

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Treatments for breast cancer are long and complicated processes, including surgery, chemotherapy, radiotherapy, endocrine therapy, and target therapy. During the long period of treatment, breast cancer patients experience several diverse psychological distresses, such as depression, anxiety, pain, and social isolation. This psychological distress is a normal and adaptive reaction to unpleasant stimuli or threats. However, it sometimes persists in some patients to where it may damage the individual's quality of life (QoL) [12], adherence to treatment [34], and even clinical outcomes [567] in breast cancer. Therefore, the American College of Surgeons Commission on Cancer and National Comprehensive Cancer Network recommended that cancer patients be routinely screened for psychological distress during the cancer trajectory.
Among psychological distresses, anxiety is very common and has been associated with cancer [1289101112]. However, most studies examining psychological distress have been focused on depression, and the concerns about anxiety have been relatively small compared to depression.
We conducted this prospective longitudinal cohort study to determine the QoL and psychological distress of breast cancer patients who were newly diagnosed with their respective diseases. In this report, we evaluated the temporal patterns of anxiety in patients who underwent breast cancer operations using the Hospital Anxiety Depression Scale (HADS), and found factors associated with persistent anxiety during breast cancer treatment. The HADS [13] is a standardized 14-item self-assessment instrument for the evaluation of anxiety and depression in patients with nonpsychiatric and physical illness (Supplementary Table 1). It has been frequently used in cancer research as a validated, brief and effective screening tool [14]. This was used in this study because it can be easily assessed without proficiency and the Korean versions of the HADS has been validated [15].
METHODS
Study design and population
This was a prospective longitudinal cohort study that followed consecutive newly diagnosed breast cancer patients 18 years and older from 2 different cancer hospitals in Seoul, Korea, between July 2010 and July 2011. Patients were asked to fill out preoperative questionnaires, and again at 2 weeks, 3 months, 6 months, and 12 months after surgery by themselves. If they had difficulties understanding or filling out the questionnaires, a nurse or trained research assistant helped them to complete the questionnaire.
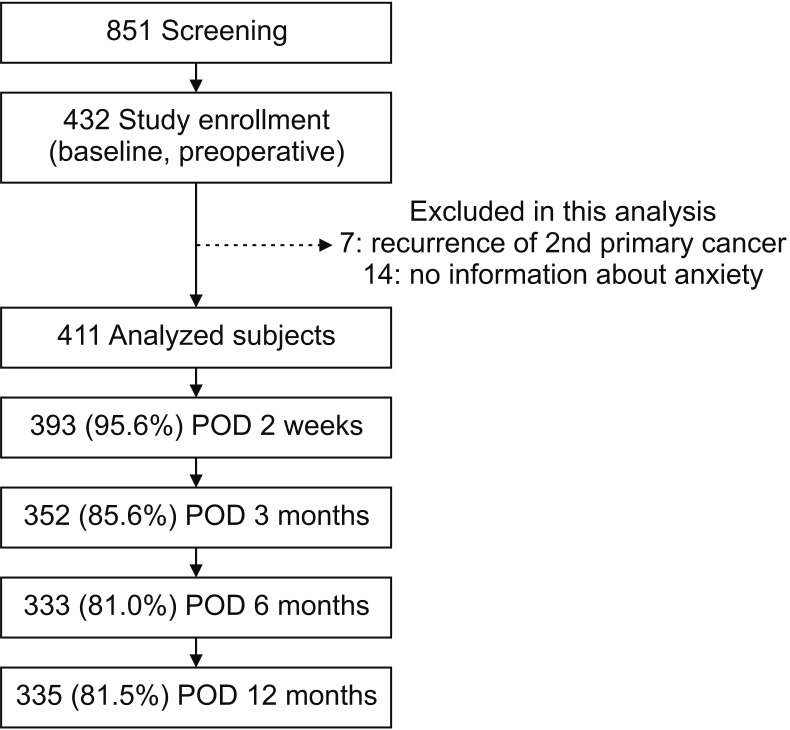
We included patients who underwent breast cancer surgery with pathologic stage 0 to III in this study (n = 851). We excluded patients who received neo-adjuvant treatment and had secondary cancer, or who did not understand the purpose of the study or had psychotic disorders at the beginning of the survey. Ultimately, 432 patients (50.8%) agreed to participate in the study. For the analysis of this study for anxiety disorder, 7 patients who had recurrence or a second primary cancer during follow-up and 14 patients who did not have the information about anxiety were excluded. The final analysis included 411 patients (Fig. 1). This study was approved by the Institutional Review Boards (IRB No. SMC 2010-05-069), and all study participants provided written informed consent.
Measurement
Anxiety was assessed using the patient's completed HADS, which is frequently used as a screening tool for psychological distress in cancer patients. A study was conducted to standardize the HADS for Koreans by Oh et al. [15], which demonstrated the validity and accessibility of the HADS, and we used this Korean version of the questionnaire for this study (Supplementary Table 2). There are 7 questions for the anxiety dimension in HADS (HADS-A) and each item is scored on a scale of 0 to 3, with a higher score indicating a more severe symptom. The scores can be categorized as; 0–7, normal; 8–10, borderline; and 11–21, abnormal. In this analysis, we considered cutoff scores of ≥8 as cases of anxiety including borderline and abnormal level based on the previous report [14].
We used a combined form of the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core 30 and the breast cancer specific module (BR-23), which has been translated into Korean and validated [1617]. Symptoms (breast and arm) were measured using the 7 questions of the BR-23. The BR-23 has 23 items to assess the impact of common breast cancer treatment modalities (surgery, chemotherapy, radiotherapy, or hormonal treatment). It includes questions about body image, sexual functioning, sexual enjoyment, and future perspective for function and questions about systemic therapy side effects, breast symptoms, arm symptoms, and distress over hair loss (Supplementary Tables 3, 4). We used additional measured questions related to sociodemographic and clinical characteristics, including age, marital status, income, education, employment status, religion, stage, breast surgery type, and treatment received.
Statistical analysis
Differences in baseline demographical and clinical characteristics were compared by the severity of the anxiety group using chi-square tests for categorical variables and t-tests for continuous variables. Multilevel models were used to assess how the severity of anxiety affected the level of change in the symptom level over time and case-wise deletion was used for the missing data. This method is functionally the same as growth curve modeling or mixed-effects models. The models were adjusted for baseline demographical characteristics and clinical characteristics, as shown in Table 1. Full-information maximum likelihood estimation was used to directly compare the fit of the nested models to the data and to use all variable data, given the presence of missing data at random. All analyses were conducted using STATA 12.0 (StataCorp LP, College Station, TX). P < 0.05 was considered statistically significant.
RESULTS
Characteristics of participants according to the preoperative level of anxiety
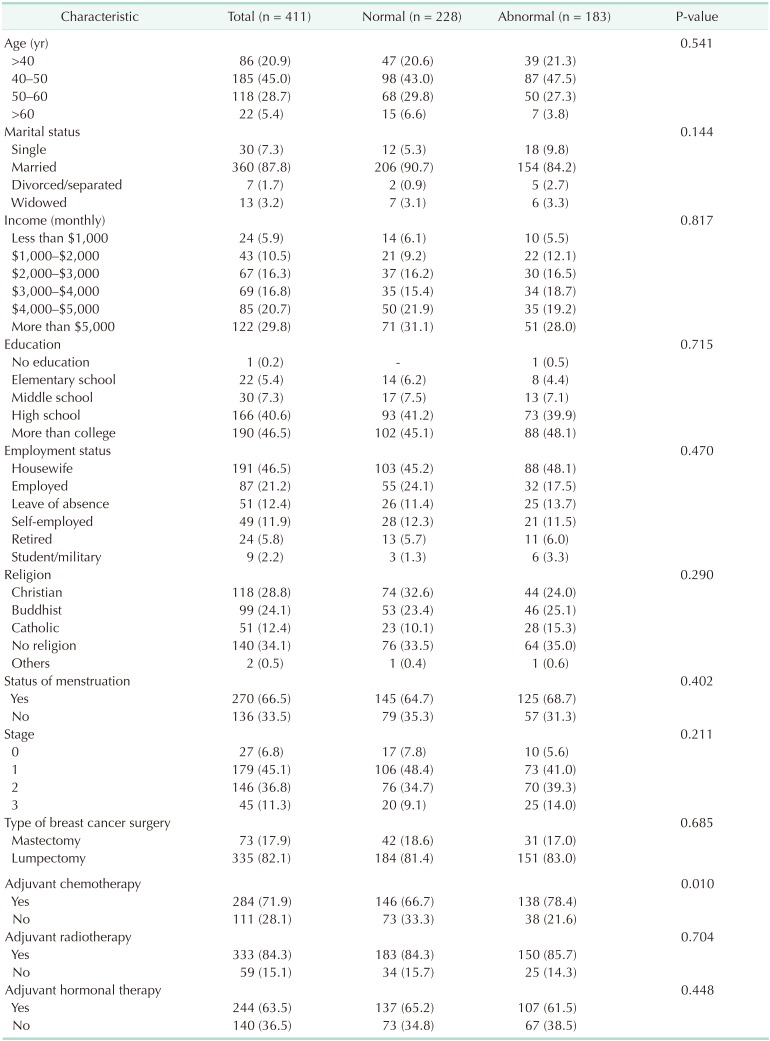
The characteristics of the 411 participants are listed in Table 1. A total of 183 patients (44.5%) showed abnormal levels of anxiety after diagnosis. The patients were regrouped into normal and abnormal groups based on the preoperative level of anxiety. We analyzed socioeconomic factors which could affect the baseline of anxiety; however, nothing was related with baseline anxiety. Age, marital status, income, statuses of education and employment, religion, and menstruation status were not associated with preoperative anxiety. Among clinical factors such as TNM stage and adjuvant therapy, nothing except adjuvant chemotherapy was related with baseline anxiety.
Temporal patterns of anxiety
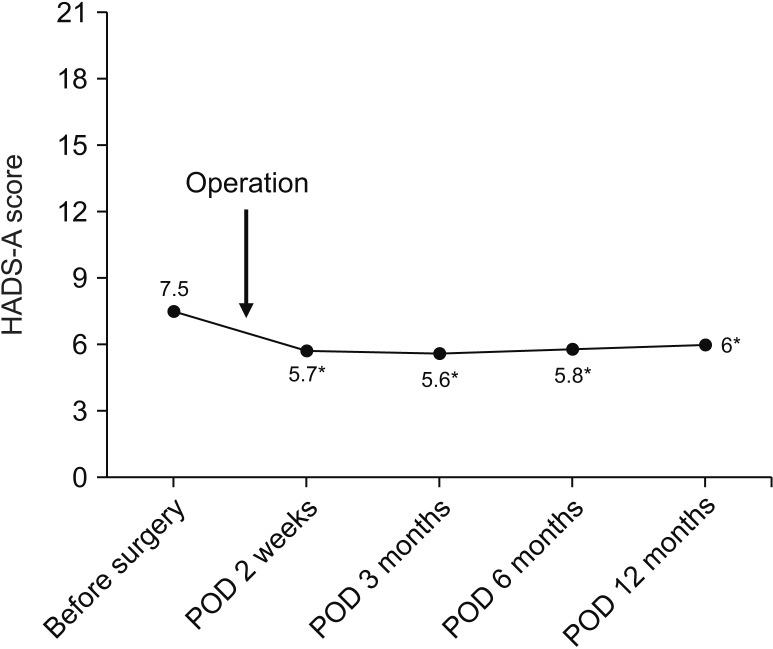
Among 44.5% (183 of 411) of the patients who showed abnormal levels of anxiety preoperatively, 89 patients (48.6%) showed a high score of anxiety (more than 11). After surgery, about half of the patients who had an abnormal level of anxiety preoperatively returned to normal (from 44.5% to 25.7%) (Table 2). We could see the highest level of anxiety at diagnosis with improvement after surgery. As shown in Fig. 2, mean HADS-A score decreased significantly from 7.5 to 5.7 immediately after surgery. The HADS-A score was sustained during the follow-up period; though slightly elevated again at 12 months after the surgery when main adjuvant treatments were completed.
Factors of associated with persistent anxiety
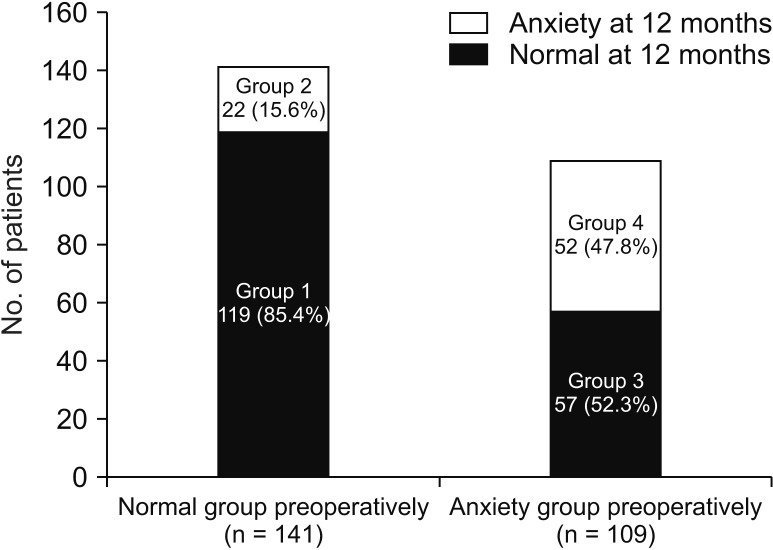
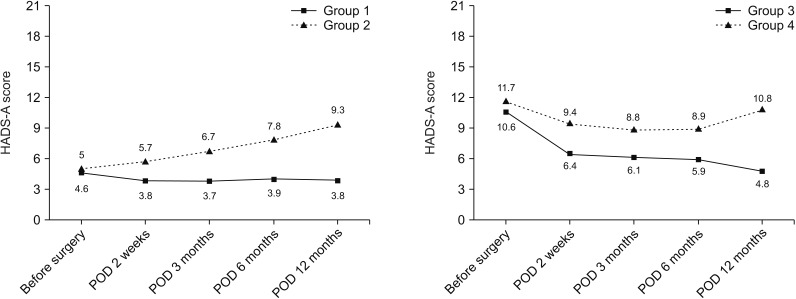
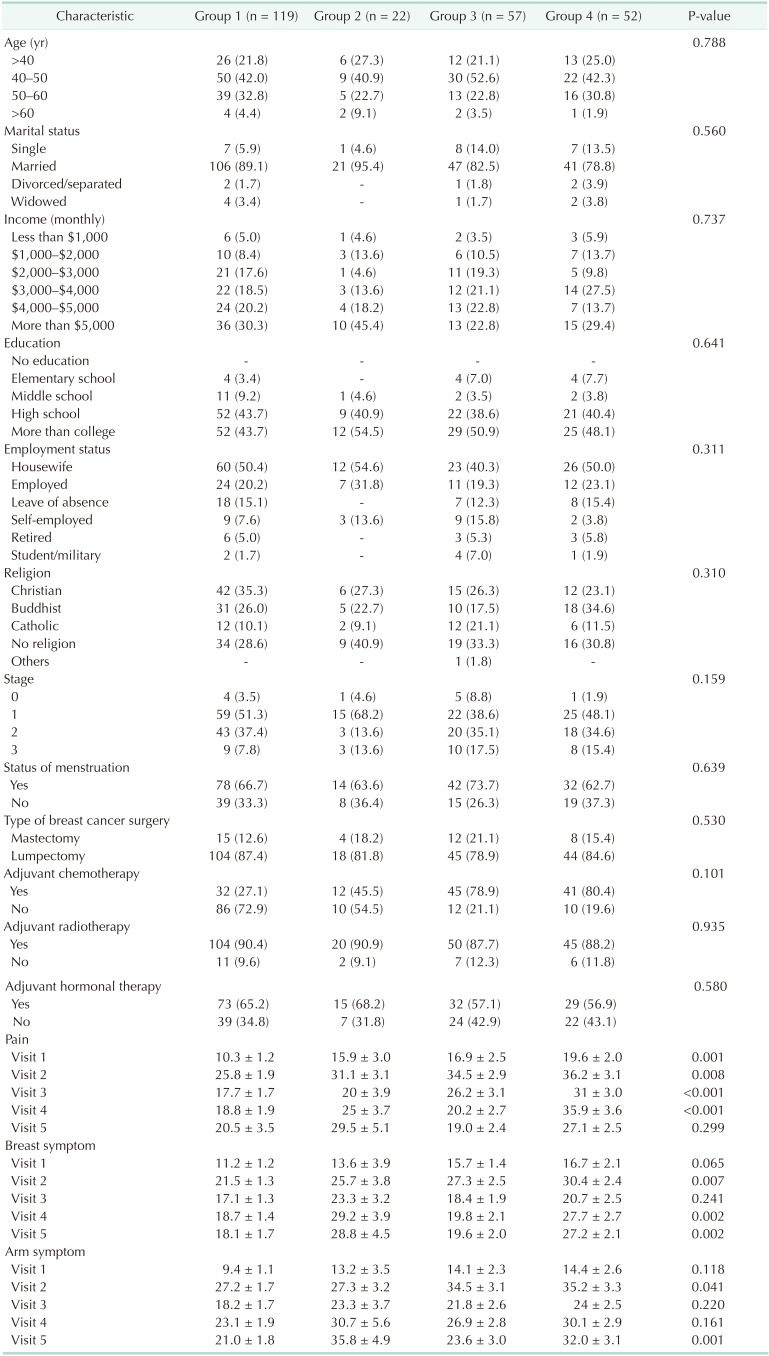
A total of 250 patients with complete longitudinal data about anxiety were analyzed during the follow-up period. We classified these patients into 4 groups: Group 1 (normal), group 2 (newly developed anxiety), group 3 (resolved anxiety), and group 4 (persistent anxiety). Among the 141 patients who showed normal anxiety levels preoperatively, 22 (15.6%) developed anxiety symptoms late, at 12 months (group 2). Fifty-seven patients (52.3%) who showed abnormal levels of anxiety at baseline were normalized 12 months after surgery (group 3). Nonetheless, 29.6% (74 of 250) were still suffering from persistent (group 4) or newly developed (group 2) anxiety (Fig. 3). Fig. 4 shows the temporal pattern of anxiety of each group over time. According to the level of baseline anxiety, overall mean scores and pattern of change were different from each other.
Socioeconomic and clinicopathologic demographics were not associated with persistent anxiety in our data (Table 3). Pain, breast, and arm symptoms were significantly higher in the newly developed or persistent anxiety groups (groups 2 and 4), especially at the time of visits 4 (postoperative day [POD] 6 months) and 5 (POD 12 months).
Comparison of anxiety level with regard to follow-up duration by breast cancer operation type
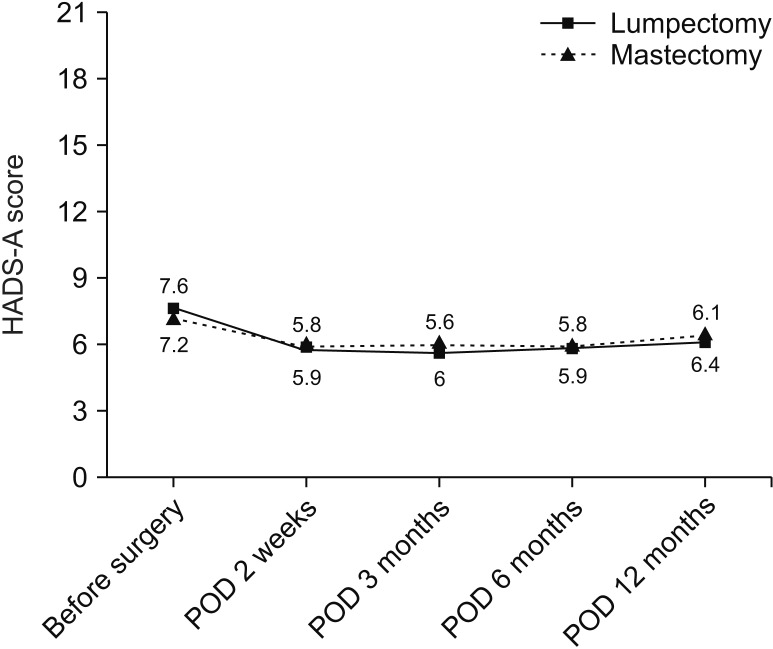
The anxiety level of the patients who underwent total mastectomy and partial mastectomy were not different (Fig. 5).
DISCUSSION
Previous studies have shown a diverse prevalence of anxiety, which depends on different criteria of the anxiety, diverse populations studied, differences in methodology used, and timing of measurement, ranging from about 20% to greater than 50% [1289101112]. In this study, we could see a high prevalence of anxiety after the diagnosis of breast cancer. The percentage of patients with anxiety in the normal range was just over half (55.5%). Pathologic or clinical levels of anxiety (scores more than 11) were shown in 21.6% patients.
In this analysis, we examined the temporal pattern of anxiety starting from cancer diagnosis. Many previous studies for anxiety in breast cancer patients were assessed crosssectionally during the courses of treatment with different cohorts [10]. Few researchers have reported anxiety level in relation to time progression; however, they did not show the baseline anxiety from diagnosis [21218]. Other previous studies demonstrated that level of anxiety was highest at diagnosis with improvement over time [1920], consistent with our data. However, these studies did not assess the anxiety level at immediate postoperative period, and could not show the effect of surgery itself on the anxiety.
Several studies showed distress trajectories including anxiety after cancer diagnosis [18]. Henselmans et al. [21] found that most breast cancer survivors within the first year postdiagnosis experienced no psychological distress (36.3%) or recovered to normal after completion of active treatment (33.3%), but small percentages of breast cancer survivors became distressed in the re-entry and survivorship phase (15.2%) or experienced persistent distress (15.2%) in the first year after breast cancer diagnosis. These are comparable with our study results in which 8.8% of patients became newly distressed in the re-entry periods (group 2) and 20.8% showed chronic anxiety (group 4) at month 12.
During the observation period of our cohort, there were 2 distinctive features. The first was rapid relief of anxiety after surgery. Patients were the most anxious before surgery, and this level of anxiety was sharply decreased after surgery. Understandably, this phenomenon was probably the fear of uncertainty about the cancer itself, treatment process, and outcomes. It could simply that surgery is a main relieving factor of anxiety; however, conversely, surgery itself is also a primary fear for patients after cancer diagnosis. Secondly, we could see the second rising of anxiety (re-entry) at 12 months. Most main adjuvant therapies were finished and the patients entered follow-up periods at this time. Several studies showed that anxiety generally decreased with time during the treatment period [8121822]. However, after completion of the treatment, the patients confront worries about leaving the health care system, uncertainty about the future, and the fear of recurrence [232425], and these could raise distress levels as in our results.
There have been many reports about the psychological distress associated factors in breast cancer [89101112222326]. Unlike these studies, in our study, socioeconomic factors, younger age, stage, social support, and mastectomy did not elevate anxiety. Adjuvant chemotherapy was preoperatively thought to be a risk factor of anxiety; however, after completion of chemotherapy, chemotherapy was not associated with elevated levels of anxiety. In our analysis, pain, and breast and arm symptoms were associated with persistent anxiety as in previous reports in which pain influences anxiety [81222].
There are some limitations to this study. This is a preliminary report with short-term follow-up data. Long-term follow-up results could provide the evidence and the reason for the reentry phenomenon. In addition to this, baseline distress, which was assessed preoperatively but not before diagnosis, did not reflect the real baseline (normal psychological) status of each person. If we have control cohorts (general population), the effect of breast cancer diagnosis on anxiety could be assessed more objectively. However, considering the result of previous research reporting that the prevalence of anxiety using HADS was 32.2% in generally healthy women [27], the breast cancer patients in our study seemed to suffer from anxiety more frequently after diagnosis. We needed also more information about previous mental health status because a past history of or pre-existing anxiety and/or depression before cancer diagnosis was known as an important predictor of anxiety [1928]. Regardless of these limitations, we have several important strengths. First is the design of this study. This is a prospective longitudinal study, and we could assess the psychological status from the preoperative period to 12 months. Also, our research was performed at clearly defined time points, including preoperative and immediate postoperative periods. Several prospective studies had much heterogeneity in assessment timing and did not assess the preoperative status.
In conclusion, anxiety disorder was common in patients who were diagnosed with breast cancer (44.5%). Surgery was a main relieving factor of anxiety and patients who finished their main adjuvant treatments experienced renewed anxiety. Surgeons should be the main detectors and care-givers for psychological distress in breast cancer patients during the time after diagnosis and completion of adjuvant therapy. To reduce persistent anxiety, taking care of physical symptoms is important.

 XML Download
XML Download