

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
As computers have prevailed and the Internet has developed, there has been a revolution in the work and lives of disabled people with cervical cord injury who have limitation of movement [1]. Patients with cervical cord injury who have surviving functions of their hands can input information into a computer by using a big-ball mouse, button mouse, touch pad, and usual mouse with rubber pad and so on [2]. However, for patients with high cervical cord injury, it is impossible to feed information by using the special input devices mentioned above, and therefore, it is difficult for them to work with a computer, lead a private life and be rehabilitated.
Recently, patients with high cervical cord injury can also input information into a computer by moving their heads, pupils and mouths due to the introduction of various computer interface devices available for them to do these functions without using their hands [2]. Nonetheless, as there is little information about the variety of computer interface devices available to them, most patients with high cervical cord injury are still using mouse sticks which are the most basic devices [3]. Moreover, although diverse computer interface devices should be assessed and applied properly according to the surviving physical functions, to date, there have been few reported cases of applying such computer interface devices to individuals in the country because most of these devices are high-priced.
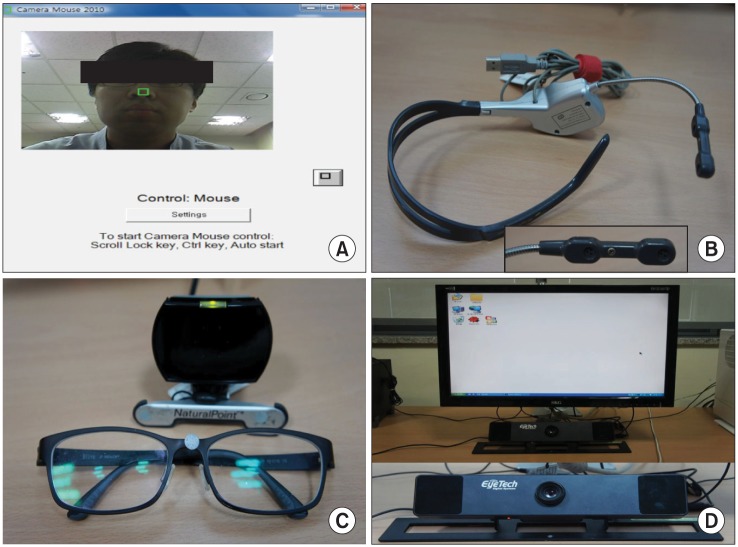
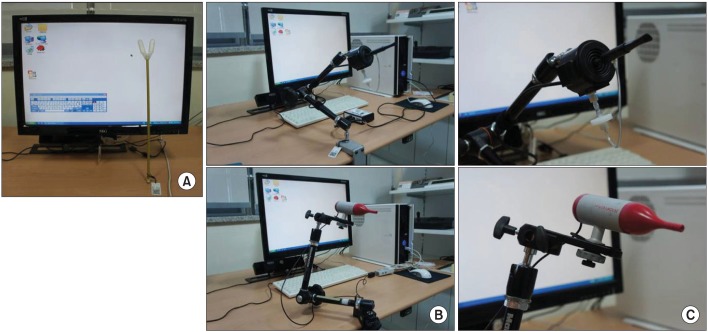
There are two classifications of the interface devices in accordance with the handling methods available to patients with high cervical cord injury. In the first classification, there is sensing of specific body parts, and included in this category are the Camera Mouse (Boston College and Boston University, Boston, MA, USA) (Fig. 1A) [4], Head Z mouse (RS Care Systems, Daegu, Korea) (Fig. 1B) [5], SmartNav 4AT (NaturalPoint, Corvallis, OR, USA) (Fig. 1C) [6], and Eyemouse4 (EyeTech Digital Systems, Mesa, AZ, USA) (Fig. 1D) [7]. The second classification, devices are operated with the mouth, for example, mouse stick and touch screen (Fig. 2A), Jouse2 (Compusult Limited, Mount Pearl, NL, Canada) (Fig. 2B), IntegraMouse (LifeTool Solutions GmbH, Linz, Austria) (Fig. 2C), and so on.
We have frequently experienced the problem of selecting suitable computer interface devices according to fine differences in the surviving functions of patients with high cervical cord injury. Therefore, to help patients select appropriate interface devices in accordance with their surviving functions, we will report three cases of application of special input devices.
CASE REPORTS
Case 1
A 49-year-old man injured his cervical cord from a fall 3 months ago. According to the American Spinal Injury Association Impairment Scale (ASIA)-A, he had a neurological level of injury C4, motor level C5/4, and sensory level C4/4. The surviving muscular strength was grade 3 of right-side C5, grade 1 of C6, and grade 2 of left-side C5. Pronation and supination of the right forearm were possible. Spasticity in the left and right upper arms was Modified Ashworth Scale (MAS) 0 and 1, respectively, and as he had been in management before the accident, he needed to use a computer to continue his work.
First, we tried a big-ball mouse, used with the right upper arm, but it did not work well. Seeing that his work required the use of both the computer and conversation, we tried out interface devices that sense the movement of specific body parts on the patient.
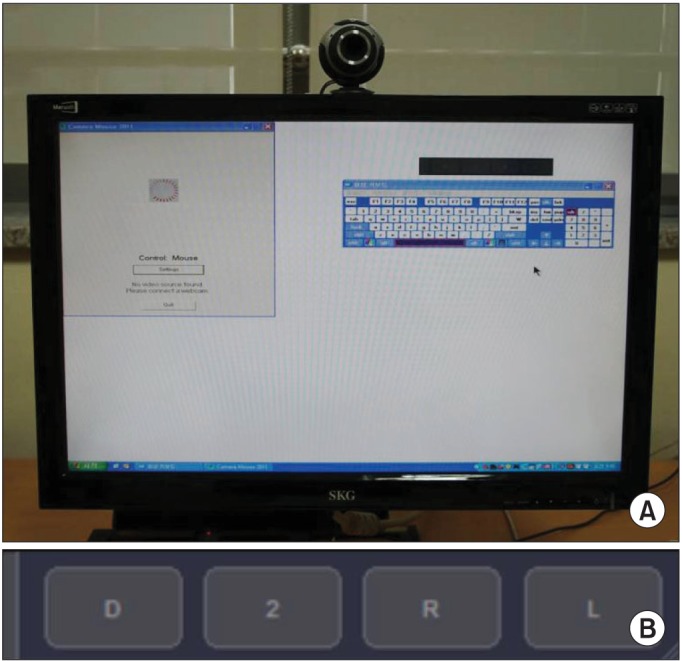
The patient was able to move the cursor by using the Camera Mouse and webcam with ease. However, while using the MintoClick 1.0 (http://jj21.org/wordpress/?p=274), a mouse button (Fig. 3B), to stop the cursor on the screen when clicking icons, because of vibrations of the tracking point, there were difficulties.
To move the left mouse button with pronation movements of the right forearm, we used micro light switch (Fig. 4A), but there were problems with accuracy and difficulty of repetitive motions due to narrow part of clicking. For this reason, the micro light switch was modified to make the block on which putting the whole of hands and to push one side or it with the whole of hands (Fig. 4B). By making this modification, the functions of click, double clicks and drag were easily performed through pronation movements of the forearm.
The cursor movement and clicking function were also implemented by applying Head Z mouse and SmartNav 4AT, but it was the easiest to input information though the Camera Mouse and modified micro light switch. He practised typing short sentences three times with the Camera Mouse, webcam, modified micro light switch, and screen keyboard (Fig. 4A), and as a result of the training, a typing speed of 16 wpm for typing with 100% accuracy was reported, which enabled him to control the business remotely.
For patients who can move one of their forearms, the Camera Mouse is an appropriate computer interface device, and it can be downloaded for free and can be used with any computer simply by changing the way clicks are made.
Case 2
Case 2 was a 41-year-old man who had a cervical cord injury from a diving accident 2 years ago. On the ASIA-A, this patient had a neurological level of C3, and a motor level and sensory level of C3/4. The muscle power of the surviving forearms was grade 1 on the right C5, grade 1 on the left C5, and forearm spasticity was MAS 0 for both forearms. The computer interface device sensing movements of specific body parts was applied rather than devices operated with the mouth, because he had been a used car dealer requiring the use of computer and consultation before the accident.
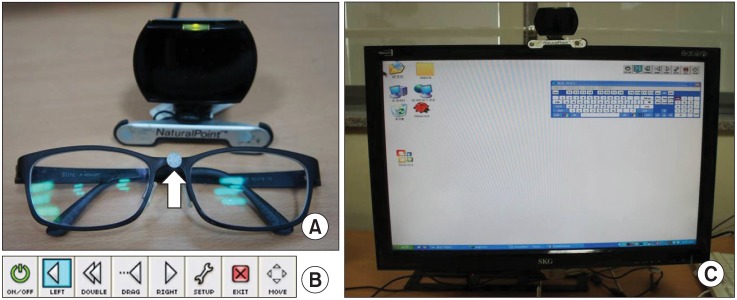
There was no difficulty in moving the cursor with the Camera Mouse and webcam, but there was difficulty when selecting a function of the mouse button using MintoClick 1.0 because of the vibrating tracking point. In the case of the Head Z mouse, the vibration of the tracking point was more stable compared to the Camera Mouse and webcam, but it was difficult to use consistently as a result of dizziness and increase in fatigue induced by the need for taking frequent breaths when selecting a mouse button. It was possible to click, double click and drag stably with the SmartNav 4AT, and cursor movement was the most stable with this device, and vibration of the tracking point was the least when selecting a function of the mouse buttons through its program (Dwell Clicking; NaturalPoint) (Fig. 5B).
Typing practice with short sentences was performed twice, resulting in a typing speed of 22 wpm with 100% accuracy by using SmartNav 4AT and screen keyboard (Fig. 5C), and he successfully returned to his previous job as a used car dealer.
Like this case, quadriplegics with motor level C4 can typically control the movement of the head, and SmartNav 4AT is considered to be the most suitable interface device when using computers.
Case 3
Case 3 was a 13-year-old ASIA-B patient who has hereditary neurofibroma with a neurological level of injury C1, sensory level C1/1 and exercise level, due to cervical cord compression by cervical kyphosis one year ago. The spasticity of the forearm was MAS 0 for both forearms. The patient had been staying in bed for months because of a pressure sore on her buttock, and she was breathing with a mechanical ventilator via a tracheotomy.
Jouse2 and IntegraMouse operated with the mouth were tried because the Head Z mouse and SmartNav 4AT were impossible to use due to difficulty in controlling head movements. It was not easy to move the cursor with Jouse2 because of weakness of her neck muscles, and functions of the mouse buttons were not able to be performed by inhalations and exhalations, because of weak breaths. However, the IntegraMouse was used easily because click, double click and drag were possible to be performed with a small breaths and fine movements of the lips. Online searching and email sending were possible by using the IntegraMouse and screen keyboard while staying in bed.
Thus, for patients with motor level above C3, who can only produce weak breaths and have difficulties in controlling their head movements, Jouse2 and SmartNav 4AT are not suitable, and IntegraMouse is proving to be the most appropriate interface device.
DISCUSSION
Advantages and disadvantages of a variety of computer interface devices
These are the advantages and disadvantages of various computer interface devices introduced in the country.
Camera Mouse chooses a tracking point on specific parts of the face appearing on the screen, by interlocking with webcam and MintoClick 1.0 (Fig. 3A). A cursor moves along with it, and the functions of mouse buttons were chosen by putting the cursor on each button of MintoClick 1.0 (Fig. 3B). It is possible to download the software for free and it can be used with any computer that uses a webcam. Meanwhile, the function of the mouse buttons was difficult to set up due to vibrations of the tracking point.
For the Head Z mouse, a cursor is moved by a Gyro sensor that senses head movements inside the headset. The left and right mouse buttons are clicked and selected by two sensors inside a microphone sensing the pressure made with the lips. Even though the vibration of a tracking point is stable, resulting in more stable cursor movement than the Camera Mouse, it is not suitable for patients with cervical cord injury and weak breaths due to the need to take frequent breaths when choosing mouse functions.
SmartNav 4AT moves a cursor sensing a reflector (Fig. 5A) with an infrared sensor, and its program (Dwell Clicking) is used to click. It is easy to choose functions of the mouse buttons and to move the cursor because the tracking point is stable. If conversation is required while using a computer, this can be done preferentially before using the IntegraMouse.
With Jouse2, the user operates the cursor by biting the mouthpiece, and button functions are selected by inhalation and exhalation. It is difficult to use for a long time because of the wider range of cursor movements with this device than with the IntegraMouse, and so dizziness and fatigue due to having to take frequent breaths are the disadvantages of this device.
With the IntegraMouse, clicking and moving of the cursor can be done with a small breaths and movements of the lips (0.1 mm). The most stable and accurate movements achieved with this device are the advantage, but this device would not be used if the work requires conversation.
Selection of computer interface devices ac cording to surviving functions
Like case 1, the patient with one-side motor level C5, if choosing a stable way to click applying a variety of switches, expected tasks can be conveniently performed with any computer by installing the Camera Mouse for free. As in case 2, Head Z mouse, SmartNav 4AT, Jouse2, and IntegraMouse can be applied to patients with typical motor level C4 who cannot use both upper arms. For the patients who need to talk to others for work, the Head Z mouse and SmartNav 4AT would be appropriate. However, the Head Z mouse has the limitation of causing dizziness and fatigue due to the need to take frequent breaths when selecting functions of the mouse buttons, so SmartNav 4AT is considered to be more suitable for patients with a high cervical cord injury.
Like case 3, the Integra mouse would be the most suitable interface device to use for patients with weak breaths and who can only make fine movements and for patients who cannot keep their necks balanced and breathe normally.
In addition, Eyemouse4 can be applied to patients with locked-in syndrome, who find it almost impossible to make even fine movements of the lips.
In this paper, proper interface devices were applied to patients with high cervical cord injury in accordance with the purpose of use and the surviving physical functions of the patients, consequently helping them to lead their private and recreational lives and to be rehabilitated.
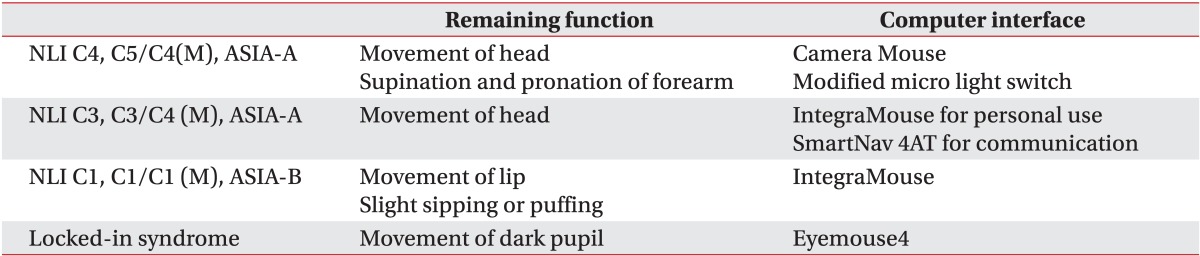
As a result, testing and application of suitable computer interface devices to further rehabilitation programs for patients with high cervical cord injury are needed, and the standard suggested by the paper (Table 1) may be helpful in selecting the appropriate interface devices according to the purpose of use and the differing surviving abilities of high cervical cord injury patients.

 XML Download
XML Download