

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Open fundoplication for gastroesophageal reflux disease (GERD), or antireflux surgery (ARS), was first developed by Nissen in 1956 [1]. Laparoscopic Nissen fundoplication was first performed by Dallemagne et al. in 1991 [2]. In Western society, this treatment was deemed the best way to treat GERD until proton pump inhibitors (PPIs) were developed. Although the use of medication to treat GERD has increased after the development of PPIs, the merits of ARS are remarkable in terms of economic efficiency because of the high cost of long-term PPI use [345].
In Korea, ARS is a recognized treatment option and covered under national health insurance, but it is rarely practiced due to concerns over invasive intervention. Meanwhile, the number of patients taking PPI medication and the cost of that medication increased 10.6 and 16.8 times from 2002 to 2013, respectively [6]. The efficacy and costs of the various GERD treatment options should be carefully considered due to the recent increase in the prevalence of GERD in Korea [78].
The efficacy of laparoscopic ARS is similar to drug treatment according to multicenter randomized trials conducted in Europe [91011]. Despite their small number, ARS results in Korea are comparable to those of Western countries [121314]. A recent Korean study compared the medical costs between ARS and PPI medication groups using nationally-representative sample data; however, the number of ARS patients was too small to perform a detailed comparison [15]. Furthermore, few data are available for even the basic features of ARS in Korea such as the number of people who underwent ARS and their general characteristics.
This study aimed to investigate the surgical volume of ARS using all national insurance claims, and compared the general characteristics, medical utilization, and costs for GERD treatment in Korean patients who underwent ARS and patients taking PPI medication.
METHODS
Data
We used customized cohort data extracted from the National Health Insurance Database (NHID). The NHID is generated using participants' medical bill expense claims filed with the National Health Insurance Service (NHIS) by medical service providers. Korea has universal health care which covers 98% of the entire Korean population. Thus, the NHID contains medical information for nearly all of the Korean population.
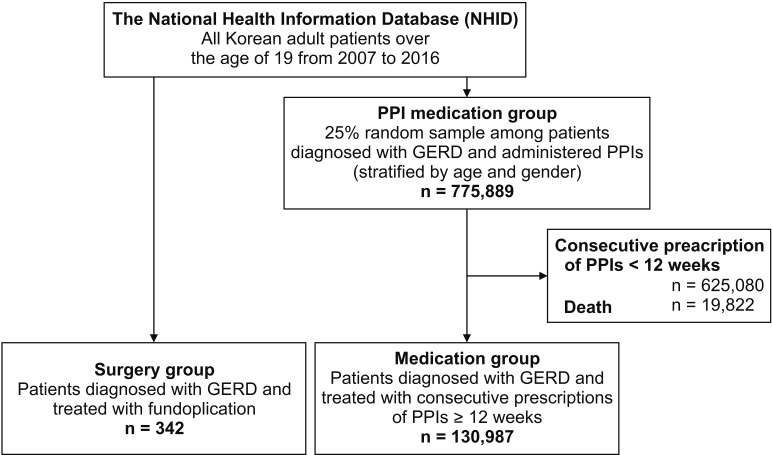
Fig. 1 is a flow chart of patients in the surgery and medication groups. The customized cohort was comprised of 2 treatment groups for GERD, surgery, and PPI medication. The surgical group was composed of all Korean patients who were diagnosed with GERD and underwent ARS between 2007 and 2016 (n = 342). Among the 342 patients, 12 died during the average 35-month follow-up period (n = 12). There were also 7 reoperation cases during the observation period, and the average interval between the first and second operations was 2.5 years. A GERD diagnosis was defined using the International Classification of Disease, 10th Edition, Clinical Modification (ICD-10-CM) as follows: K20.0, K20.9, K21.0, and K21.9. Fundoplication was confirmed using the corresponding surgical codes (QA424 and QA426). The medication group was selected with a 2-step procedure. First, we randomly selected 25% of all Korean patients who were diagnosed with GERD and who were prescribed PPIs between 2007 and 2016 (n = 775,889). The sample size was determined based on the distribution of mean daily dose of PPIs prescriptions in GERD patients [15] to include approximately 10 times more subjects with high dose PPIs compared to ARS cases. Second, a total of 130,987 patients were down-selected (n = 130,987) after excluding patients who had died (n = 19,822) and patients prescribed medication for less than 12 weeks (n = 625,080). The drug codes of PPIs were described in Supplementary Table 1.
The NHID released the data after anonymization and deidentification; therefore, informed consent could not be obtained from each patient. This study was approved by the Institutional Review Board (IRB) of Kosin University Gospel Hospital (IRB number: KUGH 2018-02-013).
Measures
The data included the sex, age, insurance type, household income, disease diagnosis, treatment, and prescriptions for each patient. Patients were categorized into 7 groups according to age (from 20 to 80 years or older). The insurance type was defined as self-employed, employed, and medical aid beneficiary. Household income was separated into 5 groups based on the 20 levels of insurance fees (a low level represents a low household income). Health status at baseline was measured using the Charlson Comorbidity Index (CCI), which is scored according to the presence of 17 types of chronic diseases and their severity [16].
The prescription of PPIs was defined using the active ingredient codes of lansoprazole, dexlansoprazole, omeprazole, pantoprazole, s-pantoprazole, rabeprazole, ilaprazole, and esomeprazole. Consecutive PPI prescriptions included those administered 7 days after the last date of the previous prescription period. The duration of consecutive prescriptions was calculated based on the number of prescription days after excluding overlapping days of multiple prescriptions and the number of days between prescriptions. We calculated the average prescribed daily dose (PDD) of PPIs for 12 weeks, the consecutive prescription period of PPIs, and then categorized patients into 4 groups: <standard dose, standard-double doses, double-triple doses, and ≥ triple doses.
Medical expenditures were defined as the total costs (inpatients cost, outpatients cost, PPI cost, and other drugs cost) for GERD treatment in medical care institutes covered by an insurer or a beneficiary. The average monthly costs for each group were calculated as the sum of the total medical costs divided by the follow-up months; thus, differences in the observation times for GERD treatment could be considered. Medical costs were adjusted for inflation using the consumer price index (CPI) for medical care [17]. The CPI for medical care is a measure that examines the weighted average of prices of a basket of consumer goods and services such as medication costs, medical costs, dental costs, etc. [18]. In our analysis, we calculated the inflation multiplier that was the relative value of each year based on 2016 and applied it to medical costs by year. Costs were presented in US dollars and calculated based on the exchange rate of Korean won 1,000.
Medical utilization included the number of hospitalizations, the number of clinic visits, and the number of Emergency Department visits for GERD treatments. The average monthly utilization was calculated by dividing the frequency of medical utilization by the follow-up months. For the surgery group, the number of follow-up months was calculated from the last day of fundoplication operative care to December 31, 2016. Since the patient selection year varied from 2007 to 2016, the follow-up period varied from a few days to a maximum of 9 years. In the medication group, the follow-up time was calculated from the end date of consecutive PPI prescription for 12 weeks to December 31, 2016.
Statistical analysis
The means and standard deviations of the medical costs and utilization for GERD were estimated according to inpatient, outpatient, and prescribed drug costs (PPI costs and other drug costs). To distinguish between the costs of the surgery and follow-up care for GERD recurrence, the medical costs in the surgery group were divided into 3 parts: operation costs, costs within the first year after surgery, and costs from the second year after surgery. For the medication group, we calculated the mean costs according to the 3 PDD levels of PPIs. A 2-sample t-test was used to test the difference in mean costs between surgery and medication groups.
This study focused on the medical costs and utilizations for GERD treatment. Thus, we excluded cases of death in both surgery and medication groups to prevent the confounding due to the increase in medical cost for end-of-life care. However, only the estimation for fundoplication costs included all surgery cases because the number of operations was small and there were no deaths within 3 months after surgery. To compare the exclusions due to death between the 2 groups, the mortality rates were presented by age category as supplementary information (Supplementary Table 2).
All statistical analyses were performed using SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Table 1 shows the demographic distributions and comorbidities of the medication and surgery groups. A total of 342 patients underwent fundoplication for the treatment of GERD in Korea. Even though the number of patients undergoing surgery to treat GERD has increased recently, it is still rare (n = 4 in 2007, n = 7 in 2008, n = 8 in 2009, n = 16 in 2010, n = 22 in 2011, n = 29 in 2012, n = 64 in 2013, n = 61 in 2014, n = 46 in 2015, and n = 85 in 2016). The number of males and females were similar in both groups, but older subjects or subjects with a high CCI score were more common in the medication group than in the surgery group.
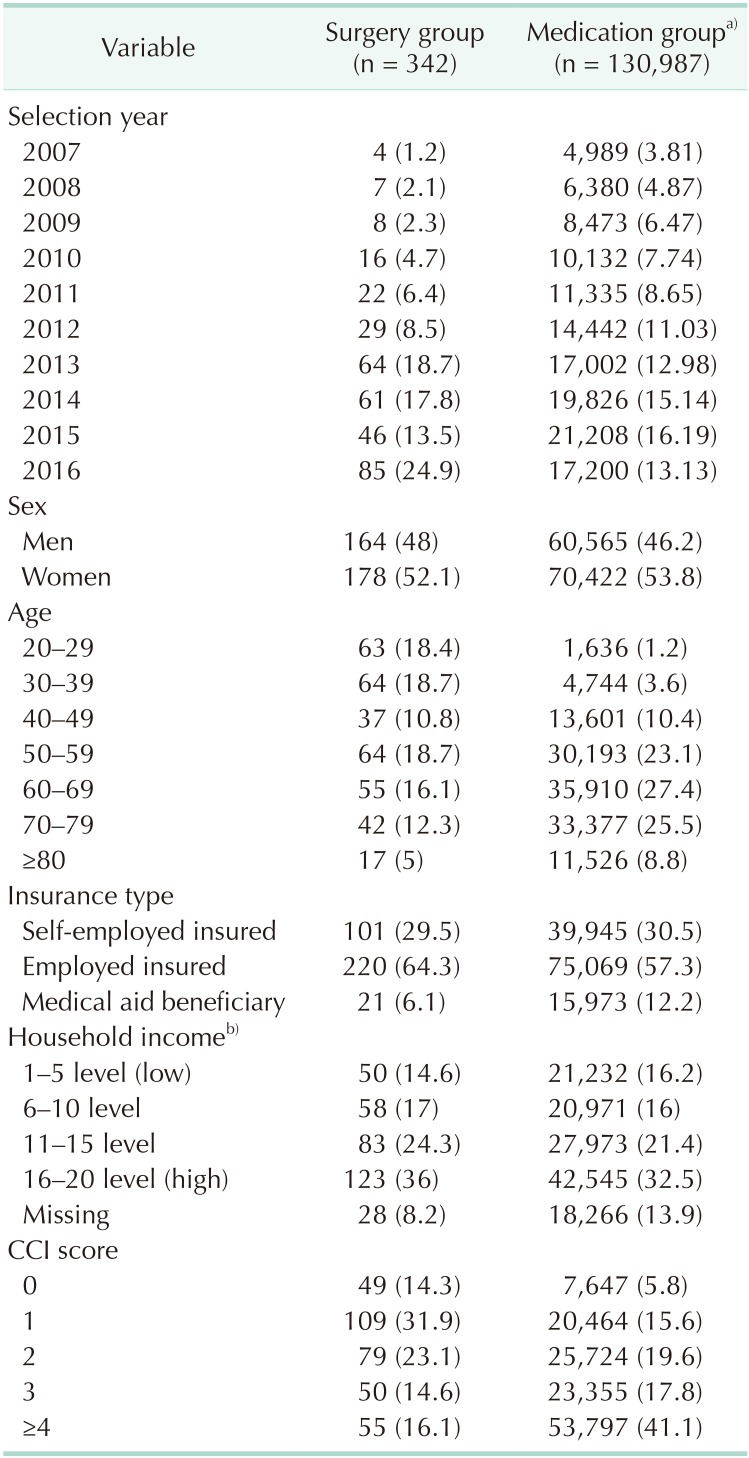
Table 1
The general characteristics of gastroesophageal reflux patients in the surgery and medication groups
Values are presented as number (%).
CCI, Carlson Comorbidity Index; GERD, gastroesophageal reflux disease; PPI, proton pump inhibitor.
a)Patients who had a GERD diagnosis and took PPI medication consistently for more than 12 weeks. b)Household income levels were based on insurance fees. A low level represents a low household income.
![]()
Table 2 presents the average medical expenditures for inpatients, outpatients, PPIs, and other drugs for the treatment of GERD in the surgery and medication groups. In the surgery group, the average cost associated with fundoplication was $4,631. The average cost within the first year after surgery was $78.10 per month. The follow-up costs were estimated to be $50.10 per month, which is approximately $28 less than the cost associated with the first year after surgery. In the medication group, the mean cost associated with GERD treatment was $137.50 per month. Considering the PDD of the PPIs, patients who were prescribed PPIs below triple doses spent an average of approximately $130 ($126.70–$136.60) per month. However, those who were prescribed PPIs over triple doses spent a monthly average of $165.00.
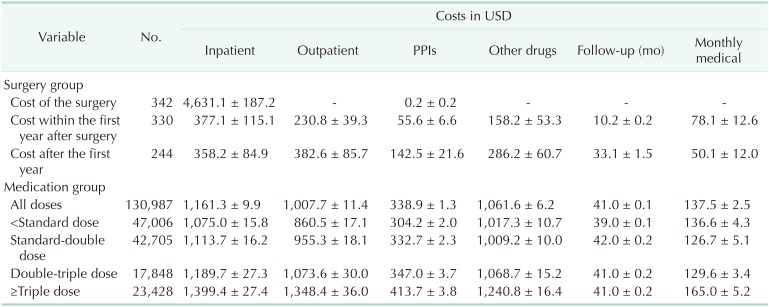
Table 3 shows the medical costs for GERD treatment by age group since the age distribution was different between the medication and surgery groups. Monthly medical expenses were lower in the surgery group than those in the medication group. Particularly, surgery patients in their 20s and 30s had 1/10 of the medical costs of their counterparts in the medication group.
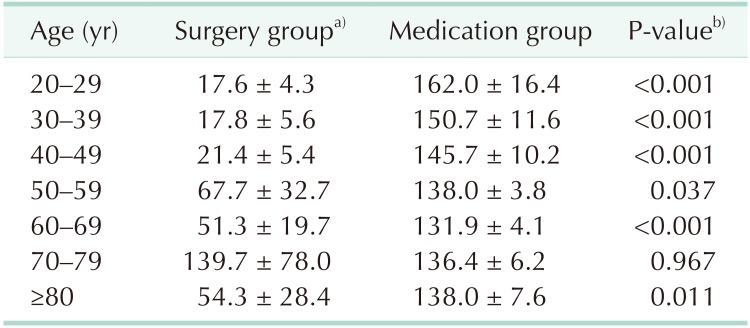
Table 4 shows the medical utilization for GERD treatment including hospitalization, clinic visits, and Emergency Department visits for both the surgery and medication groups. The frequencies of hospitalization, clinic visits, and Emergency Department visits were lower in the surgery group than in the medication group. The monthly frequency of hospitalization for the surgery and medication groups was 0.01 and 0.03, respectively. The average number of clinic visits per month was 0.45 for the surgery group and 0.72 for the medication group.

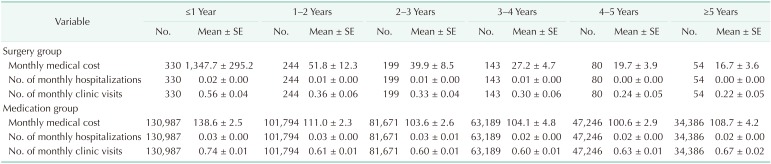
The follow-up costs and medical utilization for GERD treatment are presented in Table 5. During the first follow-up year, the monthly medical costs were approximately 10 times higher in the surgery group than in the medication group ($1,347.70 for the surgery group and $138.60 for the medication group). During the second follow-up year, the medical care costs for the surgery group dramatically decreased to an average of $51.80, and then they continued to decline (2–3 years: $39.90, 3–4 years: $27.20, 4–5 years: $19.70, and ≥5 years: $16.70). However, the medication group costs remained consistent at approximately $100 per month from the second follow-up year to the end of the follow-up period (1–2 years: $111.00, 2–3 years: $103.60, 3–4 years: $104.10, 4–5 years: $100.60, and ≥5 years: $108.70).
We calculated the mortality rate by age group to explore the distribution of excluding patients due to death. The results showed that age-specific mortality was higher in the medication group than in the surgery group among elderly patients aged over 70 years (Supplementary Table 2).
DISCUSSION
This study investigated the characteristics, medical utilization, and medical costs between GERD patients treated with ARS or PPI medication over the same period of time. ARS was performed mainly in younger patients and patients with fewer comorbidities. The ARS group showed better outcomes with respect to the length of hospitalization, number of outpatient visits, and number of Emergency Department visits. In terms of medical costs, the surgical patients paid 10 times more than the medication group in the first year after surgery, but their costs gradually declined over the years while costs for patients in the PPI medication group did not.
The lower, long-term medical utilization and costs in the surgery group might be evidence of the indirect benefits of ARS. A previous study conducted in the West also showed a cost decrease after ARS, rendering it more cost-effective than treatment with medication [1920]. Additionally, randomized control trials (RCTs) demonstrated that clinical outcomes measured by 24-hour esophageal pH monitoring, lower esophageal sphincter pressure, symptom improvement, quality of life, or patient satisfaction were better in patients who underwent ARS than in patients treated with medication [102122].
ARS is not a new treatment, and it is already covered under the national health insurance in Korea, but it is rarely performed. In our study, 342 ARS procedures were performed during the 10-year study period. However, no instances of mortality occurred within 90 days after ARS, and the reoperation rate was very low. Despite the small number of laparoscopic ARSs in Korea, the results were comparable to those from Western countries [121314].
We selected severe GERD patients treated with PPIs to compare the health utilization and the costs of the surgical group. The severe GERD was defined based on the definition of refractory GERD requiring more than 12 weeks of PPI treatment to treat GERD [2324], because refractory GERD is one of most important indication of ARS [2526]. When comparing the distributions of general characteristics between the 2 groups, sex distribution among patients was very similar. However, the age distribution was significantly different, which led to a discrepancy in the CCI scores between them. Thus, a subgroup analysis by age was conducted to compare the results between the 2 groups, and the monthly average medical costs by age group were presented.
Younger patients (20–40 years of age) who underwent ARS had one-tenth of the monthly medical costs after 1 year of their counterparts in the medication group. On the other hand, the medical costs among elderly patients in both groups were not significantly different. A study by Fei et al. [27] showed that the number of atypical symptoms was higher in the elderly, and the number of typical symptoms was higher in younger patients. In addition, elderly patients are more likely to have poor motility of the esophagus (dysmotility), which is predicted to be insignificant after antireflux surgery. These results collectively suggest that ARS may be more effective in younger patients than PPI treatments. Also, GERD in young people may require continuing PPI administration over a lifetime, and there are many potential side effects associated with the long-term use of PPIs, such as dementia, infection, etc. [28]. Well-controlled studies are necessary to clarify which patients are suitable for GERD surgery in terms of effectiveness as well as cost.
Considering the follow-up period in this study, the costs for patients in the surgery and medication groups within 1 year and after 1 year are almost the same ($55.60 per 10.2 months, $142.50 per 33.1 months, respectively; Table 2). The PPI cost within one year after ARS seems to reflect the PPI treatment on-demand after surgery, and this tendency may not have changed after one year. It may be interpreted that the use of PPI did not increase after ARS, and most of the patients did not relapse after surgery. In fact, the use of PPI after GERD surgery in foreign countries was less than 10% per year in RCT [9102930]. A recent multicenter prospective study on laparoscopic Nissen fundoplication for GERD also reported that less than 30% of Korean patients required any medication 3 months after the surgery [14].
This study investigated the treatment pattern (ARS and PPI treatment) of GERD using the national representative database. The strength of this study lies in its use of data from all ARS cases in Korea between 2007 and 2016. However, this study has several limitations. The claim database we used was not established for research purposes. Therefore, some information regarding clinical aspects such as disease severity, symptom change (relief or relapse), and laboratory assessment was missing. A GERD diagnosis was obtained using ICD-10 codes, and severe GERD patients were identified according to the refractory GERD definition (12 weeks of continuous PPI use) without clinical assessment. Even though we adjusted the inflation of medical costs using CPI, the cost changes during 10 years could not be fully accounted for in our analysis. Comparability between the medication and surgery groups was not guaranteed due to the different characteristics between the 2 groups (e.g., age and CCI score). Propensity score matching is one statistical technique that can remedy the imbalance of a covariate's distribution. However, an analysis using matching samples based on the characteristics of surgery cases may not be indicative of patients with GERD since ARS is rarely performed in Korea. Thus, we used an unmatched, random sample of GERD patients and alternatively conducted a stratification analysis by age group to overcome such drawbacks.
This study revealed the surgical outcome in terms of cost. Moreover, in the same way, this study indirectly suggests that GERD surgery may be more cost-effective in young adults. Further research on the clinical effectiveness (e.g., symptom recurrence) of ARS is needed to target the appropriate group for GERD surgery.
 XML Download
XML Download