

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
On March 12, 2020, the World Health Organization (WHO) declared the Coronavirus disease 2019 (COVID-19) a pandemic [1]. Globally, countries such as the United States, Italy, the United Kingdom, and Spain have implemented drastic strategies, such as social distancing, smart working, school closures, quarantine, and travel restrictions [23]. The Saudi Arabian government has also enforced quarantine to suppress the spread of COVID-19. Quarantine and social distancing have helped reduce the transmission of COVID-19. However, quarantine is a new experience for the younger generation, especially children, as it encroaches upon their freedom, possibly causing stress and depression [4]. The COVID-19 pandemic curfew has affected the lifestyle of children, especially their diet and physical activity. More than 85% of the families in Italy and Spain have reported changes in children's emotions and behaviors during quarantine [2], leading to an unhealthy diet and reduced physical activity level [4]. Changes in lifestyle can result from reduced availability of goods due to restricted store opening hours or feeling of stress, which leads to an increased intake of food, especially food containing high quantities of sugars and fats, as these food items have positive effects on the mood due to the glycemic index level [5]. Di Renzo et al. [6] indicated changes in hunger and satiety sensation in more than half of the population during quarantine, with an increased appetite in approximately 34% of the participants.
Changes in lifestyle and insufficient physical activity due to prohibitions on outdoor exercise during COVID-19 has increased body weight and/or fat deposition among children, and therefore, increased the incidence of being obese in the future [378]. Childhood obesity has been considered a pandemic, putting children and adolescents at risk of poor health [9]. Moreover, it is considered as the fifth leading cause of death in adults, with around 4 million deaths in 2017 according to WHO. In Saudi Arabia, a study by El Mouzan et al. [10] found that, in children aged 5–18 years, the overall prevalence of overweight, obesity, and severe obesity were 23.1%, 9.3%, and 2%, respectively. Obesity during the quarantine could worsen, as people with body mass index (BMI) >25 can undergo over-eating and thus further gain weight [5]. Additionally, childhood obesity is associated with a significantly increased weight in adulthood [11].
There is a positive relationship between obesity and cardiovascular disease (CVD), diabetes, and other chronic diseases [1213]. Therefore, the consumption of healthy diet and physical activity must be promoted during quarantine.
This study aimed to highlight the effect of COVID-19 on children's health behaviors during curfew, including eating habits, physical activity, and sedentary behavior.
Go to : 
SUBJECTS AND METHODS
Participants
This survey was conducted between June 22 and July 22, 2020. The target population was children aged 6–15 years from all different regions across the Kingdom of Saudi Arabia. For families with more than one child between ages 6–15, the parents were asked to fill out one survey form separately for each child. This study included children in both genders attending primary and intermediate schools, and excluded children below 6 years and those above 15 years of age.
Based on a statistical power of 80%, confidence level of 90%, margin of error of 5%, and a population size of around 6 million children aged 6–15 years, a minimum sample size of about 271 participants was required.
Approval for this study was obtained from The Faculty of Medicine Research Ethics Committee at King Abdul-Aziz University (reference No. 380-20).
Study design
This cross-sectional study was conducted using online survey distributed via social media (WhatsApp, Twitter, and Snapchat) in Arabic language. The first page of the survey included digital consent form, objectives of the study, duration of the survey, voluntary declaration, confidentiality, and anonymity of the study. The survey included 43 questions divided into 3 sections: demographic characteristics, anthropometric measures, and health behaviors, including eating habit, physical activity, and sedentary behavior before and during COVID-19.
Sociodemographic characteristics
Sociodemographic characteristics included gender, age, region of residence, parents’ education, occupation and condition, accommodation type, diagnosis of any chronic conditions that affect eating habits, and whether the children take any supplements.
Anthropometric measures
Due to the COVID-19 curfew situation, the height and weight of children were self-reported by the parents. Parents were asked to measure their children's height and weight with the children's shoes off and their light clothes on. BMI and BMI percentiles (ile) were calculated using weight in kilograms, height in meters, date of birth and gender, based on the Excel spreadsheet provided by the Center for Disease Control and Prevention.
Children were classified into 4 groups based to their BMI: BMI <5th ile, underweight; 5th to < 85th ile, normal weight; 85th to < 95th ile, overweight; and ≥ 95th ile, obese.
Changes in health behavior
Parents were asked if their children's eating habits changed 4 months later after the WHO declared COVID-19 a pandemic, compared with their eating habits before the pandemic. If the parents replied “yes,” they were asked to mention the ways in which the eating habits had changed: whether healthier/unhealthier.
Further, parents were asked what their children tend to do when they feel bored during the curfew (choose all that apply): eat more/sleep more/watch TV/more use of computer/video games/exercise. Additionally, parents were asked about the number of meals, and the days in which breakfast was consumed by their child before and during the curfew. We also asked about the frequency of consumption of the following foods before and during the curfew: vegetables, fruits, milk and dairy products, soft drinks, sugar-sweetened beverages, sweets/candy/chips, and fast food. These questions were adopted from the Health Behavior in School-Aged Children (HBSC) study [14], and were slightly modified. All questions included 5 response options ranging from “None at all” to “5–6 times a week.” However, question regarding soft drinks and sugar-sweetened beverages included eight response options ranged from “≤ 1 Can a month” to “≥ 3 Cans a day.” The response options were recorded dichotomously as: 1) daily, “≥ 1 per day”; 2) not daily, “< 1 per day.” For soft drink and sugar sweetened beverages, it was recorded as: 1) often, “≥ 1 per day”; 2) not often, “< 1 per day.”
For physical activity and sedentary behavior, parents were asked whether their children’s physical activity levels had increased/ decreased/ remained unchanged during the curfew compared with that before curfew. Moreover, parents were asked about the number of days during a week their children participated in physical activities before and during the curfew. The question included 5 response options that ranged from “None at all” to “5–6 times a week.” The responses options were recorded based on the HBSC study as: ≤ 4 times a week, “not physically active;” and ≥ 5 times a week, “physically active.”
Furthermore, parents were asked about the number of hours children spent watching TV/computer/video games per day before and during the curfew. These questions included 9 response options ranged from “None at all” to “≥ 7 h a day.” The response options were recorded based on the HBSC study as: ≥ 4 h of watching TV per day was considered high level of watching TV, while ≥ 3 h of computer use was considered high level of computer use.
Data analysis
Descriptive analysis is presented as mean ± SD for frequency, and as percentages. The χ2 test was applied to compare between categorical variables. McNemar test was used to measure significant differences in categorical data before and during the curfew. Repeated measures analysis of variance (ANOVA) was used to determine differences between continuous variables before and during the curfew. A P-value < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS program version 23 (SPSS, Inc, Chicago, IL, USA).
Go to :
RESULTS
Participants' characteristics
In total, 280 participants who completed the survey were included in the study, after excluding those with incomplete data (n = 12). There was almost an equal distribution of girls (n = 137, 49%) and boys (n = 143, 51%) in the study. The average age of children reported by their parents was 10.22 ± 2.72 years. Majority of the participants were from the Western region (n = 241, 86%). About 72% (n = 202) and 79% (n = 221) of the fathers and mothers, respectively, held a university degree. About 88% (n = 245) of the fathers were working, and 58.6% of the mothers were housewives (n = 164). Most of the participants were living in apartments (n = 171, 61%). Majority of the children had no chronic disease (n = 263, 94%). Only 23% (n = 64) of the participants reported being administered supplements during COVID-19, and of those, only 14% (n = 39) reported regular use. Characteristics of the parents and children are provided in Table 1.
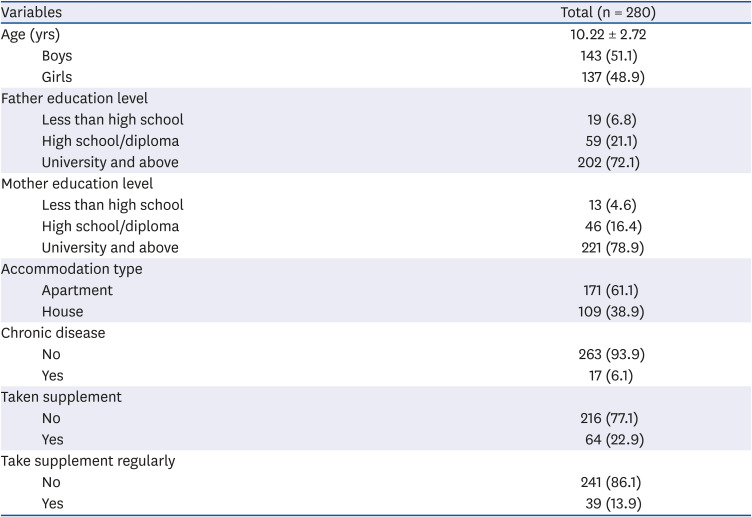
Table 1
Sociodemographic characteristics of participants
![]()
BMI classification
Thirty-four percent of the parents reported no change in the body weight of their children during the COVID-19 curfew, while 53% and 13% thought that their children might have gained or lost weight, respectively. The COVID-19 curfew was significantly associated with increase in the children's BMI. The results showed that the percentage of underweight children decreased from 13.9% to 8.2% during the COVID-19 curfew, while that of obese children increased from 18.9% to 22.5% (P < 0.001; Table 2).

Table 2
BMI classification among children before and during the COVID-19 curfew
| BMI classification (n = 241)1) | Before COVID-19 | During COVID-19 | P-value |
|---|---|---|---|
| Underweight | 39 (13.9) | 23 (8.2) | < 0.001*** |
| Normal | 104 (37.1) | 110 (39.3) | |
| Overweight | 45 (16.1) | 45 (16.1) | |
| Obese | 53 (18.9) | 63 (22.5) |
Values are presented as number (%).
BMI, body mass index; COVID-19, coronavirus disease 2019.
1)1n = 39 participants reported I don't know.
***P < 0.001 was considered statistically significant.
![]()
Eating habits during COVID-19 curfew
With regards to eating habits during the COVID-19 curfew, 27% (n = 75) reported no change in eating habits, while 38% (n = 106) and 35% (n = 99) reported changes in the eating habits or some changes, respectively, in their children. Moreover, 33% (n = 91) and 31% (n = 88) of the parents reported that their children's eating habits had become unhealthy and healthy, respectively.
Children who were classified as overweight/obese significantly tend to follow unhealthy eating habits during COVID-19 curfew (42.6%) compare to children with normal and under body weight (20.9%, 39.1%, respectively) (P < 0.05; Table 3)

Table 3
Association between body mass index classification of children's and eating habits during the COVID-19 curfew
Values are presented as number (%).
1)39 participants reported I don't know.
*P-value < 0.05 was considered statistically significant.
![]()
Parents reported changes in the number of meals their children consumed daily. The repeated measures ANOVA with a Greenhouse-Geisser correction showed that the mean number of meals consumed by the children was significantly different before and after COVID-19 curfew (F [1.00, 279.0] = 84.35, P < 0.001). Post hoc tests using the Bonferroni correction revealed that there was a decrease in the number of meals consumed daily during COVID-19 curfew than that before curfew (2.71 ± 0.520 vs. 2.52 ± 0.568, respectively).
Further, the COVID-19 curfew led to a significant decrease in the consumption of fast food (77%) than that before curfew (96%) (P < 0.001).
We examined the difference in daily food intake before and after COVID-19 curfew, and the analysis suggested no significant difference between daily consumption of vegetables, fruits, sweets/candy/chips, sugar-sweetened beverages, and soft drinks before and during COVID-19 curfew.
Additionally, in the case of daily consumption of dairy food, the COVID-19 curfew led to a significant decrease in the daily consumption (50%) compared with that before the curfew (56%) (P < 0.001).
Finally, the COVID-19 curfew led to a significantly lower intake of breakfast meal (52%) than that before curfew (73%) (P < 0.001).
Table 4 summarizes the changes in eating habits in children before and during COVID-19 curfew.
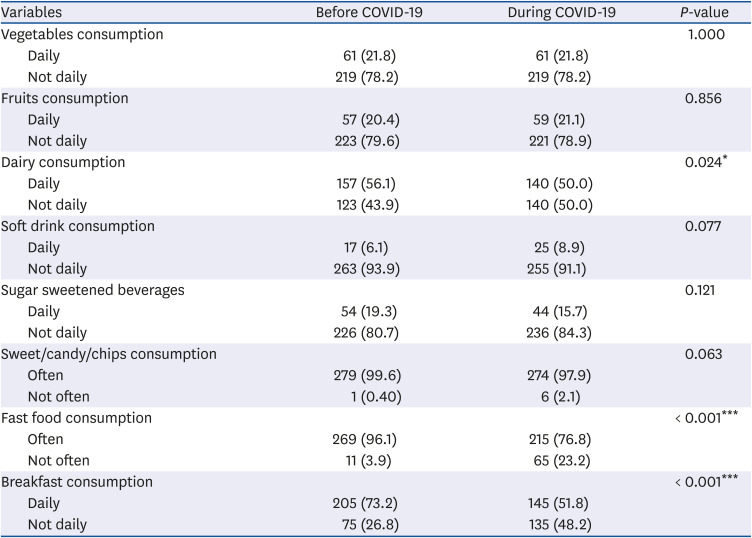
Table 4
Changes in eating habits among children before and during the COVID-19 curfew
Values are presented as number (%).
COVID-19, coronavirus disease 2019.
*P < 0.05, ***P < 0.001 was considered statistically significant.
![]()
Physical activity and sedentary behavior during COVID-19 curfew
With regards to changes in physical activity and sedentary behavior in children during the COVID-19 curfew, 88% (n = 280) of the parents reported that their children watched TV or played video game when they felt bored, while 18% (n = 51) reported that their children practiced physical activities, and 11% (n = 30) reported that their children slept when they felt bored.
Further, 31% (n = 88) of the parents reported no change, while 50% (n = 141) and 18% (n = 51) reported decrease and increase in their children's physical activity, respectively. Physical activity did not significantly change before and during COVID-19 curfew. However, the curfew led to an increase in the number of hours spent watching TV and playing video games per day. About 44% of the parents reported that their children spent 4 h or more time watching TV than 21% before curfew (P < 0.001). Whereas, 75% of the parents reported their children spending 3 h or more time playing video games than 40% before curfew (P < 0.001) (Table 5).
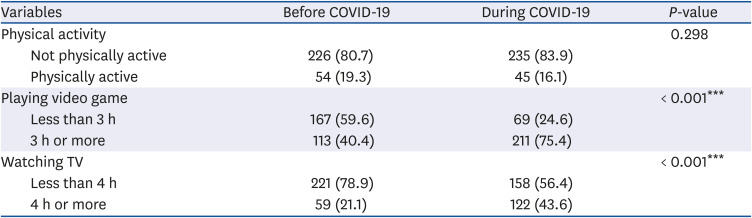
Table 5
Physical activity and sedentary behavior in children before and during the COVID-19 curfew
Values are presented as number (%).
COVID-19, coronavirus disease 2019.
***P < 0.001 was considered statistically significant.
![]()
Go to :
DISCUSSION
To our knowledge, this study was among the first studies to determine the changes in weight, eating habits, physical activity levels, and leisure screen time in children aged 6–15 years in Saudi Arabia before and during COVID-19 curfew. The analysis suggested that the COVID-19 curfew and the subsequent lockdown resulted in a significant difference in the BMI, eating habits, and lifestyle in children before and during COVID-19 curfew. Children significantly tended to skip breakfast and decreased their intake of dairy products and fast foods. Additionally, children were less physically active and significantly tended to perform increased leisure screen-based activities, including watching TV and use of computer/playing games. Our results shed the light on future effects on the health of children due to strict quarantine, showing a significant change in physical activity levels and eating habits.
The changes in eating habits and increase in sedentary lifestyle could explain the perception of significant weight gain reported in children before and after COVID-19 curfew. People who suffer from overweight or even obesity need more care during a pandemic [1516]. Studies have found a strong association between obesity and severe COVID-19 infection, illness, and death [17181920]. Depending on the duration of the curfew, excess body weight gained by the children may not be easily lost if healthy behavior was not adopted, which may contribute to obesity during adulthood [21].
The findings of this study indicated that the COVID-19 pandemic negatively impacted children's eating habits, potentially due to the curfew and increased period required to stay indoors. Alterations in eating habits during COVID-19 curfew can change body weight as a result of decreased levels of physical activity and changes in food intake. Additionally, overweight and obese children tend to show unhealthy eating habits, including overeating and eating when not hungry [22], which may be more pronounced during curfew due to prolonged home stay with unlimited access to food. Therefore, the results are informative on the potential changes of meals prepared and consumed at home.
A previous study has reported an overall high prevalence of unhealthy dietary habits, sedentary lifestyle, and obesity in children in Saudi Arabia [23], and this condition may have worsened during the COVID-19 curfew. The present study showed that during the curfew, children's eating habits have either changed or have some kind of change, and a few parents even assumed that their children's eating pattern has become unhealthier, which may lead to weight gain in children in Saudi Arabia. Similarly, studies conducted in different countries showed an increase in caloric intake and weight gain during COVID-19 and prolonged home stay [6242526]. Therefore, current dietary habits among children in Saudi Arabia may not be effective against the COVID-19 curfew as it can negatively impact the immune system. Therefore, adequate intake of macro- and micro-nutrients are crucial for optimal immune function especially during COVID-19 pandemic [27].
Regarding the number of meals and food consumption, the analysis indicated that the number of meals and consumption of breakfast and dairy products in children had significantly decreased during the COVID-19 compared with that before the pandemic. It appears that children's consumption of dairy products decreased particularly during a pandemic due to the decreased consumption of breakfast, which may be affected by the change in sleeping habits. Previous studies showed that inadequate sleep pattern was associated with unhealthy food habits including decreased breakfast consumption [2829]. Additionally, as indicated by previous studies, majority of the daily milk and dairy products consumed by children was usually during the breakfast [2330]. Breakfast is recognized as the most important meal of the day. A study by Wüenstel et al, [31] has identified the importance of breakfast consumption in maintaining healthy weight status in children and adolescents. Skipping breakfast has become an issue in children. A systematic review found an association between skipping breakfast and increased risk of overweight and obesity in children and adolescents in Saudi Arabia [32]. Cancelling or skipping breakfast, along with consuming sugar-sweetened beverages that contain large amounts of sugars such as sucrose or fructose, eating fast food and fried food, and sitting and watching TV in excess, significantly affected the childhood weight gain and BMI [3334]. Additionally, imbalanced diet might worsen vitamin status, especially vitamin D, which could be affected by reduced outdoor activities.
On the contrary, despite the fact that several parents reported increase in their children's unhealthy eating habits, healthy eating changes were also observed in a significant number of children during the pandemic. Some parents reported that their children consumed less fast food either at home or take-out, possibly because all the restaurants were closed during the curfew.
The results of this study concur with that of a recent study conducted in Canada which indicated that parents and children ate less fast food and take-out during the COVID-19 pandemic [35]. Another study conducted among adolescents from Latin America and Europe found a decrease in fast food consumption during COVID-19 curfew [36]. The decrease in fast food consumption could be due to increased time spent at home and home-cooked meals [35]. Additionally, a study conducted in the US showed that adults tended to cook more and ate out less frequently during the COVID-19 pandemic [37].
The present study indicated that COVID-19 curfew promoted a more sedentary lifestyle, such as watching TV and use of computer/playing games than that before curfew, accompanied by a decrease in physical activity levels. The findings from this study are concurrent with previous studies conducted during the COVID-19 to assess the changes in screen time and physical activity among children, youth, and adolescents, which revealed that the pandemic had negative effect on lifestyle behaviors including decreased physical activity levels and increased sedentary behavior [353839]. Moreover, a systematic review confirmed a strong association of extensive screen time with increased obesity, less consumption of healthy diets, symptoms of depression, and poor quality of life [40]. It is known that schools promote an active routine, including physical activities; however, school closure during COVID-19 pandemic prevented these activities, and hence led to the difference in children's behavior [4142]. Additionally, a previous study comparing eating habits and physical activity before and after vacations showed that children tended to engage in structured activities during the school period, while they tended to not participate in any sports activities and spent time playing video games or using computer during holidays [43]. It is evident that school environments provide children with normal routine about mealtimes, physical activity and sleep time, which are major factors associated with obesity risk [44]. Prolonged sedentary behavior along with unhealthy eating habits may not only lead to weight gain, but also could increase the risk of obesity and developing chronic diseases such as diabetes, and CVD in children later in life [12].
Thus, in this critical period of the pandemic, as the virus continues to spread, healthy dietary habits are imperative than before to help all family members, especially the children, to enhance their body's immunity. It is really important to increase awareness about the importance of positive health-promoting behaviors including healthy eating habits and regular physical activity performance. The WHO has recommended managing stress and health during the pandemic by consuming a healthy and balanced diet, staying active and hydrated, and getting sufficient sleep [11]. However, the findings of the present study were in contrast to the WHO's recommendations. Therefore, it is recommended that parents should make sure that their children consume healthy breakfast daily and are physically active, as these are the most preventive factors against weight gain in children and adolescents. Moreover, parents should involve their children in planning and preparing meals to help them develop important skills and adopt healthy eating habits [4546]. Additionally, parents should ensure that their children's diet contains essential nutrients, such as vitamins D and E, zinc, omega-3, polyunsaturated fatty acids (PUFAs), minerals, and antioxidants [47]. Vitamin D can improve the immune functions, and its deficiency is prevalent in obese people (40–80%), even in sunny regions [47]. Furthermore, zinc maintains homeostasis of the immune system, and omega-3 and PUFAs have strong anti-inflammatory effects [4748].
This is one of the first studies to assess the impact of COVID-19 curfew on eating habits, physical activity levels, and leisure screen time in children in Saudi Arabia, although it has few limitations. First, due to the cross-sectional nature of the study design, we could not determine the causal association; however, it was a suitable design during the COVID-19 curfew. Second, the sample size was limiting and may not be representative of the entire population. The study parameters were self-reported by the parents, including children's weight and height, which may result in response bias and/or underestimate/overestimate their responses. In addition, the health behavior questions were self-reported and asked before and during COVID-19, which may result in recall bias.
In conclusion, the study indicated a negative impact of the COVID-19 curfew on the eating habits and physical activity levels, with a significant increase in screen time and unhealthy eating habits, indicative of breakfast skipping and a decreased consumption of dairy products. As the COVID-19 pandemic continues, it may have a long-term impact on the eating habits, physical activity level, and sedentary time, while negatively affecting the children's physical and mental health. Therefore, future research should be conducted to assess the long-term impact of the COVID-19 pandemic on children's eating habits and physical activities. An understanding of the eating habits and lifestyle of children during the COVID-19 curfew will help in the implementation of more effective health interventions and reform future recommendations about physical activity and nutrition.
Go to :
 XML Download
XML Download