

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
While coronavirus disease 2019 (COVID-19) spreads across the globe, many countries have closed schools to ensure physical distancing to slow transmission and ease the burden on health systems. The nationwide school closures are estimated to affect over 60% of the world's student population.1 After launching online classes in April 2020, Korean Ministry of Education provided flexible instruction like blended learning of online and offline classes to Korean students with the means to safely achieve their academic goals in the face of changing caseloads of COVID-19.2 Many families are turning to digital solutions to support children's learning, socialization, and play, which provide opportunities for sustaining and promoting education but may increase exposure to online risks.1 Our previous study shows growing tendency of media device use and its adverse effects among preschool children in Korea.345 Although the scientific debate is ongoing about the effect of school closures on virus transmission,6 prolonged partial closures of schools could have detrimental social and health consequences for children and may exacerbate existing inequalities.7
Research shows that the mental health burden of disasters across communities is pervasive for both individuals and families.8 In the case of COVID-19, it is different from previous disasters in that it is not a single disaster (earthquake, terror, accident etc.) but a long-lasting disaster affecting many areas of family life. Any family members can have fears and concerns related to COVID-19, which can lead to tremendous stress and psychological distress. Parents are responsible for explaining the pandemic to their children, and managing their fear and anxiety arising from uncertainties as well as various adversities caring for their children.
In South Korea, with the enactment of the Mental Health Act in 1995, community-centered mental health projects were established. Despite the positive effect of community-based mental health centers, the utilization of professional mental health services appears to be low.9 Suwon, where the study was conducted, is a relatively well-serviced city with four independent, specialized mental health centers, unlike other cities or districts with one mental health center responsible for various tasks. During epidemics, psychosocial support is as important as infection control, and collaboration and networking are the key to disaster management. Therefore, a multidisciplinary team of mental health professionals was immediately established and effectively working with internal and external stakeholders to provide psychosocial support during the COVID-19 outbreak. The effectiveness of disaster management by mental health care professionals will be evaluated later.
This study identified a range of parental concerns, and examined whether parental stress or depression were positively associated with children's behavior problems, sleep problems, and media exposure during COVID-19-related primary school closures.
METHODS
Study design and participants
COVID-19 spread rapidly around the world after it was reported in early 2020. Many governments implemented social distancing strategies to prevent the spread of the disease, encouraging employees to work from home and closing schools and childcare facilities.10 In South Korea, students received an online-only curriculum instead of physically attending school from March to May of 2020, without a strict social lockdown. This study was conducted in June of 2020 to investigate children's characteristics, problematic behaviors and media usage, including online learning patterns, during the primary school closure. It also identified factors related to parental mental health including their concerns, subjective stress and depression that significantly impacted children's mental health. The data include the baseline survey results collected from June 1–30, 2020, approximately three months after South Korea's online curriculum was implemented.
We recruited 217 caregivers of primary school children, including 97 children who had already participated in the Kids Cohort for Understanding of Internet Addiction Risk Factors in Early Childhood (K-CURE) study,11 from community centers in Suwon City, Gyeonggi Province, South Korea. Parents who contacted the study team were e-mailed a link to the questionnaire. Participants who consented to the study and met inclusion criteria completed the survey and were rewarded for their time ($5 worth of masks and hand sanitizer). The inclusion criteria were: 1) parents of primary school children, 2) parents whose children received an online-only curriculum during COVID-19-related school closures, and 3) parents able to read and write Korean.
Measures
After providing online consent for themselves and their children, caregivers (mostly parents) were sent a link to a webpage of study instructions and the online research survey. They used this survey to report their demographic data and that of their children.
Children's body mass index and activity levels
Children's body mass index (BMI) was calculated from parental reports of height and weight.
Children's activity levels were assessed with the question “How has your child's daily activity changed since COVID-19 compared to a year ago?” Caregivers answered using the following response options: “not changed,” “decreased by less than two hours,” “decreased by less than four hours,” “decreased by over four hours,” “increased by less than two hours,” “increased by less than four hours,” and “increased by over four hours.”
Media usage
Unlike previous K-CURE studies,11 we did not distinguish between weekdays and weekends for media usage, as we assumed that children's time at home would not differ between weekdays and weekends with social distancing in place and schools closed.
Media usage was assessed by asking primary daytime caregivers to report the frequency of their children's media device usage (TV, tablet PC, and smartphone). We asked caregivers to list their children's favorite three types of media content used in the last three months, or when school was closed.
Children's sleep and behavioral problems
Children's sleep problems were assessed with a six-item sleep quality and ritual survey from the Children's Sleep Habits Questionnaire (CSHQ), developed by Owens et al.12 in 2000. The survey assesses several key sleep domains that encompass the major clinical sleep complaints in this age group. We used the short version of the CSHQ, which covers 1) sleep onset, 2) sleep regularity, 3) sleep duration, 4) anxiety around sleep, 5) night waking, and 6) morning waking difficulties. Parents were asked to recall sleep behaviors occurring over a “typical” recent week. Items were rated on a three-point scale as “frequently” if the sleep behavior occurred five to seven times/week, “often” for two to four times/week, and “rarely” for zero to one time/week. Item scores were summed to create a score ranging from 0 to 12, with higher scores representing bigger sleep problems.
Behavioral problems were assessed with the Behavior Problem Index (BPI), consisting of 28 items (32 items for children 12 years of age or older) on which caregivers rated their children using a three-point Likert-type scale (0 = not true, 1 = sometimes true, 2 = often true).13 These questions assess specific behaviors that children may have exhibited in the previous three months. The psychometric properties of the BPI reported in previous studies include high estimates of internal consistency for the full instrument.1314 In the current study, Cronbach's α was .92.
Parental mental health (subjective stress, depression, their concerns)
Parental subjective stress was assessed with the question “Please write the number that best describes your level of stress over the past week. If stress is very high, write a 10, and if it is low, write 0.”
Parental depression level was assessed with the Patient Health Questionnaire-9 (PHQ-9).15 The PHQ-9 is a self-report measure that asks if the subject has experienced the following problems in the past two weeks: 1) little interest or pleasure in doing things, 2) feeling down, depressed, or hopeless, 3) trouble falling or staying asleep, or sleeping too much, 4) feeling tired or having little energy, 5) poor appetite or overeating, 6) feeling bad about yourself, 7) trouble concentration on things, 8) psychomotor retardation or agitation, and 9) suicidal thoughts. Subjects were asked to rate how often each symptom occurred: 0 (not at all), 1 (several days), 2 (more than half the days), or 3 (nearly every day). Cronbach's α in this study was 0.90.
Parental concerns were assessed with the question “Please answer Yes or No about having your concerns regarding the current COVID-19 pandemic” for the following 12 areas: C1, losing a loved one to COVID-19, C2, getting sick or dying from COVID-19, C3, being infected and being stigmatized, C4, unstable social atmosphere, C5, failure to receive adequate treatment due to an overload of the medical system, C6, economic recession, C7, unemployment in the family, C8, school suspension and closure, C9, difficulty in caring for children (e.g., problems finding daytime caregivers), C10, changes in your children's friendships, C11, a worsening relationship with your child, C12, a worsening relationship with your spouse.16
Other family factors
Household income was assessed with the question “What is your average monthly household income?” Caregivers chose from the following response options: “less than $1,700 (2,000,000 Korean won, 2M KRW),” “$1,700 (2M KRW) to $3,400 (4M KRW),” “$3,400 (4M KRW) to $5,000 (6M KRW),” and “over $5,000 (6M KRW).”
Household income changes after COVID-19 were assessed with the question “Has your household income changed since COVID-19?” Caregivers chose from the following response options: “not changed,” “increased,” and “decreased.”
Changes in primary caregiver, availability of the regular daytime caregiver, and recent adverse life events were assessed with the questions “Has the person who parents or cares for your child changed since COVID-19?” “Has anyone cared for your child regularly during the daytime since COVID-19?” and “Have there been any adverse life events in the family since COVID-19?”
Statistical analyses
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 25.0 (SPSS Inc., Chicago, IL, USA), and a P value of < 0.05 was considered statistically significant. Data were cleaned by checking for completeness and value range. Variables were summarized with descriptive statistics for demographic information, including frequencies, means, and standard deviations. The t-test or analysis of variance was used for data composed of continuous variables, and the Kruskal-Wallis test was used for sequence-scale data. A χ2 test was used to compare the rate of parental concern responses by group. The Pearson correlation coefficient was used to measure the strength of the linear association between the parental mental health and other variables.
Ethics statement
This study was approved by the Institutional Review Board (IRB) at the Ajou University School of Medicine, Suwon City, South Korea (IRB No. AJIRB-SBR-SUR-14-378). Informed consent was obtained from all participants at enrollment. Data were collected through a web-based questionnaire platform to keep physical distancing and ensure survey quality. Participants could withdraw from the survey at any time without justification.
RESULTS
Descriptive characteristics
Demographic data are shown in Table 1. We invited 217 parents of children aged 7–12 years to participate in the study and analyzed demographic data. The average age of the children was 9.16 years, and the average BMI was 18.14. There was an average increase in weight of 1.8 kg noted in children during the three months after COVID-19 began, and 30.1% of children showed an increase of 3 kg or more (the greatest increase was 10 kg).17 According to parents, 80.2% of children spent less time being physically active when they were unable to attend school physically due to COVID-19, and 21.7% of children had a decrease in physical activity of more than four hours. The rate of parents (mainly mothers) as regular daytime caregivers changed from 94.6% to 70.5% and that of grandparents changed from 4.1% to 12.0%. Also, 10.6% of families lacked a regular daytime caregiver when children were unable to attend school.
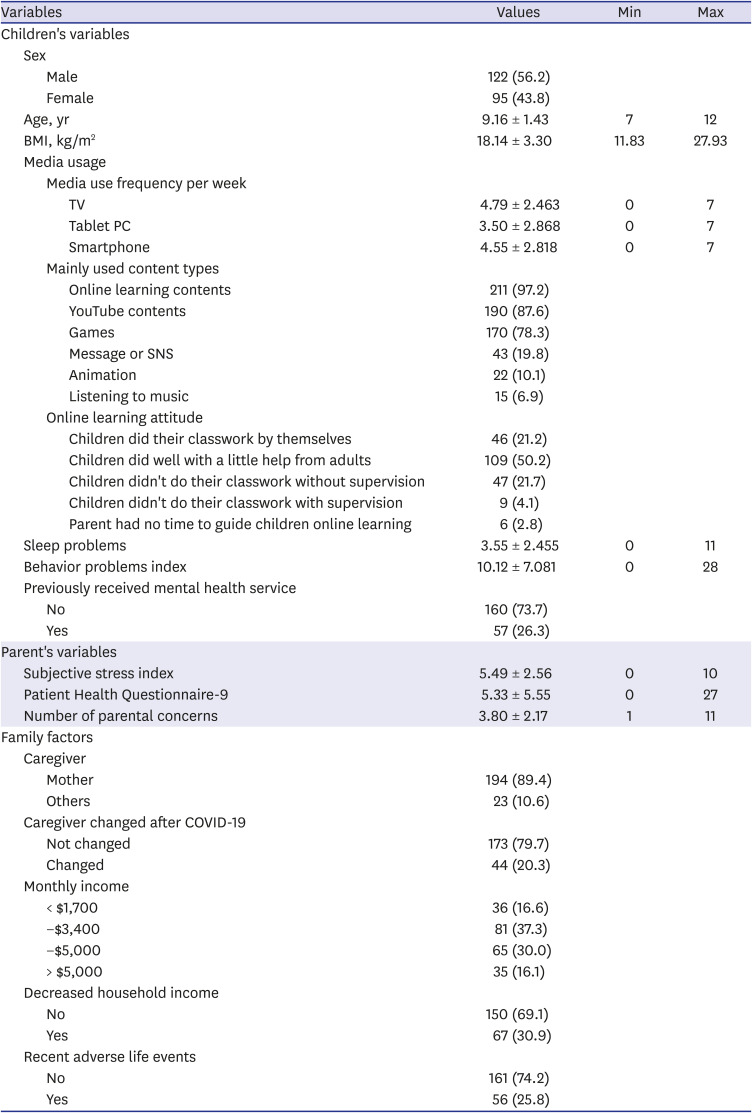
Table 1
Demographic characteristics of study sample (n = 217)
Values are presented as number (%) or mean standard ± deviation.
N = number, Max = maximum, Min = minimum; BMI = body mass index, COVID-19 = coronavirus disease 2019.
![]()
Media usage pattern
Children's media usage pattern is shown in Table 1. Media usage was mainly observed by daytime caregivers who chose the top three types of media content. Almost all children (97.2%) used online learning content during school closures, 87.6% of children used YouTube contents, 78.3% of children used games, 19.8% of children used messages or SNS, 10.1% of children watched the animation, and 6.9% of children used digital devices for listening to music.
Parental reports on their children's online learning attitudes demonstrated that 6.9% of parents stated their children's online learning activities did not go well. 2.8% of parents did not have time to observe with guidance and 4.1% had trouble with their children's online learning despite having supervision. 50.2% of parents reported that their children did well with a little help from parents, and 21.2% reported that their children did their classwork by themselves.
Comparison of parental concerns between the mental services-received groups and non-serviced groups
Parents reported various concerns related to COVID-19, children factors, family factors, ranging from 1 to 11. Many parents were concerned about unstable social atmosphere (59.9%), economic recession, school suspension (59.4%), their children's social relationships (36.4%), and COVID-19 infection (36.4%). According to the change of caregivers, economic difficulty, and adverse life events in the family, differences in the content of parental concerns existed between the groups (Supplementary Table 1).
There were 57 children who previously received mental health services (26.3%) (Table 1). Parents in the serviced group were more concerned about C9; difficulty in caring for children and C10; changes in their children's friendships, while parents in the not serviced group were about C3; being infected and being stigmatized, and C8; school suspension and closure. There were no statistically significant differences in other parental concerns (Table 2).

Table 2
Comparison of parental concerns between the mental services-received group and non-serviced group
C1, losing a loved one to COVID-19; C2, getting sick or dying from COVID-19; C3, being infected and being stigmatized; C4, unstable social atmosphere; C5, failure to receive adequate treatment due to an overload of the medical system; C6, economic recession; C7, unemployment in the family; C8, school suspension and closure; C9, difficulty in caring for children (e.g., problems finding daytime caregivers); C10, changes in your children's friendships; C11, a worsening relationship with your child; C12, a worsening relationship with your spouse.
SG = group previously received mental health services, NG = group did not receive mental health services, COVID-19 = coronavirus disease 2019.
*P < 0.05, **P < 0.01.
![]()
Association of parental mental health and children's problematic behavior, media usage
The average parental subjective stress index, ranging from 0 to 10, was 5.49 and depression, ranging from 0 to 27, was 5.33 (Table 1). Parental depression was evaluated by the PHQ-9, and 46.5% of parents reported depressive symptoms. The results showed that 29.0% of parents had mild depressive symptoms, 13.4% had moderate depressive symptoms, and 4.1% had severe depressive symptoms based on the PHQ-9 cutoff scores. The PHQ-9 item on self-harm and suicidal ideation showed that 10% of parents reported suicidal thoughts and 1.4% reported suicidal thoughts nearly every day in the past two weeks.
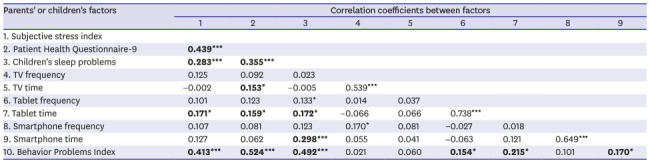
In Table 3, parental subjective stress index was highly associated with parental depression (Pearson correlation 0.439, P < 0.001), children's sleep problems (0.283, P < 0.001), tablet time (0.171, P = 0.012) and behavior problems (0.413, P < 0.001). Parental depression was associated with children's sleep problems (0.355, P < 0.001), TV time (0.153, P = 0.024), tablet time (0.159, P = 0.019), and behavior problems (0.524, P < 0.001). Children's sleep problem was associated with tablet (0.172, P = 0.011) and smartphone time (0.298, P < 0.001) but not its frequency.
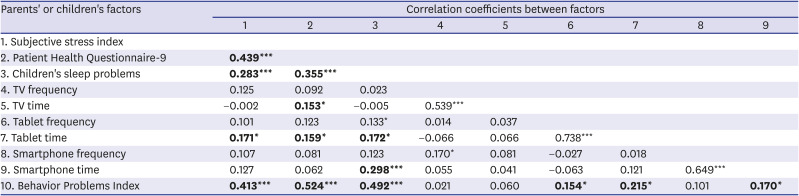
Table 3
Correlations between parental mental health related to coronavirus disease 2019 and children's psychological/behavioral factors (n = 217)
![]()
DISCUSSION
Our study shows various parental concerns related to COVID-19, children factors including children's media usage and behavioral problems, and family factors. According to the changes of family factors during COVID-19 related school closures, we tried to identify the characteristics of parental concerns and the correlation with children's factors. Time-sensitive research identifies parental stressors related to COVID-19, including disruptions to work/learning, daily self-care routines, fears of infection and a lack of access to reliable resources and information.1618 Reports from families suffered from COVID-19 in the States indicate that these stressors are elevated in caregivers,19 although it is not well-known about how this increased stress will impact child-parent relationships.20 High levels of caregiver burden and psychological distress may complicate the balance between parallel care responsibilities. Parents may sacrifice their well-being to meet their children's needs, especially mothers, who frequently assume the role of primary caregiver.21
Compared to our previous study,22 this study showed that moderate to severe parental depression (17.5%) was higher than previous results (14.7%) and mild depression (29.0%) was doubled. This pandemic has had a huge economic impact and has put financial strain on many families. Factors such as economic downturn and unemployment, declining incomes, and unmanageable debts are significantly associated with declining mental health, increased rates of substance-related disorders, mental disorders, and suicidal behaviors.23 These risks also apply to parents.24 The recent recession draws attention to the fact that low socioeconomic status is a well-known risk factor for worsening children's mental health. Parental mental health significantly influences parent-child relations25 and increases the risk for children's mental health problems.26 School closures, despite being an important and powerful public health intervention for epidemics/pandemics, can have adverse effects on children and adolescents.27 Not only are they not receiving an education—with potential lifelong implications—but children from deprived backgrounds are at increased risk of hunger (from missing free school meals), domestic violence, and the poverty that ensues from parents being unable to work because of daytime parenting responsibilities. These consequences are most likely greatest for the most vulnerable members of society. The longer lockdowns continue, the greater the risks are for the young and the disadvantaged.
Suwon has a mental health community center only for children and adolescents and makes it easy to access mental health services. Children who previously received mental health services reported having more sleep problems (t = 3.533, P = 0.001) and behavioral problems (t = 7.216, P < 0.001) and parents in the serviced group reported higher levels of subjective stress (t = 2.940, P = 0.004) and depression (t = 4.056, P < 0.001) (Supplementary Table 2). Interestingly, there is a difference in the parental concerns content between the serviced group and non-serviced group. In the serviced group, parents seemed to be more concerned that the problems their children already have (difficulty in caring for children, changes in children's friendships, worsening relationships in the family) are getting worse because of COVID-19 than the disease itself and consequences (losing a loved one, getting sick, infection and stigmatization, school suspension).
Our previous study shows an increase in the tendency of media device use and its adverse effects among preschool children in Korea.345 Online learning has many advantages of education equalities but high risks for online exposures. In this study, only 6.9% of parents reported that their children's online learning activities did not go well and it is fortunate that online education was relatively well-working. But, almost all children (97.2%) used online learning content during school closures, 87.6% used YouTube content, 78.3% used games, 19.8% used messages and SNS, 10% watched animations, and 6.9% of children used digital devices for listening to music. Increased online activity supports children's learning, socialization, and play but also puts them at heightened risk of sexual exploitation and cyberbullying. Even before COVID-19, children were increasingly using a variety of screen devices on a regular basis. Pre-pandemic, children's time using mobile devices had tripled from 2013 to 201728—with children under eight using screens for almost 3 hours per day. During the COVID-19 pandemic, caregivers noted that YouTube was children's most commonly used video platform, with over 78% of children watching.2930 Parents and caregivers, meanwhile, are being asked to navigate their children's shift online while balancing work and other uncertainties related to the pandemic. Not all online risks translate into actual harm, but children facing other issues in their lives may be more vulnerable to these threats. Mitigating risks should be balanced with children's freedom of expression, access to information, and privacy. Keeping children informed, engaged, and empowered with internet safety skills is critical. Governments and companies should support parents with appropriate guidance and tools, including how to respond to and report harmful contact, conduct, and content. One growing area of interest is children's exposure to disaster-related media.31 Parents have a significant role in determining their children's media exposure to such events. Research shows that media exposure to disasters is connected to posttraumatic problems in young people.32
Our study suggests that parental subjective stress and depression was strongly and positively associated with children's sleep problems, media exposure, and problem behaviors. Caring for children with mental health problems, especially externalizing disorders, can be very difficult during lockdowns. A myriad of mental health threats are associated with the current pandemic and subsequent restrictions. Child and adolescent psychiatrists must ensure continuity of care during all phases of the pandemic. The mental health risks associated with COVID-19 will disproportionately affect already disadvantaged and marginalized children33. American parents, on average, feel significantly higher levels of stress than adults without children. Parents report stressors related to their children's education, basic needs, access to health care services, and missing out on major milestones.34 The report points out that rates of reported caregiver burden among the nearly half of the sample who lack adequate financial resources is significantly higher. This highlights the potential heightened mental health needs of economically vulnerable people as noted by similar COVID-19 surveys of the general population. In parents of children under age 18, the average reported stress level over the past month related to the coronavirus pandemic was 6.7, compared with 5.5 for adults without children. Nearly half of parents (46%) said their stress level was high (between 8 and 10 on a 10-point scale, where 1 indicates “little or no stress” and 10 indicates “a great deal of stress”) compared with 28% of adults without children.
The results presented here provide time-sensitive information about families' experiences during school closures due to the COVID-19-pandemic; however, some limitations should be noted. First, there is no pre-pandemic baseline assessment compared to our results about families' experiences during the pandemic. Longitudinal data are required for more robust inference beyond those possible with cross-sectional data. Second, attention should be paid to the generalizability of the sample. Although these sample results may not be as representative as those from a probability sample, they are one of the first data available on the complex stresses for parents during COVID-19. Third, as we used a web-based survey method to avoid possible infections, our sampling was voluntary and conducted via an online system. Therefore, we must consider the possibility of selection bias.
In this study, we provided evidence on the association between parental mental health and their children's problem behaviors as well as media exposure in South Korea during the COVID-19-related school closures. The higher level of parental mental health risk was associated with more sleep problems, problem behaviors, and greater time spent on media usage of their children. Parents who have previously received mental health services may constitute a more vulnerable group as they reported higher rates of parental stress, depression, and more concerns. Therefore, ongoing monitoring of mental health at risky group and multiple support systems may need to be expanded to cover those parents having difficulty in caring for their children.
 XML Download
XML Download