

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Type 2 diabetes mellitus (T2DM) shares similar risk factors and pathogenesis with gestational diabetes mellitus (GDM) and is known to be associated with vitamin D deficiency (VDD) [123]. However, evidence for a relationship between VDD and GDM has been inconsistent. While several studies reported a non-significant association between serum vitamin D level and GDM [45678], other studies showed that serum vitamin D was inversely related to GDM risk [910111213], with women with serum 25-hydroxy vitamin D (25[OH]D) < 50 nmol/L having a higher risk of GDM [1415]. These inconsistent observations could be due to the timing of the serum collection (e.g., early pregnancy, mid-pregnancy, post-GDM diagnosis), the accuracy of vitamin D (and its metabolite) assessment, the selection of the VDD cut-off values, as well as the influences of potential confounders and/or effect modifiers.
Accumulating evidence supports the role of vitamin D in glucose metabolism [1617], but the underlying mechanism requires further investigation. Vitamin D is thought to be essential in the development of insulin resistance due to its role in gene polymorphisms and metabolic/immune pathways. Gene polymorphisms of the vitamin D receptor, vitamin D-binding protein, and the vitamin D 1-alpha-hydroxylase gene could produce insulin resistance [171819] and disrupt the production, transportation, and action of vitamin D [17]. Numerous studies have suggested that the association might be due to pancreatic β-cell dysfunction, leading to impaired glucose metabolism, whereby vitamin D affects pancreatic β-cell function, insulin secretion, and insulin resistance, subsequently affecting blood glucose metabolism [1315]. Additionally, the active form of vitamin D (1,25-dihydroxyvitamin D3; 1,25[OH]2D3) has potent anti-inflammatory properties that could inhibit inflammation and the production of inflammatory cytokines that have a crucial pathogenic role in diabetes by promoting insulin resistance [2021]. Vitamin D is also involved in immune system development and function. A vitamin D receptor is located on most immunological cells [22], and the active form of vitamin D regulates circulating glucose levels by binding to the vitamin D receptor of pancreatic β-cells and modulating insulin secretion [2324]. The effects of VDD could increase insulin resistance and subsequently affect blood glucose metabolism, further contributing to increased GDM risk.
With the increasing trend in overweight and obesity incidence among reproductive-age Malaysian women, GDM is becoming a public health concern. The national prevalence of GDM in Malaysian women based on government hospital data, has increased from 8.7% (2010) to 9.3% (2017) [2526]. However, other small-scale studies have reported GDM in Malaysian women to be in the range of 11.4% to 29.7% [2728]. Despite the abundance of sunlight, approximately 59.8–90.4% of Malaysian pregnant women appear to be VDD [2930]. Previous studies showed that VDD is more prevalent among obese women with a higher GDM prevalence [7831], underscoring the importance of exploring the association between serum 25(OH)D level and GDM risk within this population. Other related factors include ethnicity, family history of T2DM, alcohol consumption, smoking status, and physical activity. Knowledge regarding a possible relationship between vitamin D status and GDM risk is important for developing public health actions related to preventive and curative measures. The present study aimed to identify the association between maternal vitamin D status and GDM and the potential influencers of that association.
Go to : 
SUBJECTS AND METHODS
Study participants
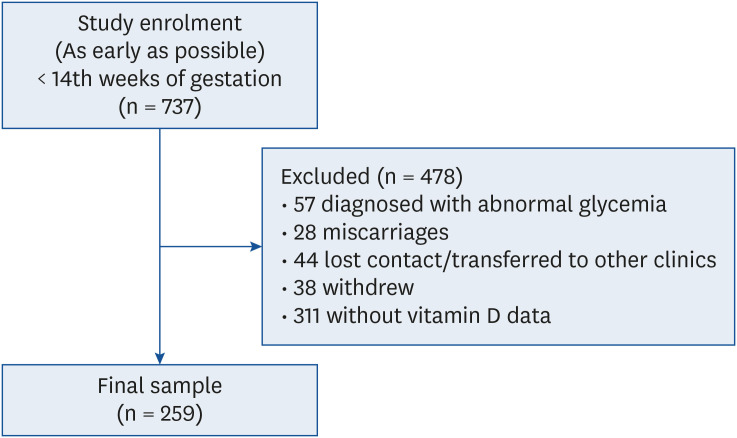
This study included 259 pregnant women from the Seremban Cohort Study (SECOST). Details of the study protocol have been published elsewhere [3233]. Fig. 1 provides an overview of the participant selection process. Ethical approval for the study was obtained from the Medical Research Ethics Committee (MREC), Ministry of Health (MOH) Malaysia (KKM/NIHSEC/08/0804/P12-613), and the MREC, Universiti Putra Malaysia (UPM/FPSK/100-9/2-MJKEtika). Prior to data collection, permission and informed written consent were obtained from the Head of Health Office of Seremban district and the respondents, respectively.
Measurements
Biochemical test
Fasting venous blood samples were drawn by clinic nurses on the subject's first prenatal visit (< 14th week of gestation) for determination of serum 25(OH)D level. Blood samples were transported on the same day to the laboratory for ARCHITECT 25-OH chemiluminescent microparticle immunoassay (CMIA) analysis. Subjects were then categorized as severe VDD (< 25 nmol/L), mild VDD (≥ 25 and < 50 nmol/L), vitamin D insufficiency (≥ 50 and <75 nmol/L), or vitamin D sufficiency (≥ 75 nmol/L) [34]. GDM status was diagnosed based on a 75 g oral glucose tolerance test conducted at 24–32 weeks of pregnancy. Fasting venous blood (2 mL) was drawn by clinic nurses before and after (2 hours) ingestion of a standard glucose solution. The GDM diagnostic criteria were fasting plasma glucose (FPG) ≥ 5.6 mmol/L and/or 2-hour plasma glucose (2hPG) ≥ 7.8 mmol/L [35].
Anthropometric measurements
A SECA digital weighing scale and SECA body meter were used to determine subjects' weight and height, respectively. Weight and height measurements at the first prenatal visit were used to calculate body mass index (BMI). Categorization of subjects based on BMI was based on World Health Organization (WHO) cut-off points: underweight (< 18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥ 30.0 kg/m2) [36].
Vitamin D intake
All women completed a 24-h diet recall. Dietary information was analyzed using Nutritionist Pro Nutrient Analysis Software: Version 1.5 [37] based on the United States Department of Agriculture (USDA) food database (Release 28) [38]. Women were also required to report on the use of dietary supplements during pregnancy. Vitamin D intake from supplements was estimated according to the manufacturers' product information. A subject's total vitamin D intake was estimated by summation of all intakes from food and supplements. Total intakes were divided into 2 categories: below recommendation (< 15 µg/day), above recommendation (≥ 15 µg/day) [39].
Other variables
Other variables included socio-demographic, obstetric, and physical activity information. Weekly energy expenditure was estimated using the Pregnancy Physical Activity Questionnaire (PPAQ) [40] and was expressed in metabolic equivalent (MET) hours per week.
Statistical analysis
Chi-squared test of independence, Fisher's exact test, and independent samples t-test were performed to determine the significance of differences in socio-demographic and obstetrical characteristics, dietary intake, physical activity, serum vitamin D level between GDM and non-GDM subjects, and total vitamin D intake based on early pregnancy serum vitamin D levels, as appropriate.
Binary logistic regression was implemented to examine the covariate-adjusted associations of serum vitamin D level and GDM status. The covariates included in the regression analyses were gravidity, family history of T2DM, early pregnancy BMI, physical activity, and intakes of energy, carbohydrate, and vitamin D. All variables entered in the models were examined for multicollinearity as well as interactions with serum 25(OH)D level and GDM risk. Stratified analyses were conducted if the interaction terms were significant. Results are presented as adjusted odds ratios (AORs) with a 95% confidence interval (CI). SPSS version 25.0 software (IBM Corp., Armonk, NY, USA) [41] was used for data analyses.
Go to :
RESULTS
Subject characteristics
The characteristics of 223 non-GDM and 36 GDM women are summarized in Table 1. For both groups, mean ages were similar, with a mean of 30.39 ± 4.53 years in non-GDM and 31.21 ± 3.62 years in GDM women. Almost all women (91.7–93.7%) were Malay. Most of the women were currently employed (63.9–74.4%) and had a secondary or lower education level (41.7–44.8%). GDM women had a significantly higher percentage of a family history of T2DM (50.0%) and higher gravidity (3.06 ± 1.41) compared with non-GDM women (family history of T2DM = 24.7%; gravidity = 2.40 ± 1.36). While 37.2% and 53.8% of the non-GDM women had a height of 1.55–1.59 m and a normal early pregnancy BMI, most GDM women were overweight (38.9%) and had a height of less than 1.55 m (44.4%). GDM women had a significantly greater mean serum 25(OH)D level (37.65 ± 10.79 nmol/L) than that of non-GDM women (32.05 ± 11.30 nmol/L, P < 0.05). None of the women's blood samples indicated vitamin D sufficiency. More than two-thirds of the subjects (68.3%) were categorized as having mild VDD, whereas 23.2% and 8.5% of women were categorized as having severe VDD and vitamin D insufficiency, respectively.
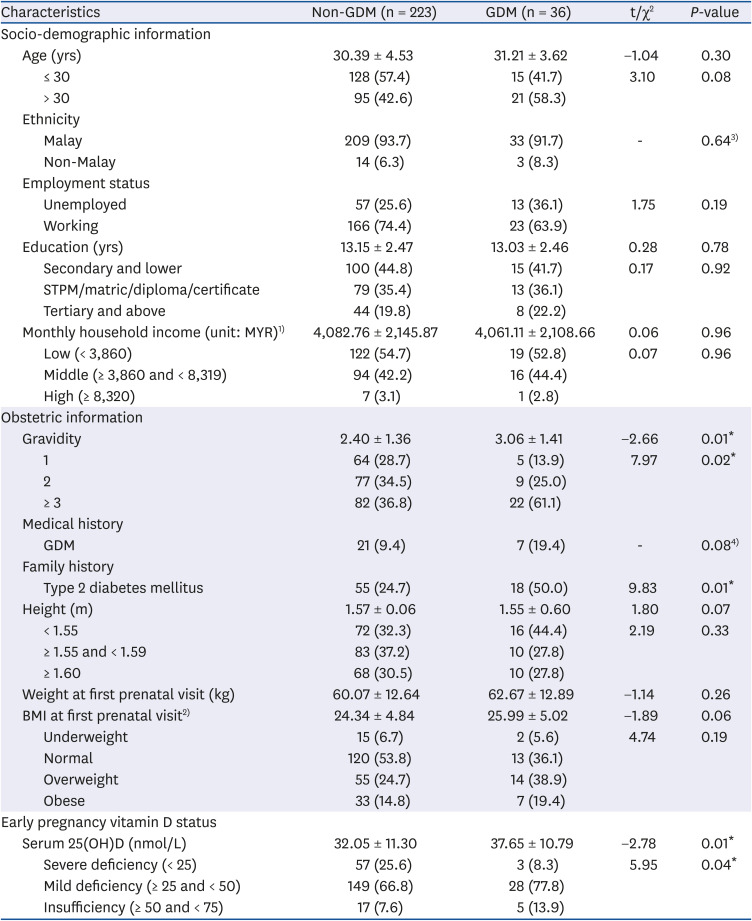
Table 1
Characteristics of women (n = 259)
Values are presented as mean ± SD or number (%).
STPM, Malaysian Higher School Certificate; MYR, Malaysian Ringgit; GDM, gestational diabetes mellitus; BMI, body mass index; 25(OH)D, 25-hydroxy vitamin D.
1) Economic planning unit, 2014: 1 USD = MYR 4.22 at the time of study; 2)< 14th weeks of gestation; 3)Fisher's Extract Test; 4)Description.
*P < 0.05.
![]()
Non-GDM women had a significantly higher mean intake of energy (1,567 ± 434.66 kcal) and carbohydrate (209.99 ± 61.59 g/day) compared with GDM women (energy, 1,390 ± 445.09 kcal/day and carbohydrate, 186.29 ± 64.37 g/day, respectively) (Table 2). The mean total vitamin D intake for GDM women (7.10 ± 1.17 µg/day) was lower than that of non-GDM (10.02 ± 0.58 µg/day) women, and a higher proportion of non-GDM women (69.5%) had a total intake of vitamin D below the recommended value (< 15 µg/day).
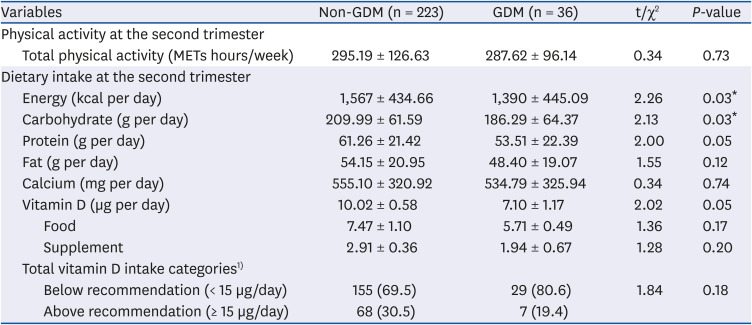
Table 2
Physical activity and dietary intake at the second trimester between non-GDM and GDM women (n = 259)
Values are presented as mean ± SD or number (%).
GDM, gestational diabetes mellitus; MET, metabolic equivalent.
1)Vitamin D: 15 µg/day (source: Malaysia Recommended Nutrient Intakes [RNI], 2017).
*P < 0.05.
![]()
Vitamin D intake by early pregnancy vitamin D status
There was no significant correlation between vitamin D intake and early pregnancy vitamin D status (r = 0.04, P > 0.05). Overall, non-GDM women had a higher mean total intake of vitamin D than that of GDM women, but a significant difference was only observed in women with mild VDD (t = 2.04, P < 0.05) (Table 3).
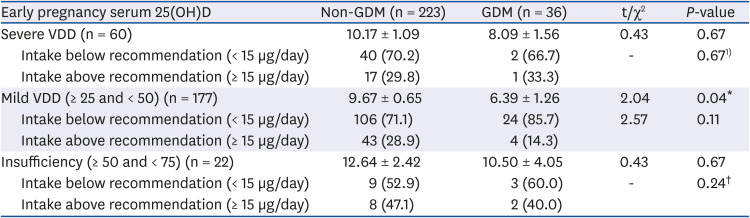
Table 3
Vitamin D intake by early pregnancy serum 25(OH)D among non-GDM and GDM women (n = 259)
25(OH)D, 25-hydroxy vitamin D; GDM, gestational diabetes mellitus; VDD, vitamin D deficient.
1)Fisher's extract test.
*P < 0.05.
![]()
Association between serum 25(OH)D level and GDM risk
Table 4 shows that women with a higher early pregnancy serum vitamin D level had a significantly higher risk of GDM (AOR = 1.05; 95% CI = 1.01–1.08). Significant interaction effects on GDM risk were detected between family history of DM (χ2 = 19.48, P < 0.05) and BMI (χ2 = 11.80, P < 0.05) with serum vitamin D level, but none of the socio-demographic factors significantly interacted with GDM risk. Stratified analyses showed that the significant positive association between serum vitamin D and GDM was only observed among overweight/obese and those with a family history of T2DM (Table 5).


Table 4
AOR and 95% CI for the association between serum 25(OH)D and GDM
Non-GDM is the reference group.
AOR, adjusted odds ratio; CI, confidence interval; 25(OH)D, 25-hydroxy vitamin D; GDM, gestational diabetes mellitus; DM, diabetes mellitus; BMI, body mass index; T2DM, type 2 diabetes mellitus.
1)Adjusted for gravidity, BMI, family history of T2DM, total vitamin D intake, energy intake, carbohydrate intake and physical activity; 2) Non-significant interaction terms: age, years of education, monthly household income, employment status, and gravidity.
*P < 0.05.
![]()
Table 5
The AOR and 95% CI for the associations between serum 25(OH)D with GDM stratified by family history of T2DM and BMI status
AOR, adjusted odds ratio; CI, confidence interval; 25(OH)D, 25-hydroxy vitamin D; GDM, gestational diabetes mellitus; T2DM, type 2 diabetes mellitus; BMI, body mass index.
1)Adjusted by gravidity, BMI, vitamin D intake, energy intake, carbohydrate intake and physical activity level; 2)Adjusted by gravidity, family history of T2DM, vitamin D intake, energy intake, carbohydrate intake and physical activity level.
*P < 0.05.
![]()
Go to :
DISCUSSION
Previous studies have reported inconsistent results indicating the relationship between vitamin D status and GDM [45678910111213]. The present study showed that women with a slightly higher serum vitamin D had an increased risk of GDM, despite all women having sub-optimal vitamin D status. Regardless of whether these results are due to the small sample size for women diagnosed with GDM (n = 36) or the small variance in the serum vitamin D levels, as most (up to 90%) of the women had mild/severe VDD, the detection of a positive association is worthwhile being investigated further, especially as it occurs among predominantly vitamin D deficient women and its interaction with other risk factors. It is worthwhile to note that although the adjusted odds ratio is small (AOR = 1.05), the narrow confidence interval indicates a high degree of certainty associated with the odds ratio [42].
In this study, the unexpected positive association of serum vitamin D level and risk of GDM was only observed in overweight/obese women and those with a family history of T2DM. Indeed, both family history of T2DM and BMI are well-established risk factors for GDM [4344]. Pregnant women with a family history of T2DM have approximately 2–4.5 times higher risks of developing GDM compared to women without family history of T2DM [45464748]. Increased body fat might increase insulin resistance and subsequently hyperglycemia [49]. Notably, GDM and T2DM share a similar genetic basis, which might be one reason for women with a first-degree family history of T2DM to be at risk for GDM [50]. Similarly, the present study results indicated that, in addition to the serum vitamin D level, family history of T2DM (AOR = 2.85; 95% CI = 1.34–6.05) and early pregnancy BMI (AOR = 1.07; 95% CI = 1.00–1.08) were significant independent risk factors for GDM. The observed positive association between serum vitamin D level and GDM among predominantly vitamin D deficient women with a family history of T2DM and/or overweight/obese BMI status, therefore, deserves further investigation. Regardless, these findings suggest that nutrition- and lifestyle-related approaches to GDM prevention should be implemented as early as possible, particularly for pregnant women with a family history of T2DM and an ‘at risk’ BMI.
The 91.5% prevalence of early pregnancy VDD (serum 25[OH]D < 50 nmol/L) in our study is similar to that in a local study (90.4%) conducted among pregnant women in Selangor [30], but higher than in studies in Western countries, such as the United States (10.0%) [51], Spain (22.7%) [52] and Netherlands (44.5%) [53]. However, the severe VDD (serum 25[OH]D < 25 nmol/L) prevalence of 23.2% in this study was much lower than in studies conducted in Turkey (45.9%) [54] and China (44.8%) [55]. To date, the “normal” or “optimal” level for serum 25(OH)D remains uncertain. While a serum 25(OH)D level of 50 nmol/L is considered to be acceptable by Institute of Medicine [34], experts of the Endocrine Group suggest a serum 25(OH)D level of 75 nmol/L for optimum calcium absorption, bone health, and multiple clinical outcomes [56]. Given the high VDD prevalence in Malaysian pregnant women, future studies to determine the optimal serum vitamin D and a safe level of vitamin D intake are urgently needed. It is also essential to develop effective monitoring and intervention strategies to ensure that pregnant women achieve at least a minimum serum 25(OH)D level of 50 nmol/L to prevent potential adverse health consequences in women and offspring.
In the present study, GDM women had a relatively low vitamin D intake but a slightly high mean serum vitamin D level than non-GDM women. This finding should be interpreted with caution, as the mean intake of vitamin D for both non-GDM (10.02 ± 0.58 µg/day) and GDM (7.10 ± 1.17 µg/day) women were below the recommended daily intake [39], which was established for populations with minimal exposure to sunlight and based on an intake level suitable for maintaining an adequate serum 25(OH)D level (> 50 nmol/L) [35]. The low total intake of vitamin D observed in the present study could be related to the limited availability of foods containing a high vitamin D level and the low incidence of vitamin D supplement usage [57]. It is also possible that women could have under-reported their vitamin D intake as the overall percentage of under-reporting was 27.5%, calculated using a cut-off EI/ER of ≤ 0.78 [58], with a greater proportion of under-reporting in GDM women (29.1%) than in non-GDM women (24.3%).
This study has several limitations that need to be taken into consideration. First, the relatively small sample of respondents with GDM (n = 36) and the limited variation in serum vitamin D concentrations could result in estimation bias. Second, as the majority of respondents were Malays and employed, they may did not represent the general pregnant population. Third, the use of percentage body fat as a measure of adiposity may have produced results different from those by BMI assessment. In addition, this study did not measure other diabetes predictors, such as plasma insulin and hemoglobin A1C, or oxidative stress markers, which could be used to explain the contribution of overweight/obesity status to the association between serum vitamin D level and GDM. Furthermore, this study did not measure vitamin D status in the second trimester of pregnancy. Finally, the accuracy of vitamin D intake estimation might be limited as the vitamin D from food sources was determined based on the USDA database and food labels of fortified foods [16]. However, the vitamin D contents of fortified foods in the Malaysian market compared to those in the USDA food database is not expected to vary significantly. Also, the vitamin D intake of supplements was estimated based on the supplement's label value.
Although VDD was prevalent in this sample of Malaysian pregnant women, a slightly higher serum 25(OH)D level within this sub-optimal range was associated with GDM, particularly among overweight/obese women and those with a family history of T2DM. Given the high prevalence of VDD, effective public health strategies aimed at preventing VDD are urgently needed due to the health significance of vitamin D. For women with multiple risk factors (e.g., overweight/obese and family history of T2DM), consultation on vitamin D status concerning the prevention of GDM could include an assessment of overall vitamin D intake (food and dietary supplement). Nevertheless, further investigation is warranted to confirm the relationship between vitamin D status and GDM in this predominantly vitamin D deficient population.
Go to :
 XML Download
XML Download