

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sleep is one of the basic physiological human needs with importance comparable to drinking water, eating, or breathing, according to Maslow's hierarchy of needs [1]. Sleep status is associated with overall health; thus, it is recommended that adults aged 18−65 yrs sleep 7−9 h per night, as shorter nighttime sleep duration has been associated with obesity, alcohol use/abuse, nicotine use, psychiatric disorders, inflammation, cardiovascular disease (CVD), and deficits in cognitive functions [234].
According to the Korea National Health and Nutrition Examination Survey, only half of Korean adults sleep 7−8 h per night [5]. Insomnia characterized by difficulties with falling asleep, maintaining sleep, and early morning awakening for at least 3 mon, is one of the most common sleep disorders and often treated with cognitive behavioral treatments, nondrug alternatives, or the use of benzodiazepines, benzodiazepine receptor agonists, melatonin, antidepressants, antipsychotics, and antihistamines [6]. Unfortunately, according to clinical studies, about 40% of patients do not reach remission with treatment even after a period of 6 mon [7]. Moreover, some health professionals refrain from prescribing them the use of hypnotics as it can lead to dependence and intolerance [6].
Vitamin B6 (VitB6) or pyridoxine is a water-soluble vitamin found in foods (e.g., viscera, whole-grain cereals, and soy beans), plays a role in macronutrients synthesis, and acts as a coenzyme in pathways involving the neurotransmitters like serotonin. Thus, VitB6 has been often used as a sleep medication ingredient and reported to influence sleep. Preliminary results from a clinical study showed that VitB6 supplements enhance dream recall capacity, influencing the dream perception as a more vivid and colorful experience [8].
Poly-γ-glutamic acid (γ-PGA) is a polypeptide made of D- and L-glutamic acid units connected by an amide linkage. γ-PGA is a glutamate derivate, an excitatory neurotransmitter that can be converted to γ-aminobutyric acid (GABA). GABA, which is synthesized in the presynaptic neuron cytoplasm by glutamate decarboxylase (GAD) using VitB6 as a cofactor, is well known as an inhibitory neurotransmitter having calming effects, acting as a sleep inducer [9]. A previous animal study observed a significantly elevated glutamate and an increasing trend in GABA concentrations in serum after γ-PGA supplementation [10], but did not evaluate the γ-PGA effects on sleep status. In the best of our knowledge, so far, there is no epidemiological study conducted to test the effects of γ-PGA supplement on sleep status. Thus, this study conducted interventions to evaluate whether individual or combined supplementation with γ-PGA and/or VitB6 would improve sleep duration and sleep quality in healthy adults.
Go to : 
SUBJECTS AND METHODS
Study design and participants
This was a randomized, double-blinded, placebo-controlled crossover intervention study. The participants' recruitment process included announcement letter posting about this study on the Kookmin University bulletin board and neighboring buildings (residential apartments, health centers, grocery stores, etc.). When a person informed his/her interest to participate in the study (via phone call, email, or Google survey), the research team contacted them back to conduct a screening evaluation via phone call. The study participants' inclusion criteria were as follows: adults aged 20−65 yrs with no chronic disease history, including CVD, diabetes mellitus, cancer, hepatic disease, or kidney disease. Individuals who were regularly taking medications to treat a condition, pregnant, currently taking dietary supplements, or had allergic symptoms or an anemia diagnosis in the last 3 mon were excluded from the study. Eligible subjects were invited to participate in face-to-face meetings and enrolled after they signed an informed consent form, which was approved by the Human Subjects Review Committee of Kookmin University (KMU-201808-HR-184). The study's protocol was registered in the Clinical Research Information Service (KCT0005083).
All enrolled participants were randomly allocated considering age and gender (stratified random allocation) into 3 intervention trials: the ‘Group A’ trial evaluated γ-PGA supplementation only, the ‘Group B’ trial evaluated VitB6 supplementation only, and the ‘Group C’ trial evaluated a combined γ-PGA and VitB6 supplementation. The participants were assigned to one of the three intervention groups stratified by age and sex; each participant was randomly allocated to either intervention or placebo sub-group. Among the 130 recruited individuals, a total of 72 were enrolled, allocated to the groups, and participated in 4 examinations over 12 weeks; first baseline examination (Exam 1), first follow-up examination (Exam 2), second baseline examination (Exam 3), and second follow-up examination (Exam 4) with a 4-week period between each examination (Fig. 1). After a 4-week washout period between Exams 2 and 3, the study participants in the intervention and placebo groups were switched. Finally, 47 participants completed all examinations conducted in the Kookmin University facilities. We performed a power analysis using the G*Power program (version 3.1.9.2;Heinrich Heine University Düsseldorf Universität, Düsseldorf, Germany) to confirm the sample size appropriateness. Thus, a sample of 30 subjects (10 for each intervention) would provide the non-parametric test a 90% power at a two-sided significance level of 5%. Considering the 30% average dropout rate in clinical trials, at least 39 subjects were needed.
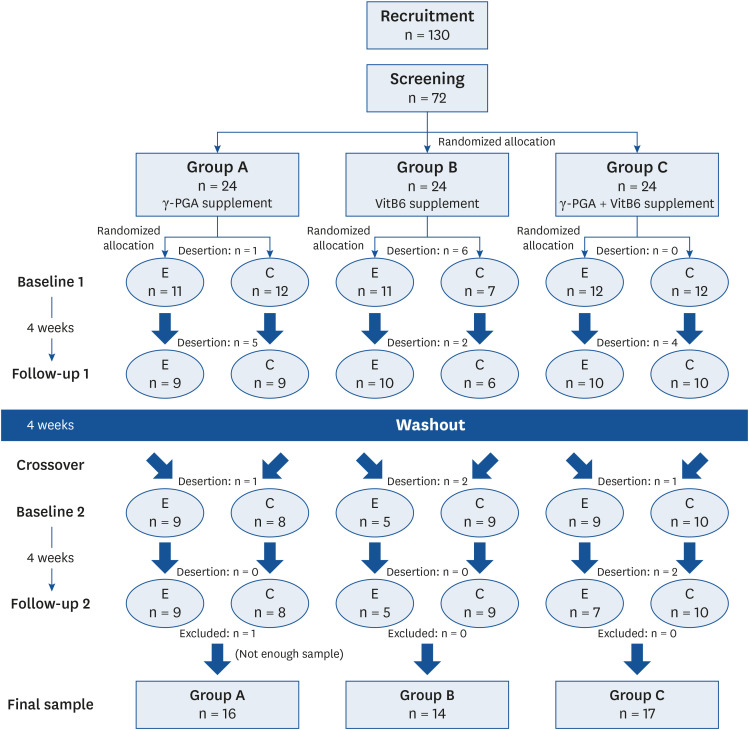 | Fig. 1Study flowchart.Group A received γ-PGA supplementation only; Group B received VitB6 supplementation only; Group C received both γ-PGA and VitB6 supplementation. The number of participants who were enrolled, dropped out, and completed the trial by interventions in the randomized, double-blinded, placebo-controlled, and crossover study.
γ-PGA, poly-γ-glutamic acid; VitB6, vitamin B6.
|
Questionnaire data collection
All participants answered questionnaires, including their demographic characteristics, lifestyle habits, caffeine-containing beverage consumption, supplementation side effects, and sleep status. Particularly, sleep status was asked using Pittsburgh Sleep Quality Index (PSQI) [11] and Epworth Sleepiness Scale (ESS) [12], which are reliable instruments and have been validated in prior studies [131415]. Sleep duration was calculated based on the information on usual bed time and getting up time in the PSQI questionnaire. All questionnaires were inquired in the four examinations. Additionally, the food frequency questionnaire developed by the Korea Disease Control and Prevention Agency (available in the website, http://www.cdc.go.kr) was inquired in the last examination only. The participants were advised not to change their habitual sleep and diet status during the study duration.
Anthropometric measurement
Anthropometric measurements were conducted in every examination. Body weight and height were measured using a digital scale and a stadiometer (CAS, Seoul, Korea) and rounded to the nearest 0.1 kg and 0.1 cm, respectively. The participants were asked to remove coats, shoes, caps and any belongings from their pockets and adopt an erect posture while measurements were obtained. Body mass index (BMI) was calculated with body weight (kg) and height squared (m2).
Biospecimen collection and assay
Blood samples were collected by a health professional in each study examination. Serum samples were stored in an ultra-low temperature freezer (−75°C constant temperature) until biochemical assays. The samples were sent to a commercial laboratory for serotonin assays using a competitive enzyme-linked immunosorbent assay kit (LDN, Nordhorn, Germany).
Supplementation method
A γ-PGA powder form (Vedan Enterprise Corporation, Taichung City, Taiwan) and a VitB6 tablet form (Junsei Chemical Co., Tokyo, Japan), which was ground into a powder before administration, were purchased for the study. Cornstarch powder was purchased at the local supermarket to use as placebo. The daily VitB6 dose was 100 mg, corresponding to the tolerable upper intake for female and male adults according to the 2015 Dietary Reference Intakes for Koreans [16], while the daily γ-PGA dose was 600 mg, which is below the approved level of the Ministry of Food and Drug Safety [17]. Additionally, there are no reports of toxic side effects from the γ-PGA use [1819].
Each participant received a calendar with 30 pockets containing an envelope with the proper amount of γ-PGA or/and VitB6 supplement or cornstarch powder (placebo). The participants were instructed to take one envelope (containing the assigned supplement) every night 1 h before going to sleep. Thus, groups A, B, and C received 600 mg of γ-PGA, 100 mg of VitB6, and mixture of γ-PGA (600 mg) and VitB6 (100 mg), respectively. Placebo envelopes contained cornstarch powder in the same amount as the supplementation dose in each trial.
Statistical method
Descriptive statistics were presented as mean ± SD or proportions. The paired t-test and nonparametric methods (Wilcoxon signed-rank test) were used to analyze differences between the baseline and follow-up variables and consider statistical significance at P < 0.05 in a two-sided test. The SAS v.9.4 software (SAS Institute Inc., Cary, NC, USA) was used to analyze the data.
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Kookmin University IRB committee (KMU-201808-HR-184) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All participants were engaged in this study voluntary and signed an informed consent.
Go to :
RESULTS
Baseline and follow-up outcomes
After a 2-week recruitment period followed by a 12-week total trial duration (mid-November 2018 to February 2019), 16 participants in group A, 14 in group B, and 17 in group C completed the 4 examinations (Fig. 1).
There were no significant differences in the baseline characteristics including BMI, caffeine intake, sleep duration, PSQI, ESS, and serum serotonin levels between the intervention and placebo groups within each intervention (Table 1).
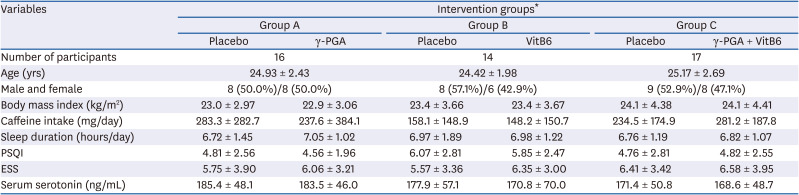
Table 1
Baseline values for the general characteristics and sleep status variables according to the three intervention groups
Variable values are presented as mean ± SD.
γ-PGA, poly-γ-glutamic acid; VitB6, vitamin B6; PSQI, Pittsburgh Sleep Quality Index; ESS, Epworth Sleepiness Scale.
*Group A received γ-PGA supplementation only; Group B received VitB6 supplementation only; Group C received both γ-PGA and VitB6 supplementation.
![]()
There were no significant differences in the follow-up characteristics (after intervention) between the intervention and placebo groups within each intervention (Table 2). All participants reported no side effects in any group after supplementation.

Table 2
Follow-up values for the caffeine intake and sleep status variables according to the three intervention groups
Variable values are presented as mean ± SD.
γ-PGA, poly-γ-glutamic acid; VitB6, vitamin B6; PSQI, Pittsburgh Sleep Quality Index; ESS, Epworth Sleepiness Scale.
*Group A received γ-PGA supplementation only; Group B received VitB6 supplementation only; Group C received both γ-PGA and VitB6 supplementation.
![]()
Changes before and after supplementation
Table 3 shows the comparison between the groups in terms of the differences in sleep status variables, serum serotonin levels, and caffeine intake before and after supplementation for each intervention. Statistical significance was tested when the differences before and after supplementation for the intervention were compared with those for the placebo. There were significant differences between the intervention (a γ-PGA and VitB6 supplementation mixture) and the placebo of group C for sleep duration and PSQI global scores (P < 0.05). When compared with the placebo, the intervention showed an increase in the total sleep duration (mean ± SD, 0.27 ± 0.98 h) and a decrease in PSQI global scores (−0.52 ± 1.58). The placebo showed a decrease in sleep duration (−0.25 ± 1.25 h) and an increase in PSQI global scores (0.64 ± 1.93). No significant findings for other variables were observed in group C. There were no significant findings for sleep status variables, serum serotonin levels, and caffeine intake in groups A and B.

Table 3
Differences in the baseline and follow-up values according to the three intervention groups
Variable values are presented as mean ± SD.
γ-PGA, poly-γ-glutamic acid; VitB6, vitamin B6; PSQI, Pittsburgh Sleep Quality Index; ESS, Epworth Sleepiness Scale.
*Group A received (γ-PGA supplementation only; Group B received VitB6 supplementation only; Group C received both γ-PGA and VitB6 supplementation. †P<0.05 when being compared with a placebo group in each intervention. Comparison was performed using a nonparametric test.
![]()
Go to :
DISCUSSION
This study explored the γ-PGA and VitB6 supplementation effects on sleep-related variables in a randomized, double-blinded, placebo-controlled, crossover study. We found that the study participants with dual γ-PGA and VitB6 supplementation have increased sleep duration and improved sleep quality (indicated by reduced PSQI global score).
γ-PGA is known to be produced by chemical synthesis, peptide synthesis, biotransformation, or microbial fermentation. Its cost-effective production is through fermentation by Bacillus subtilis strains in foods like Korean chungkookjang or Japanese natto [2021]. Nowadays, γ-PGA is widely used in the food industry as an ingredient, a texture enhancer, an oil reducing agent, and a bitterness-relieving agent [22]. Regarding its biological role, some studies have suggested that γ-PGA supplementation may improve disturbed lipid metabolisms and adiposity [23] and may have immune-stimulating and antitumor activity [18] and anti-inflammatory effects [19]. Another study has explored the relationship between γ-PGA and minerals and showed increased calcium absorption due to the γ-PGA supplementation [24]. Currently, there is limited data from a human study on the γ-PGA supplementation effects on sleep status, with only a few on animal studies that provide data reflecting its potential role in sleep regulation. An animal study observed elevated glutamate and GABA concentrations in serum and brain tissue after γ-PGA administration [10]. In this experiment, rats showed significantly elevated serum and brain glutamate levels and an increasing trend in brain GABA concentrations after γ-PGA administration [10]. Another animal study demonstrated increased serum GABA concentrations in rats after γ-PGA administration and improved abnormal metabolic status resulting from sleep disturbance [25]. GABA is the main neurotransmitter with an inhibitory function in the central nervous system (CNS) with around 20% of the GABA neurons in the brain, having activity linked to serotonin (or 5-hydroxytryptamine [5-HT]) modulation. The 5-HT3 subunit increases GABA and glutamate releases, and the 5-HT2 subunit increases GABA and either increases or reduces glutamate release. The 5-HT1A/5-HT1B reduces GABA and glutamate releases in the brain [26]. Glutamate, which is a GABA precursor, is an excitatory neurotransmitter in the CNS regulating wakefulness by acting on the ascending reticular activation system, a glutamatergic zone in charge of the sleep-wake transitions. The arousal effect of glutamate is mediated by N-methyl-D-aspartate and histamine H1 receptors [27]. The glutamate levels of the orbitofrontal cortex increase during rapid eye movement (REM) sleep, while its lowest levels are observed during non-REM sleep [28]. To synthesize GABA from glutamate, GAD enzyme requires VitB6 as a coenzyme [29]. In fact, insufficient VitB6 intake was reported to modulate the gene expression of the enzymes involved in GABA, glutamate, and serotonin metabolism [30].
There are accumulating data regarding the relationship between GABA supplementation and sleep with no clear conclusion to date due to inconsistent findings [31]. It has been accepted that ingested GABA is unable to pass through the blood-brain barrier (BBB) [32], a semipermeable border formed by vessels, regulating the influx and efflux between the blood and the brain to protect neural tissue and function [33]. A few studies have suggested that GABA can pass through the BBB only in small amounts [31]. An animal study evaluating the GABA supplementation effect on sleep found that ingested GABA can alleviate a caffeine-induced effect, stimulating sleep disruption [34]. Another study found that GABA-containing black tea can improve sleep status by shortening latency and prolonging sleep duration [35]. Some studies have explored the effect of GABA together with additional components. One found that the GABA and L-theanine combination has a synergistic effect on sleep by decreasing sleep latency and improving non-REM sleep [36]. Another study found that the GABA and 5-hydroxytryptophan combination improves sleep quality more than the administration of the two substances individually [37].
In our study, neither γ-PGA supplementation nor VitB6 supplementation showed any significant effects, but the combined supplementation of γ-PGA and VitB6 resulted in a significant improvement in sleep duration and quality. Regarding the dual supplementation effects, several potential underlying mechanisms can be suggested. We speculated that the gut microbiota may contribute to glutamate production using supplemented γ-PGA. In particular, γ-PGA supplementation may act as a prebiotic compound, and the degradation of γ-PGA to glutamate may be performed by enzymes from bacteria, such as Bacillus subtilis [38]. Produced glutamate and supplemented VitB6, which can pass through the BBB, may be used to synthesize GABA in the brain, and then increased GABA levels may induce sleep.
The study limitations should be considered when our findings are interpreted. First, we cannot rule out the possibility that the lack of significant findings in groups A and B might be due to inadequate power. However, group C has a similar number of participants to that of group A. Second, the study participants who dropped out were not included in the analysis, despite having minimal impact on the results. The major strength of this study is the randomized, double-blinded, placebo-controlled, and crossover design. Due to these attributes and the bio-safety of the interventional treatments used, this study's nature can be extended, hence generalizability attained. Further studies, including a large sample or a population with various ethnicities or with coexisting health conditions, are warranted.
In summary, this intervention study provided novel data that the supplementation combination of γ-PGA and VitB6 improves sleep duration and quality, suggesting these active and safe ingredients as potential candidates for sleep treatment.
Go to :
 XML Download
XML Download