surgery or fractures in the lumbar spine or other bonny structures, pregnancy, or body mass index (BMI) above 25 kg/m2. These two groups were matched in age, BMI, and VAS at the time of testing [21]. According to previous studies on reliability, BMI can influence the reliability and measurement errors of spinal motions in three planes in CLBP [2223]. However, we aimed to evaluate how acceptable the proportion of reliability and measurement error could be according to their spinal movement variability due to CLBP in this study. Participants with BMI higher than 25 kg/m2 were excluded from this study.
Three-dimensional motion analyses
A 3D approach was used for kinematic analysis of trunk, lumbar, and pelvis for all participants. Six cameras were set up to measure kinematics of the trunk, lumbar, and pelvis during walking. Gait kinematic variables were captured at 100 Hz using a 10MX T20 camera 3D motion capture system (Qualisys, Gothenburg, Sweden). They were analyzed using both QTM software (Qualisys, Goteborg, Sweden), custom MATLAB software version R2015 (matrix laboratory), and Microsoft Excel 2010 (Microsoft Corp., Redmond, WA, USA). Using palpation, anatomical landmarks were identified by a physical therapist for each participant and 13 reflective markers with a size of 10 mm×8 mm and circular cross-section were placed on these landmarks to capture kinematics of each segment with the movement analysis system.
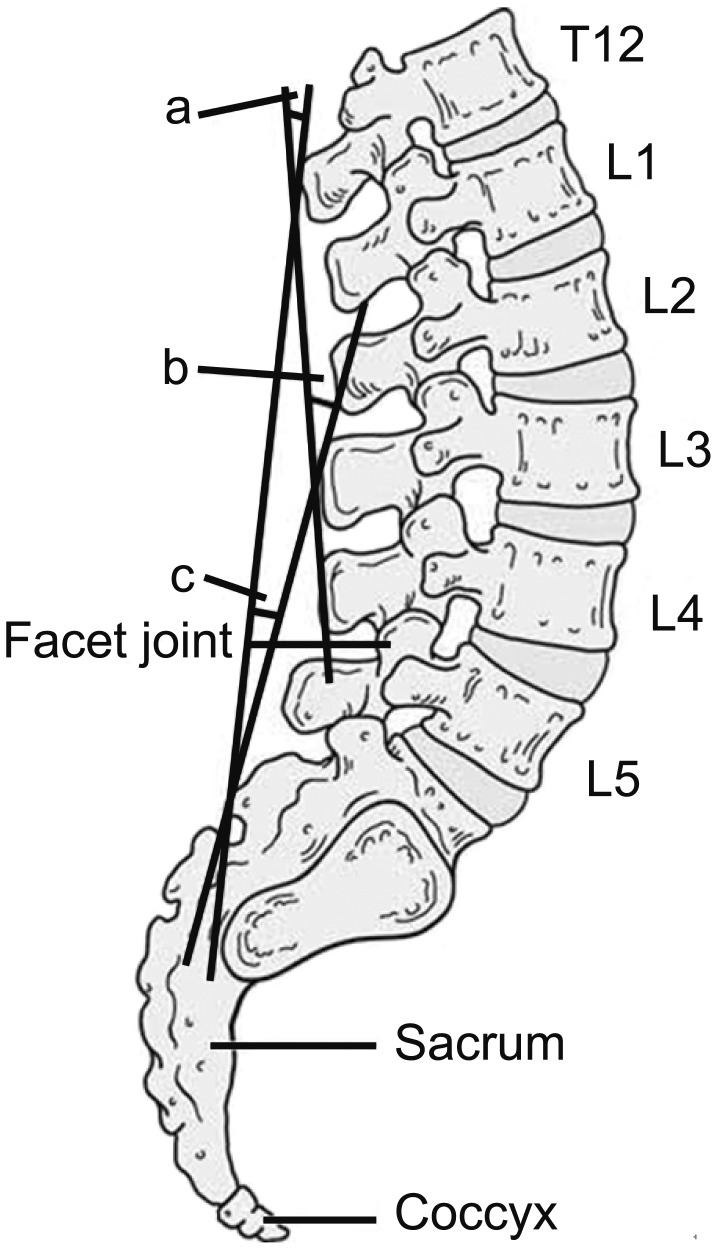
The following standardized marker locations were used [21]: T12 was first located and marked using the technique suggested in Gray's Anatomy for Students [28]. The spinous process of T12 was identified while participants were in a flexed standing position supporting themselves on a stool. Marker location was confirmed by counting spinous processes from T12 down to the S2 spinous process. It was then double checked by counting back up to the marked spinous process (Fig. 1). Three markers were placed on the spinous process of T12, L3, and S2. Two markers were placed on acromioclavicular (AC) joints. Four markers were placed on bilateral anterior superior iliac spines (ASIS) and posterior superior iliac spines (PSIS). To detect gait cycle during walking trials, four markers were placed on the posterior calcaneal tubercle (posterior heel center) and the 5th metatarsophalangeal joint of both feet [2]. A physiotherapist who was a Ph.D. student in physiotherapy performed all marker placements in two sessions. Participants were asked to return for retest after 6–11 days following their initial visits [24]. This time interval was long enough to avoid assessor memory bias yet short enough to avoid change in gait pattern and clinical condition of CLBP patients [16]. Both tests were conducted at the same time between 9 and 12 o'clock of the morning to reduce the effect of diurnal variation in joint mechanics. All procedures were carried out by the same assessor.

Each participant performed 1–2 minutes of walking for warm-up. After a static trial, participants were asked to walk barefoot from one end of a marked 10-m walkway to the other at their self-selected walking speed. A total of six trials were performed in each test measurement.
Kinematic spine model
Trunk joint angles (using a XYZ Cardan sequence) were computed and expressed relative to the pelvis segment in three planes of movement well defined by Hidalgo et al. [21]. Thorax segment was modeled by placing three markers on bilateral acromial process and T12 spinous process. Lumbar segment was modeled by placing three markers on S2, L3, and T12 spinous processes. The pelvic segment was modeled by placing four markers on ASISs and PSISs on both sides. Thorax movements relative to the pelvis were calculated in three planes. Movement of the thorax segment was computed by the line connecting T12 to the midpoint of two AC markers. Total lumbar segment was computed by two markers connecting S2 and T12. Pelvis segment movements were computed using four markers on ASISs and PSISs. Movement of the thorax and total lumbar segments in frontal planes were calculated using thorax and lumbar markers relative to the line connecting the mid-point of ASIS-PSIS in the left to the right side. Sagittal plane movement was calculated using thorax and lumbar segments relative to the line connecting mid-points of ASISs to PSISs markers. Transverse plane movement of the thorax was calculated using AC markers relative to the line connecting ASIS-PSISs bilaterally.
Movements of upper and lower lumbar spine were defined as described previously by Parkinson et al. [18]. Lumbar segments were divided in two upper and lower parts. Upper lumbar movements were calculated using the line connecting T12 to L3 relative to T12-S2 markers (‘a’ angle in Fig. 2). Lower lumbar movements were calculated by the line connecting L3-S2 relative to T12-S2 markers in sagittal plane (‘c’ angle in Fig. 2). Lumbar lordosis was calculated using the angle created between lines connecting T12-L3 and L3-S2 markers in sagittal plane (‘b’ angle in Fig. 2) as described by Whittle and Levine [29]. The ‘b’ angle is one that the lumbar lordosis is taken place during walking [29]. Data were normalized to 100% gait cycle. Peak values for thorax and lumbar angles relative to the pelvis segment were computed for each cycle and averaged for each participant. Gait cycle was considered as the time from the initial right heel contact (0%) to the following initial right heel contact (100%). Heel contact was identified as the lowest vertical displacement of a right heel marker.
Data analysis
ICCs and their 95% confidence interval (CI) for the two-way random model were calculated for each trunk segment peak displacement as angular kinematic measures. The mean difference (D) between two measurements at time 1 and time 2 was also calculated. SEM, SEM%, and the minimal detectable change (MDC) were calculated using the following equations:

where SD is the standard deviation for all observations, x represents sessions 1 and 2, and R is the test-retest reliability coefficient (ICC) for sessions 1 and 2 [21].

where mean is the mean of all observations in sessions 1 and 2. SEM% represents measurement error independent of the unit of measure. It indicates the limit for the smallest change indicating real improvement [21].

where 1.96 is the two-sided table z value for 95% CI, and √2 is used to account for variance in the two measurement sessions [21].
is used to account for variance in the two measurement sessions [21].
is used to account for variance in the two measurement sessions [21].Go to :
RESULTS
Forty participants (20 males and 20 females) with NCLBP were included in this study. Their demographic characteristics are summarized in Table 1. Male participants had mean pain score of 4.5 (±1.7) in numerical 100 mm VAS while female participants had mean pain score of 4.7 (±1.5). No significant difference in VAS pain score was found between male and female participants (paired t-test, p=0.44).
Inter-session reliability analysis
In the male group, inter session reliability analysis revealed ICCs of ≥0.81 for all trunk kinematic angles except for peak extension of the lower lumbar spine (ICC=0.67, 95% CI, −0.68 to 0.94). SEMs were generally ≤3.5° for all displacement angles in males except for peak thorax rotation L/R (4.8°). Their MDCs ranged from 0.4° to 13.2°.
In the female group, inter session reliability analysis revealed ICCs of ≥0.79 for all trunk kinematic angles except for peak flexion of the lower lumbar spine (ICC=0.51, 95% CI, −1.4 to 0.90). SEMs were ≤3.1° for females except for peak thorax rotation angle (5.3°). Their MDCs were ≤14.7°. In the lumbar spine, the upper segment had higher ICCs than the lower segment (ICCs ≥ 0.90). However, all upper and lower lumbar movements had SEM ≤1.66°.
Male participants had an ICC of 0.67 for peak extension displacement while female participants had an ICC of 0.51 for peak flexion displacement. Other movements of the lower lumbar spine had ICC higher than 0.86. However, upper lumbar spine had MDC between 0.4° and 2.2°. Lower lumbar spine had MDC between 0.8° and 4.6° (Table 2).
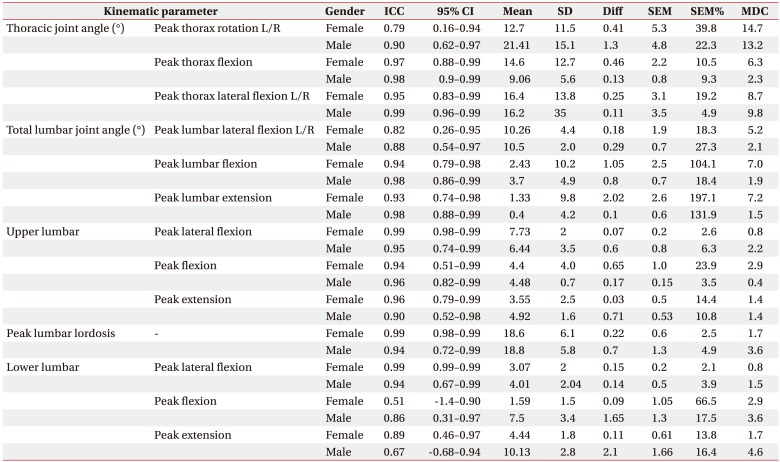
Table 2
Inter-session reliability values for kinematic parameters
ICC, intraclass correlation coefficient; 95% CI, 95% confidence interval for ICC; mean, mean of measurements at time 1 and time 2; Diff, mean of differences between measurements at time 1 and time 2; SEM, standard error of measurement; SEM%, standard error of measurement, expressed as a percentage; MDC, minimal detectable change.
![]()
Intra-session reliability analysis
In male group, intra-session reliability analysis showed ICCs of 0.91–0.96 for thorax-pelvis movement angles and ICCs of 0.75–0.87 for lumbar-pelvis movement angles. SEMs were ≤4.5° except for peak thorax lateral flex L/R (10.2°). Their MDCs ranged from 0.3 to 28.4.
In the female group, intra-session reliability analysis demonstrated that ICCs ranged from 0.68 to 0.96. SEMs were ≤5.3°. Their MDCs ranged from 1.06° to 14.6°. In the upper lumbar spine, ICCs ranged from 0.75 to 0.96 for the male group and from 0.81 to 0.87 for the female group. In the lower lumbar spine, male group showed ICCs ranging from 0.66 to 0.92 while the female group showed ICCs ranging from 0.68 to 0.84. The upper lumbar had higher ICCs than the lower lumbar in both groups. SEMs ranged from 0.3 to 1.7 for the upper lumbar and from 0.3 to 2.8 for the lower lumbar (Table 3).
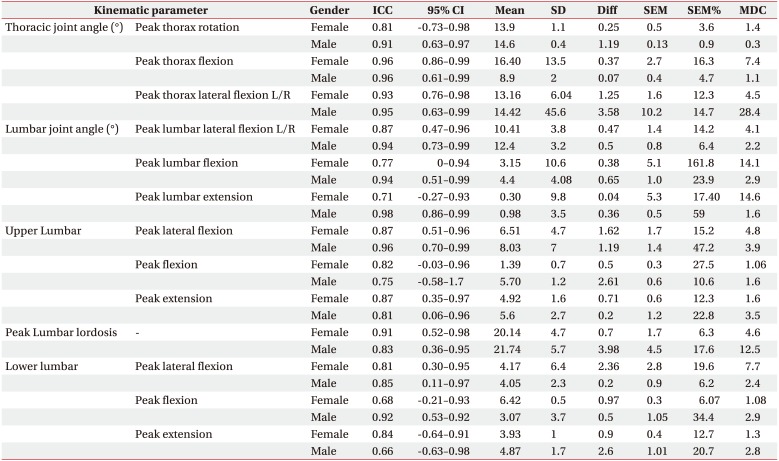
Table 3
Intra-session reliability values for kinematic parameters
ICC, intraclass correlation coefficient; 95% CI, 95% confidence interval for ICC; mean, mean of measurements at time 1 and time 2; Diff, mean of differences between measurements at time 1 and time 2; SEM, standard error of measurement; SEM%, standard error of measurement, expressed as a percentage; MDC, minimal detectable change.
![]()
Go to :
DISCUSSION
This study aimed to investigate the test-retest reliability of the 3D motion capture system to analyze trunk kinematic measures during gait in two groups (males and females) of patients with NCLBP. Results showed that ICCs were relatively constant but small in certain variables. The reliability of the inter-session was higher than that of the intra-session. This illustrates that the variability between study objects (i.e., marker positioning, within subject, and between subject variability) was very small. In addition, the measurement error remained constant and SEM difference was large between males and females. Koo and Li [32] have suggested that true variance can be stated as a main parameter affecting reliability mathematically. However, error variances are generated from soft tissue artifact and between-trial movement variability [10]. In our study, such high ICCs indicate that the extent to which measurements can be replicated by this kinematic model is highly reliable. Our results revealed some gender differences in lumbar spine kinematic between females and males, consistent with previous studies [2223]. Most segments had similar range of ICCs during inter-session and intra-session analyses. However, a gender difference was seen in total lumbar segment ICC. Intra-session ICCs in frontal and sagittal plane movement in the male group were greater than those in the female group. According to results obtained for the lower lumbar spine, peak flexion in the female group and peak extension in the male group revealed moderate ICCs on inter-session and intra-session analyses, in line with some studies showing that the lumbar spine sagittal plane movement kinematics had poorer ICCs relative to the frontal plane [21]. However, some negative values accounted for 95% CI in some variables in lower lumbar motions. Correlation coefficients might be affected by the range of variation for the parameter within the sample and large variations between subjects can result in higher ICCs. Negative value in 95% CI has been reported for some segments in CLBP patients in previous studies [2425]. Such negative value could be due to relatively small between-subject variation compared to withinsubject variation in our study. In addition, some tests (trials) might have been replicated in a reverse pattern compared to others. This could lead to very severe disagreement relative to the amount of variance available.
Another finding of our study was that ICC in thorax transverse plane was lower than that in frontal or sagittal plane in both gender groups. This is in agreement with previous studies [142223]. It could be due to greater trial-to-trial variability and difference in patients' movement strategies in these planes [18].
Although the standard of reliability is ICC, criteria for agreement on how to correct the result from this measurement are clinically important. Accordingly, the SD×√(1−ICC method [21] was used for SEM. SEMs for most trunk and lumbar movements generally remained constant in both gender groups. It seems that there is a difference in SEM between men and women for deviation. Generally, females had higher SEMs relative to males in most trunk and lumbar movements except for lower lumbar sagittal plane movements. However, most of these observed error values could be due to higher SDs and higher between-day movement variability in this group (female) of patients [10] caused by gait disturbance due to CLBP. It has been reported that females have higher values of SDs of mean in most trunk and lumbar movements due to movement variability [18222332]. SEMs obtained in our study were lower than around 5° for both gender groups. These results are reasonable according to previous studies [1033]. However, when the measurement error is higher than 2°, this may require consideration during data interpretation [10]. This means that the difference between two measurements is small and these parameters are useful. They are particularly appropriate for detecting changes in these participants.
method [21] was used for SEM. SEMs for most trunk and lumbar movements generally remained constant in both gender groups. It seems that there is a difference in SEM between men and women for deviation. Generally, females had higher SEMs relative to males in most trunk and lumbar movements except for lower lumbar sagittal plane movements. However, most of these observed error values could be due to higher SDs and higher between-day movement variability in this group (female) of patients [10] caused by gait disturbance due to CLBP. It has been reported that females have higher values of SDs of mean in most trunk and lumbar movements due to movement variability [18222332]. SEMs obtained in our study were lower than around 5° for both gender groups. These results are reasonable according to previous studies [1033]. However, when the measurement error is higher than 2°, this may require consideration during data interpretation [10]. This means that the difference between two measurements is small and these parameters are useful. They are particularly appropriate for detecting changes in these participants.
method [21] was used for SEM. SEMs for most trunk and lumbar movements generally remained constant in both gender groups. It seems that there is a difference in SEM between men and women for deviation. Generally, females had higher SEMs relative to males in most trunk and lumbar movements except for lower lumbar sagittal plane movements. However, most of these observed error values could be due to higher SDs and higher between-day movement variability in this group (female) of patients [10] caused by gait disturbance due to CLBP. It has been reported that females have higher values of SDs of mean in most trunk and lumbar movements due to movement variability [18222332]. SEMs obtained in our study were lower than around 5° for both gender groups. These results are reasonable according to previous studies [1033]. However, when the measurement error is higher than 2°, this may require consideration during data interpretation [10]. This means that the difference between two measurements is small and these parameters are useful. They are particularly appropriate for detecting changes in these participants.As another current method for agreement, MDC was also considered in our experiment. MDC95 represents changes in variables falling outside of the measurement error and the magnitude of change necessary to exceed the measurement error of two repeated sessions [21]. In our study, MDC ranged from 2.3 to 14.7 for the thorax segment and from 0.4 to 7.2 for the lumbar segment. Generally, MDC was higher in the transverse plane movement of the thorax, in agreement with results of previous studies [2425]. The thorax segment had higher MDCs in the female group except for the peak lateral flexion displacement in inter-session and intra-session analyses. The total lumbar segment also showed higher MDCs in the female group. On the contrary, in the male group, the lordosis angle and the upper and lower lumbar segments had higher MDCs in most movement planes except for the frontal plane in intra-session analysis. Our results demonstrated lower MDCs for NCLBP, different from results of the study by Hidalgo et al. [21] showing that the thoracic spine had lower MDCs while the lumbar spine had higher MDCs. However, they evaluated the reliability of the trunk in CLBP with a wide range of ages (between 30–65 years) with a different task procedure.
To the best of our knowledge, the impact of gender on reliability of trunk kinematics during gait in patients with NCLBP has not been reported yet. We observed relatively constant ICCs which were higher in the male group for some variables. Sagittal plane movements of the lower lumbar were too small to be easily interpreted. Accordingly, SEMs and MDCs that represent the agreement are clinically important. There were differences in SEMs between females and males. This could be due to higher SDs in the male group in these motions of the lumbar spine. Therefore, we recommend the use of agreement (SEM and MDC) rather ICCs in sagittal plane movement displacement in the lower segment of the lumbar spine obtained with this device for clinical utility.
The strength of our study was that two measurements were separated by 6–11 days and the assessment occurred at the same time of day. Since reliability may vary across different levels of low back pain severity, we included patients with similar range of pain intensity according to VAS (pain score of 3 to 6) [26]. Our study had some limitations. First, we did not conduct intra-tester reliability of kinematic data during gait. Another limitation of our study was that we did not evaluate the effect of different walking speed on spine kinematics reliability or measurement error. Since previous works have revealed that trunk and lumbar kinematics can vary in higher walking speed in patients with CLBP [9], further research with different walking speeds would be beneficial.
In conclusion, results of this study showed high test-retest reliability for most trunk joint angles during gait in CLBP individuals with low measurement error and MDC. Most joints had similar range of ICCs in both genders with a small superiority for the male group. Most trunk kinematics measurement parameters obtained using the 3D motion capture system were sufficiently reliable to be used for gender comparison during gait in NCLBP participants. However, there was difference in SEM due to difference in SD between males and females caused by different gait disturbance in CLBP. Thus, attention is needed when measuring lumbar motion using the method described in this study due to the increasing tendency of measurement error for other areas of men and women.
Go to :
 XML Download
XML Download