

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus-2, was declared a public health emergency of international concern on January 30th, 2020 by the World Health Organization (WHO) [1] and as pandemic situation on March 11th, 2020 [2]. Thereafter, all governments implemented complete or partial lockdowns, quarantines, and social distancing [3456]. In Turkey, schools and universities were closed on March 16th, 2020, after the first officially reported case (March 11th, 2020). Afterwards several confinement measures were introduced to limit the rate of infection, including the closure of hotels, restaurants, places of entertainment, and non-essential industries, as well as the restriction of cultural recreational and sports activities, domestic and international travels, and lockdowns on those under 20 and over 65 yrs of age. These restrictions started to resume a normal status on June 1st, 2020. After an increase in the number of COVID-19 cases, all restrictions started again in October 2020. The government promoted distance-working in all sectors. Partial lockdowns were introduced on those under 20 and over 65 yrs of age at different hours during the day. Complete lockdowns were implemented throughout the country on weekends, and between 9 pm and 5 am on weekdays for all age groups. Recently, since March 2021, the Turkish government has begun to implement different restrictions, which are tightened according to the number of COVID-19 cases in each city. The Turkish population had to live under these confinement measures in order to control the spread of the disease. During this time, however, only healthcare workers were vaccinated, and people over the age of 75 began to receive vaccines.
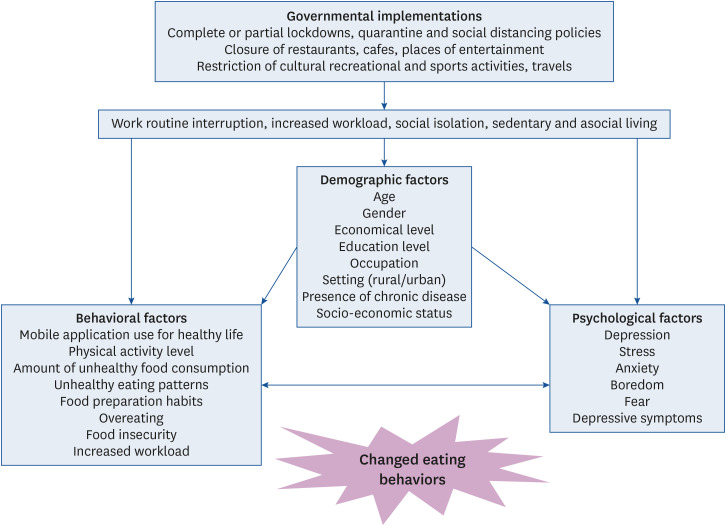
Unfortunately, these confinement measures caused the occurrence of many long-lasting psychosocial impacts, increased the risk of long-term sedentary behaviors, and negatively changed health behaviors, such as physical activity, exercise, and eating habits [789]. The shut-down of gyms, lockdown, working at home, and fear of going out changed the physical activity and exercise habits of people in Turkey. However, some people preferred to exercise at home with self-managed weight loss programs, such as online exercise classes and exercise applications [10]. Moreover, some people had less stress, and more time to focus on healthy eating and exercise [111213]. At the same time, some studies have shown several negative psychological effects of work routine interruption and social isolation, such as higher levels of anxiety, boredom, fear, stress, and depressive symptoms [141516]. The quarantine aroused mood changes like anxiety and boredom, which are considered as major reasons for poor quality food consumption when compared to standard living conditions [1718]. In order to cope with anxiety and boredom-related stress, people show a tendency to overeat “comfort foods” that are rich in fats, sugars, and thus calories, causing serotonin production and stress reduction [1920]. All of these negatively changed health behaviors could lead to weight gain that increases the risk of obesity [21]. The conceptional framework of factors affecting weight change during the pandemic is given in Fig. 1.
Many studies have shown that there is a strong correlation between the prevalence of obesity and increased risk of chronic diseases, such as cardiovascular diseases, type 2 diabetes, and some cancer types [2223242526]. Furthermore, obesity enhances chronic inflammation, which is a major risk factor for serious complications of COVID-19 and impairs the viral defense system [27].
Many studies conducted in different countries, including Spain [9], Italy [28], Poland [5], Iran [3], United States of America [2729], Belgium [30], Croatia [7], Portugal [6], Morocco [31], Lithuania [8], United Arab Emirates [32], China [33], United Kingdom [34], and India [35] have demonstrated that the quarantine has caused weight gain in different population groups, at a rate ranging from 22–98.05%. Furthermore, an increased tendency toward unhealthy eating patterns and reduced physical activity were the main outcomes of these studies. Ammar et al. [4] reported an increase in the consumption of unhealthy foods, number of meals, eating out of control, and more snacking between meals as a result of an international multicultural Effects of home Confinement on multiple Lifestyle Behaviors during the COVID-19 outbreak (ECLB-COVID-19) online survey. Unhealthy eating practices caused weight gain among 31.5% of the Lithuanian respondents [8]. Similarly, an increase in weight gain in young American adults due to the overeating of unhealthy foods in order to cope with pandemic-related stress was reported [29]. These studies demonstrated that the tendency of eating behaviors toward unhealthy lifestyles resulted in weight gain in different population groups in various populations.
Some studies have been conducted in Turkey to determine weight changes during COVID-19 pandemic and the results were reported as either decreased or increased [1113363738]. To our knowledge, no studies have quantified weight changes among adults who experienced the quarantine in Turkey. This study aimed to determine the weight change trend among the adult Turkish population after 1 yr of COVID-19 confinement and factors associated with weight variation.
Go to : 
MATERIALS AND METHODS
Sample and data collection
An online cross-sectional study was conducted between 26 February and 6 March 2021 using an online questionnaire that was created through Google Forms. The target population consisted of Turkish people who were between 19 and 65 yrs of age, living in Turkey during the confinement. Pregnancy, breastfeeding, a diagnosis of cancer, living abroad, and questionnaires belong to respondents who were under 19 and over 65 yrs of age were the exclusion criteria of the study.
In the online questionnaire system, participants were prevented from passing on to the next question unless they answered the question before it. Some questions were not multiple choices, like height and weight, and the participants had to type the values. However, some participants made typing errors and wrote values like 15.5 cm, 9e.4 kg. Moreover, some participants wrote “?” to the question of stress level. All of these (unanswered questions or with typing errors) were accepted as uncompleted questionnaires, were excluded from the data file, and were not evaluated.
The participants were informed about the objectives of the research, and as a condition of participation in the study, it was stated that those who volunteered for the study should weighed themselves up to 1–2 weeks before the pandemic and remembered their weight.
Digital informed consent was obtained from participants who confirmed that were willing to participate voluntarily prior to filling in the online questionnaire. The study was conducted in full accordance with the principles of the Declaration of Helsinki, and all data were collected anonymously and recorded according to the Turkish Law of Personal Data Protection 6698/2016. The study protocol was approved by the Research Ethics Committee of the University of Health Sciences on 19 February 2020 under registration number 21/191.
In order to reach the greatest number of participants, the questionnaire was uploaded and shared on an online platform. A link to the electronic questionnaire was distributed by the authors through social media tools, such as Instagram and Facebook. In addition, the questionnaire was distributed via messaging apps like WhatsApp, and the participants were requested to send it to one another. Finally, an advertisement was posted in the events and announcements section of a website for 5 days.
Research instrument
The questionnaire was composed of 37 questions and divided into 3 sections. The first section was about sociodemographic variables, such as gender, age, education level, income level, employment status, residence, marital status, and professional situation. In addition, height (m) and weight (kg) measurements were taken in order to calculate body mass index (BMI). The participants were asked four questions to determine their weight information. The questions were as follows: “Were you weighed before the pandemic declaration (last 1–2 weeks), and do you remember your weight? “If yes, please write your weight in the previous question? “Did you weigh yourself in the last 1–2 weeks, or can you be weighed today?” and “If yes, please write your weight? BMI values (before the pandemic and the first year after the pandemic) were classified in accordance with the WHO (< 18.50 kg/m2 underweight; 18.50–24.99 kg/m2 normal weight; 25.00–29.99 kg/m2 overweight; ≥ 30.00 kg/m2 obese). In addition, the percent of change in the BMI was calculated using the formula [(BMI after 1 yr of pandemic − BMI before pandemic)/(BMI before pandemic)] × 100.
The second section was composed of several questions that were prepared by the authors related to eating habits and physical activity level. Additionally, the stress level was determined using the visual analogue scale (VAS). To determine the participants' stress levels, the following question was asked: "Please score your stress level throughout the pandemic period between 1 (lowest) and 10 (highest)".
In the third section, in order to determine the eating behaviors of the participants the Three-Factor Eating Questionnaire-R18 (TFEQ-R18), consisting of 18 questions, was used [39]. Turkish validity and reliability analyses were conducted [40]. This scale was used to assess the degree of cognitive restraint (conscious restriction of food intake to control body weight or promote body weight loss), uncontrolled eating (loss of control of excess food intake and tendency to eat more than normal accompanied by subjective feelings of hunger), and emotional eating (inability to resist emotional symptoms) of the participants. The cognitive restraint subscale contains 6 items that are thought to measure an individual's tendency to restrict dietary intake to control weight. The uncontrolled eating subscale includes 9 items that are thought to measure an individual's control over their eating behavior. The emotional eating subscale includes 3 items that are thought to measure an individual's emotional eating their eating behavior.
The scale is a 4-point Likert type scale (definitely true/mostly true/mostly false/definitely false). Each question ranges from 1 to 4 points. The total score obtained from the sub-dimensions of the scale is as follows: cognitive restriction 6–24, uncontrolled eating 9–36, and emotional eating 3–12. Increasing scores on the scale indicate increased symptoms. The raw scores determined according to the answers given to the questionnaire were converted into 0–100 points in order to standardize the unequal question distribution. The raw scale scores were transformed to a 0–100 scale [(raw score lowest possible raw score)/(possible raw score range) × 100] [3941]. So, TFEQ-R18 score values were converted to percentage (%) values to be used for the standard assessment.
Statistical analysis
Frequencies and percentages were used to express the categorical variables, while the mean, SD, median, and interquartile range were used to express the continuous variables. Hierarchical regression was conducted to clarify the factors associated with weight change. While the categorical variables were included in the model, dummy variable coding was also done. All of the variables that were thought to have a relation with BMI (weight) change (sex, age, education status, marital status, occupation status; income status; chronic disease status; BMI categories; the amount of food consumed when compared to before the pandemic; increase in the consumption of ready snacks; increased prepared pastries, etc., at home; the presence of a child under the age of 15 at home; physical activity when compared to pre-pandemic; emotional eating score %; uncontrolled eating score %; cognitive restraint score %; level of stress) were included in the multiple linear regression model. With the backward elimination method, the variables that contributed the least to the model were removed from the model, respectively, and the final model was obtained. In the backward elimination method, beginning from the first model, the variable with the highest value that had a cut-off value above P > 0.10 was removed, and step-by-step, the same method was applied in each new formed model. The model was stopped when the P-value of all the variables in the model was below 0.10. The 11th model was the final model. The removed variables from the first model to the final model were as follows: marital status (married); income status (insufficient, reference value = no income); education status (high school, reference value = primary and secondary school); education status (postgraduate, reference value = primary and secondary school); education status (university, reference value = primary and secondary school); occupation status (student, reference value=employed); the presence of a child under the age of 15 at home (yes); occupational status (unemployed and retired, reference value = employed); income status (enough, reference value = no income); increased prepared pastry, etc. at home (yes). The distributions of the residuals (normal/symmetrical distribution and predictive versus residual plots) were examined for the model validity. The R square adjusted R-square and SE values obtained at each step showed very small changes, and the simplest model was preferred according to the parsimony principle. Statistical analysis was performed using IBM SPSS Statistics for Windows 25.0 (IBM Corp., Armonk, NY, USA). Tests for significance were 2-tailed with a significance level of 0.05.
Go to :
RESULTS
Demographic characteristics of the participants
A total of 1,694 individuals participated in the study. Sixty-four individuals, who either were not in the 19–65 age range or provided incomplete information, were excluded from the study. Finally, the study was completed with 1,630 adults in total, who were between the ages of 18–65 yrs including 485 males, and 1,145 females. Most of the participants in the study had a university degree (41.35%). Regarding the occupation status, it was determined that almost half of the participants were employed (45.6%) and 17.18% were unemployed. The participants were asked to evaluate their income level. As a result, approximately one-third of the participants (31.78%) reported that they had no income, whereas 21.78% reported that they had an insufficient income level. Moreover, the rate of participants who had a sufficient income level was less than 50% (46.44%). A vast majority of the participants (82.64%) did not have any chronic diseases. In terms of marital status, it was found that 59.57% of the participants were single. On the other hand, the rate of those who were living with a child under the age of 15 at home was 41.96%. According to the results of the VAS score, measuring the stress level of the participants during COVID-19 pandemic, it was determined that most of the participants (64.05%) experienced severe stress levels, ranging between 7 and 10 points. The rate of normal weight participants based on the BMI (18.50–24.99 kg/m2) was 55.75% before the pandemic period started. Whereas this rate decreased to 51.91% at the end of the first year of pandemic. On the contrary, the rate of obese (BKI ≥ 30.00 kg/m2) participants increased from 10.22% to 13.49% during the same period (Table 1).
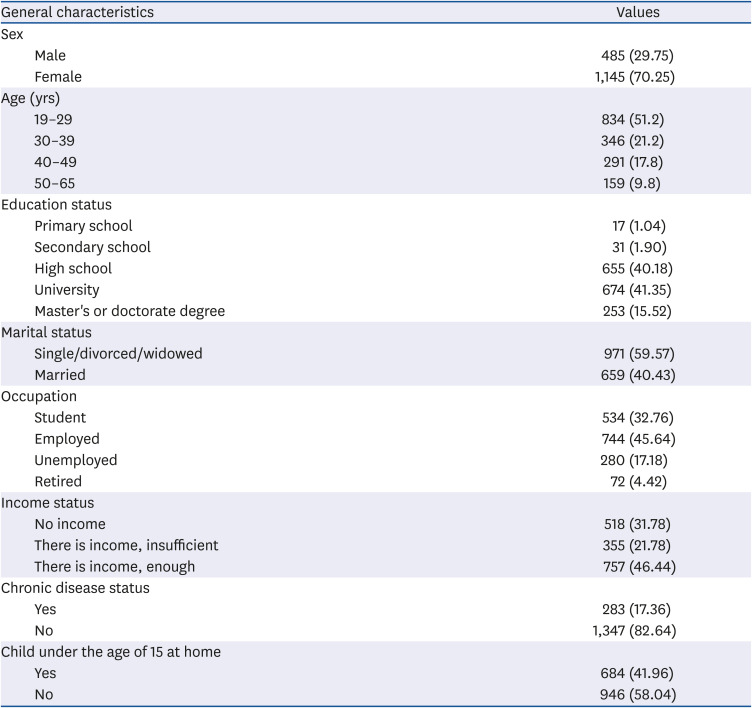
Table 1
General characteristics of individuals (n = 1,630)
![]()
Eating behavior and weight change trend of the participants
Table 2 shows that 30.74% of the participants lost weight and 58.96% gained weight. In addition, the rate of participants who did not change their daily physical activity level was 6.13%, whereas a very high percent of the participants (81.23%) decreased their physical activity level. In terms of the amount of food consumed, approximately one-third of the participants (27.24%) decreased their food consumption and nearly half of them (46.81%) increased it. In accordance with these data, more than half of the participants (54.48%) cooked more pastries, cakes, pates, etc., at home than before the pandemic. Interestingly, 52.58% of those did not increase their consumption of pre-packaged food products during the first year of the pandemic (Table 2).
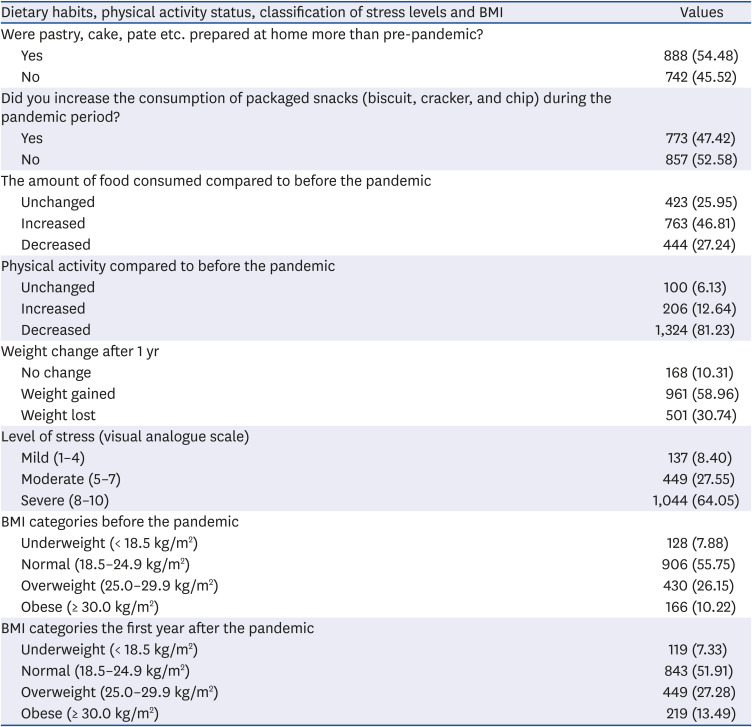
Table 2
Distribution of individuals according to their responses to some dietary habits and physical activities, the stress levels, and the classification of BMI values (n = 1,630)
![]()
While the average weight of the participants was 68.1 (15.70) kg before the pandemic, it was determined that this value increased to 69.22 ± 16.33 kg at the end of the first year of the pandemic. An average weight of 1.15 ± 6.10 kg was gained (females: 0.72 ± 5.51; males: 2.16 ± 7.22). Furthermore, 75% of the participants had a BMI of ≤ 26.67 kg/m2 before the pandemic, and this value increased to 27.46 kg/m2 at the end of the first year of the pandemic. The minimum–maximum weight values before and at the end of the first year of pandemic were 35.0–165.0 kg and 37.0–150.0 kg, respectively. Moreover, an average increase of 0.40 ± 2.14 kg/m2 was determined in the BMI. It was determined that the average stress level of the participants was 6.96 ± 2.22, and 25% of the participants had a stress level below 6 points, while 75% had a level below 8 points. According to the TFEQ-R18 scale, which aims to determine eating behaviors, the uncontrolled eating score of the participants was 39.92 ± 22.31, the average emotional eating score was 43.97 ± 30.80, and the average cognitive eating score was 51.06 ± 20.14 points out of 100 points (Table 3).
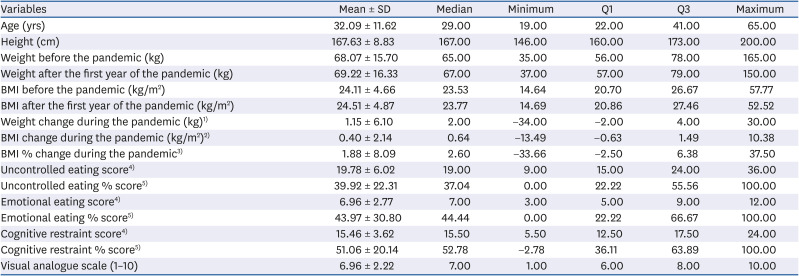
Table 3
Mean and quartile values of age, anthropometric measures, stress levels, and TFEQ-R18 scores of participants
Values are presented as mean ± SD.
TFEQ-R18, Three-Factor Eating Questionnaire-R18; Q1, percentile 25; Q3, percentile 75; BMI, body mass index.1)Formula (weight after the first year of the pandemic − weight before the pandemic).
2)Formula (BMI after the first year of the pandemic − BMI change during the pandemic).
3)Formula [(after BMI − before BMI)/before BMI] × 100.
4)TFEQ-R18.
5)Formula The raw scale scores are transformed to a 0–100 scale [(raw score lowest possible raw score)/(possible raw score range) × 100].
![]()
Factors associated with the BMI (weight) change of the participants
Hierarchical regression analysis was performed in order to explain the proportional (in percentage) change in the BMI following the pandemic. All variables that were thought to have a relation with the BMI (weight) change were included in the multiple linear regression model. With the backward elimination method, the variables that contributed the least to the model were removed from the model, respectively, and the final model was obtained. The variables showing significant association are shown in Table 4. According to the obtained final model, the change in the BMI for the women was on average 2.32% lower than that of the men. The change in the BMI was circa 1.12% higher in those with chronic diseases when compared to those who did not have any, and it was circa 0.79% higher in those who increased their consumption of biscuits, crackers, and chips, etc., when compared to the normal group, the change in the BMI was 1.71% higher in the underweight group, whereas it was 2.29% and 4.96% lower in the overweight and obese groups, respectively, before the pandemic. The change in the BMI was associated with the level of food consumption. The BMI was 2.04% lower in the group in which decreased food consumption was observed and 3.77% higher in the group in which increased food consumption was observed. In addition to the change in the BMI was inversely correlated with physical activity. The BMI was 1.66% lower and 2.29% higher in the groups in which physical activity increased and decreased, respectively, when compared to those with no change in physical activity during the pandemic. The average change in the BMI for each 1-yr age difference was 0.11% higher in the older individuals than in the younger individuals. A one unit increase in the stress level was found to be associated with a 0.14% decrease in the change in the BMI. Each 1% increase in the uncontrolled eating score and emotional eating score resulted in a 0.02% and 0.03% increase in the BMI, respectively. On the other hand, a 1% increase in the cognitive restraint score decreased the BMI by 0.05%.
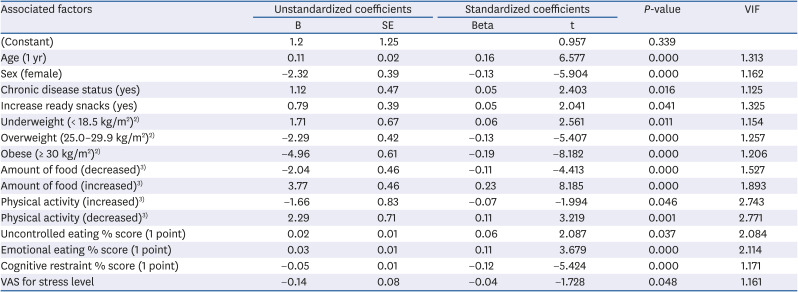
Table 4
Factors associated with 1% change in body mass index1)
Values are presented as below: R-sqr = 0.314, Adj.R-Sqr = 0.307, SE = 6.73, F = 49.169, P < 0.001.
VIF, variance inflation factor; VAS, visual analogue scale.
1)multiple linear regression (backward elimination technique).
2)Reference value = normal (18.5–24.9 kg/m2).
3)Reference value = unchanged.
![]()
Go to :
DISCUSSION
During the COVID-19 pandemic, governments have applied travel restrictions, self-quarantine implementations, and stay-home orders, as well as compulsory social distance practices in public areas to prevent the spread of the virus. It was reported that all of these precautions have caused significant changes in lifestyle and mental health [4243]. Additionally, concerns regarding the important long-term impacts of lifestyle changes on weight management have emerged. Many studies were conducted at the beginning of the quarantine period to evaluate the impacts of the pandemic on body weight and eating habits [2744]. These studies, which covered a relatively short period of the pandemic, stated that small changes in body weight may become permanent, and result in significant weight gain over time [454647]. In 2 studies in Turkey that were conducted at the beginning of the pandemic, it was observed that the rate of participants who stated that their body weight increased (35.0%; 38.4%) and did not change (36.0%; 48.6%) was higher than those who stated that they lost weight [3848]. In the present study, which was planned to determine the long-term effects of the pandemic, it was found that 58.96% of the participants gained weight, and 30.74% lost weight at the end of 1 yr of the pandemic. Thus, the number of overweight and obese people increased, while the number of those who were underweight and normal weight people decreased when compared to their initial body weight according to the BMI classification. Older age, being male, the presence of chronic disease, an increase in uncontrolled eating scores, and an increase in emotional eating scores were found to be important factors causing an increase in the BMI, whereas a reduction in food consumption, increase in physical activity, higher stress level, and an increased cognitive restraint score were the factors associated with a decrease in the BMI.
It was announced that the first COVID-19 case was seen in Turkey on the same day as the declaration of the pandemic in the world. During this 1-yr period, from March 11 to June 1, a nationwide quarantine was implemented, between June and September, the application of various restrictions and preventive measures continued, and in October, a full quarantine on the weekends and weekday evenings continued until the first year. The pandemic resulted in mandatory lockdowns, affected daily work routines [3638], increased responsibilities [13], and changed physical activity levels [11] drastically. These sudden changes affected the mental health of individuals, and caused some positive, as well as many negative, changes in their eating habits. It was reported that many adverse psychological effects were observed in people after isolation, including post-traumatic stress disorder, confusion, and anger [1449]. It is believed that increased stress and boredom play an important role in weight gain through sleep disorders, increased energy intake, and decreased exercise levels [5051]. Studies have shown that in cases of intense stress, people typically tend to eat more in response, to better cope with the situation, and they tend to consume unhealthy, high energy-dense foods, such as chocolate, chips, appetizers, and fast food [525354]. In this study, the BMI value was approximately 0.79% higher in people who consumed more chips, chocolate, and biscuits when compared to those who did not. The studies about the pandemic have shown that people have been driven to consume foods with a high sugar content, which are defined as comfort foods, more often than usual [455]. In the current study, it was found that the majority of the participants increased their consumption of food and baked more cakes and pastries at home, supporting these findings. This type of diet increases the risk of type 2 diabetes and obesity. It was shown that individuals with type 2 diabetes and obesity are at high risk in terms of serious complications and mortality caused by COVID-19 [56].
Although 1 yr has passed since pandemic began, 64.05% of the participants reported that they are still under high stress. Many factors, such as the economic crisis, lack of income, death of relatives, getting fired/laid off from their jobs, the long periods spent at home, fear of virus, boredom, and uncertainty, may boost the stress level in people. Additionally, considering that 70.25% of the participants in this study were females, other factors causing the increased stress levels of the women could be distance learning of children at home, staying at home for long periods due to distance working or flexible working hours, and meeting the care needs of family members. The perception and evaluation of stress vary among people due to differences in external or internal stimulus, personalities, emotional condition, and physiologic reactions [57]. For example, 40% of people increase calorie intake, 40% decrease calorie intake, and 20% do not change the intake when they are stressed [5859]. In the current study, it was determined that the high levels of stress were associated with a decrease in the BMI. In another study, it was found that the level of stimulation affected food intake, a very high level of stress was associated with eating less, and a lower level of stress was associated with overeating [60]. The average stress level in this study was 6.96 ± 2.22. Unfortunately, the pandemic is still not under control. Moreover, the very slow vaccination progress, economic factors, and future anxiety may be the reasons for why people still experience high stress. Prolonged exposure to stress can lead to a decrease in food intake. Additionally, the emotional conditions or characteristics of individuals may affect their eating habits.
Emotional eating is an eating behavior that is assumed to occur as a response to emotional state only, not due to hunger or because it is meal time nor due to a social necessity [54]. This eating behavior is a way to avoid or distract oneself from uncomfortable and negative emotional states. People who are in a negative mood and overeat, tend to eat delicious high-energy foods with a high sugar content. All of these can lead to weight gain [616263]. As a matter of fact, in this study, it was found that a 1% increase in the uncontrolled eating and emotional eating score caused an increase in the BMI. Furthermore, a 1% increase in the cognitive restriction score resulted in a decrease in the BMI. Restricted eating is a cognitive control effort to voluntarily restrict food intake in order to achieve or maintain weight loss. Cognitive restriction is associated with food intake under stress. People who consume severely restricted food, increase their food intake in a stressful situation, and those who eat uncontrolled food reduce their food intake [64]. Given that excess food intake and uncontrolled eating are more common in obese people [65], the intense stress experienced during the pandemic may have caused food restriction. Additionally, the declaration of obesity as a high-risk factor in COVID-19 mortality may have increased the avoidance of food consumption. This can explain the cause of greater weight loss observed in obese people.
Two studies have demonstrated that women were more affected by COVID-19, resulting in increased emotional eating habits, thus increased weight gain [3866]. However, this study found that during the 1-yr pandemic, the BMI changed less in women than in men. Although the long duration of the pandemic caused some negative situations, it resulted in an increase, especially in women's awareness of weight gain anxiety in a positive manner. Due to the fact that men spend more time outside or work outside may have affected their energy use more in this new situation. Herein, it was believed that women adapted to and managed the new conditions better. In addition, in this study, it was determined that the most important independent variable explaining the change in the BMI was the increase in the amount of food consumed. Due to the fact that men spend more time at home, contrary to their habits, may have increased the total amount of food eaten daily.
Unlike previous studies where overweight and obese people were more likely to gain weight [286768], the present study gained a different striking result. The change in the BMI was 2.29% and 4.96% lower in the overweight and obese groups than in the normal group, respectively. Additionally, the change in the BMI in the underweight group before the pandemic was approximately 1.71% higher than in the normal group. In other words, it was determined that those who were overweight and obese lost weight at the end of the first year of the pandemic, while those who were underweight gained weight. Despite the results of most studies, this finding was in accordance with the results of a study conducted in China at the beginning of the pandemic [44]. It is thought that these restrictions affected overweight and obese individuals less than others due to the more sedentary and asocial living style of obese people. In other words, the pandemic period may not have caused a drastic change in their weight. The weight gain of underweight and normal people can be attributed to the fact that they consumed more food and exercise less during the quarantine. This result showed that the prevalence of post-pandemic overweight or obesity may increase.
Although the weight loss in overweight and obese people seems to be gratifying, overall, 1.15 ± 6.10 kg were gained (min: −34 kg, max: 30 kg) throughout the study. This average value seemed to be insignificant, but it should be considered that 30 kg of weight were gained. In particular, decreased physical activity levels in the vast majority of participants (81.23%) could be considered as an important factor in weight gain. Common findings of studies conducted during the pandemic on weight gain included sleeping disorders, overeating, decreased physical activity, increased overall food consumption, and increased consumption of sugary and sweet foods in response to stress [274469]. In this study, the increase in snack consumption was found to be associated with a 1% change in the BMI.
Considering that obesity is one of the main risk factors for respiratory failure leading to invasive mechanical ventilation in the United States, which is 10 times higher than in China, and the decreased respiratory capacity of obese patients as a risk for COVID-19 complications, it is quite clear that taking preventive actions against weight gain and obesity is crucially important [70]. Frequent or daily weighing is an effective method to lose weight and maintain it, as well as to prevent age-related weight gain [71]. Alternatively, more typical strategies to maintain weight during this challenging period may include the limitation of high energy-dense foods with low nutritional value; cooking more often at home rather than eating ready-to-eat and packaged meals; doing effective physical activities; planning self-managed exercise sessions from home; creating daily routines; doing relaxing activities such as meditation, yoga, which may decrease stress levels [50].
As a result, this study provided information that the weight trend was on the rise in the first year of the quarantine and social isolation process experienced due to the emergence and fast spread of a new type of coronavirus in Turkey. At the end of 1 yr, the proportion of those who were overweight and obese increased when compared to before the pandemic. Age, being male, the presence of a chronic disease, uncontrolled eating, emotional eating, increase in food consumption, decrease in physical activity and stress level, and an increase in the consumption of ready snacks were found to be significantly associated with an increase in the BMI. However, independent variables, such as educational status, economic status, marital status, and the presence of a child at home, were not significantly associated with the change in the BMI. Moreover, a high level of stress still exists in Turkey 1 yr after the pandemic began.
One of the limitations of this study was that all of the data were based on personal statements, particularly the necessity to remember one's weight before the pandemic, because the weight based on the study participant's recall might differ from their actual weight. Additionally, the participants might have felt that they gained more weight due to limited physical activity. Moreover, as this study only included those who remembered their weight, it can be concluded that the study was limited to people who were more concerned about their health. On the other hand, this study was performed online by participants that had access to the Internet and equipment such as computers and tablets. In Turkey, this equipment is closely related both to education and economic status. As a result of this situation, the number of undergraduate and graduate participants constituted more than half of the participants in the study. Participation by people who were illiterate or primary school graduates was limited. Furthermore, the BMI values differed from the other studies conducted throughout Turkey. When compared to the nationwide General Nutrition and Health Survey data, the BMI values in the pre-pandemic period of the participants in this study were lower [72]. Finally, the backward elimination method based on beta-coefficients was used in this study. The variables that were removed from the model, step-by-step, were the highest values according to the cutoff score; however, this method may have caused conceptually important variables to be eliminated by chance.
This pandemic situation has highlighted the strengths and weaknesses of governments in response to such sudden health crises. As the future is unpredictable, long-term action plans together with short- and medium-term action plans should be planned to work together with the public, society, and healthcare professionals to reduce the risks to the minimum level. COVID-19 could result in persistent effects on various organs even though the patients recovered from this disease. The examination of the long-lasting effects of COVID-19 would be a critical step for future generations. Quarantine and isolation may increase psychosocial distress. Promoting health through the management of energy, sleep, and mental health would help to maintain the psychological well-being of people. The dissemination of science-based information, evidence-based recommendations, and correct guidance to the public and policymakers through different tools could be an effective way to combat the pandemic. The socioeconomic or health dimensions of the pandemic can increase the anxiety, stress, and fear levels of society. The negative effects of these factors on eating behavior, eating habits, and obesity are well-known, and the government should take measures to reduce these negative effects on society. The public should be guided with regard to adapting to pandemic conditions through the social media accounts of the Ministry of Health, television programs lead by experts, and family physicians. Publications and programs can be prepared that would increase the awareness of the public about the importance of weight, obesity control, and healthy nutrition through television and social media. A free healthy nutrition and obesity hotline can be established where the public can get advice. When there are no confinement measures, free activities can be organized by professional trainers in open areas or parks to encourage physical activity.
Go to :
 XML Download
XML Download