

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Graft failure (GF) after allogeneic hematopoietic stem cell transplantation (HCT) is a vexing problem with respect to adverse outcomes and the absence of established management guidelines. In recent studies, the reported incidence of primary GF is 0.6–9.6% and secondary GF is 1.7–5.0%.12345 Recognized risk factors for development of GF are marrow failure syndromes including severe aplastic anemia (AA) and myelofibrosis, low CD34+ cell yield, T-cell depleted graft, reduced-intensity conditioning (RIC) regimen, human leukocyte antigen (HLA) mismatch, ABO disparity, and poor Karnofsky performance status at the time of transplant.126789101112131415 Expert opinion recommends rescue allogeneic transplantation as salvage treatment in the setting of graft failure, however data drew comparison between different types of management in GF is very limited.
A small proportion of patients achieve autologous reconstitution (AR) after GF, in which a patient recovers from cytopenia with original recipient lineage without evidence of relapse. Previous reports mentioning autologous recovery in GF associated with transplantation for acute leukemia are very limited. In a retrospective study comprising 1,205 recipients transplanted for severe AA, the cumulative incidence of AR was 4.2%.3 In another retrospective cohort consisting of 1,726 allogeneic HCT recipients, 9 cases of AR occurred after primary GF.5 In AR cases after HCT for chronic myeloid leukemia (CML) reported by Brunstein et al.16, the AR group exhibited prolonged survival with a relapse rate of 80%.
This study reviewed a retrospective cohort of 1,630 patients who underwent allogeneic HCT for malignant disease or severe AA in a single center during an 18-year period. We analyzed pretransplant risk factors of GF, management, outcomes and AR after GF.
METHODS
Definitions
Primary GF
Primary GF is defined as the absence of absolute neutrophil count (ANC) recovery more than 500/µL in the first 28 days after HCT. Chimerism analysis using DNA short tandem repeat (STR) polymerase chain reaction was performed to confirm graft loss at day 28 after HCT.
Onset of secondary GF
Onset of secondary GF was defined as the date of ANC became under 500/µL after donor cell reconstitution, followed by confirmation with chimerism analysis.
Study population
Between January 2000 and September 2017, data of 1,798 consecutive patients were recorded in the HCT registry of Asan Medical Center in Seoul, South Korea. After exclusion of early mortality and relapse before reaching 1 month of HCT, the study population consisted of 1,630 patients. Thirteen patients were determined to experience primary engraftment failure. Sixty-nine patients experienced secondary GF. The patient selection process is summarized in Fig. 1.
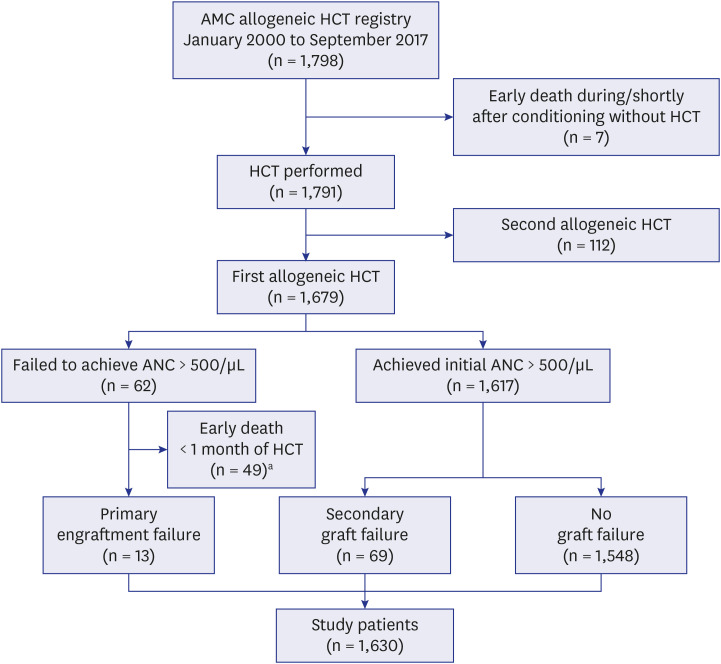
Fig. 1
Selection process of patients with graft failure.
AMC = Asan Medical Center, HCT = hematopoietic stem cell transplantation, ANC = absolute neutrophil count.
aForty-nine patients died within 1 month after HCT without achieving ANC greater than 1,000/μL. Causes of death in these patients were sepsis/organ failure (n = 23), progression of underlying malignancy (n = 23), cerebral hemorrhage (n = 2), and encephalopathy (n = 1).
![]()
Transplantation procedure
The conditioning regimen consisted of the myeloablative conditioning (MAC; busulfan-cyclophosphamide, busulfan-fludarabine) and the RIC (busulfan-fludarabine-antithymocyte globulin [ATG], cyclophosphamide-fludarabine-ATG). Graft-versus-host disease (GVHD) prophylaxis was uniformly performed with intravenous cyclosporin and 3 doses of intravenous methotrexate.
Patient monitoring
Dates with ANCs greater than 500/µL for 2 consecutive days and platelet counts greater than 20,000/µL for 7 consecutive days without transfusion were recorded. If both the ANC and platelet count were fulfilled as above, the patient's status was listed as either donor cell reconstitution or AR according to chimerism after recovery. Chimerism study measuring STR of peripheral blood (PB) sample DNA was routinely done after cellular recovery.
Statistical analysis
Outcomes included primary GF, secondary GF, donor cell reconstitution, AR, no cellular recovery, relapse, non-relapse mortality (NRM), and follow-up duration. The time to secondary GF, recurrence of underlying disease, and NRM were measured from HCT, estimated using the cumulative incidence function, and compared using the Gray method.17 The recurrence of underlying disease and NRM were considered as mutually competing risks. Event-free survival (EFS) was measured from HCT to recurrence, NRM, primary/secondary GF, or last follow-up. EFS and OS were estimated using the Kaplan-Meier method and compared using the log-rank test.18
To identify peri-transplant variables that might affect the HCT outcomes, univariate analysis performed with χ2 analysis. For multivariate analysis based on the Cox regression model, variables with a P value 0.05 or less, as determined by univariate analysis, were considered for entry in the model.19 The selection process was based on Gray's model for secondary GF, recurrence, and NRM. In addition, the incidence and clinical characteristics of AR after secondary GF was investigated. The cumulative incidence analysis was performed using R statistical software, version 3.3.1 (The CRAN project). For other analysis, SPSS software, version 21 (IBM Corp., Armonk, NY, USA) was used.
RESULTS
Patient characteristics
Median age was 43 years (range, 15–75), and the pretransplant diagnosis was as follows: acute myeloid leukemia (AML), 48.1%; acute lymphoblastic leukemia (ALL), 18.0%; CML, 3.9%; severe AA, 8.5%; myelodysplastic syndrome/myeloproliferative neoplasm (MPN), 13.9%; lymphoma/myeloma, 5.4%; and miscellaneous disorders, 2.3%. MAC was used in 37.2%, RIC was administered in 62.8%. Graft employed for HCT was bone marrow graft in 27.0%, and peripherally collected stem cell graft in 73.0%. The type of donor-recipient relationship consisted of matched sibling donors (39%), matched unrelated donors (35%), and haploidentical donors (26%). The patient and donor characteristics are summarized in Table 1.
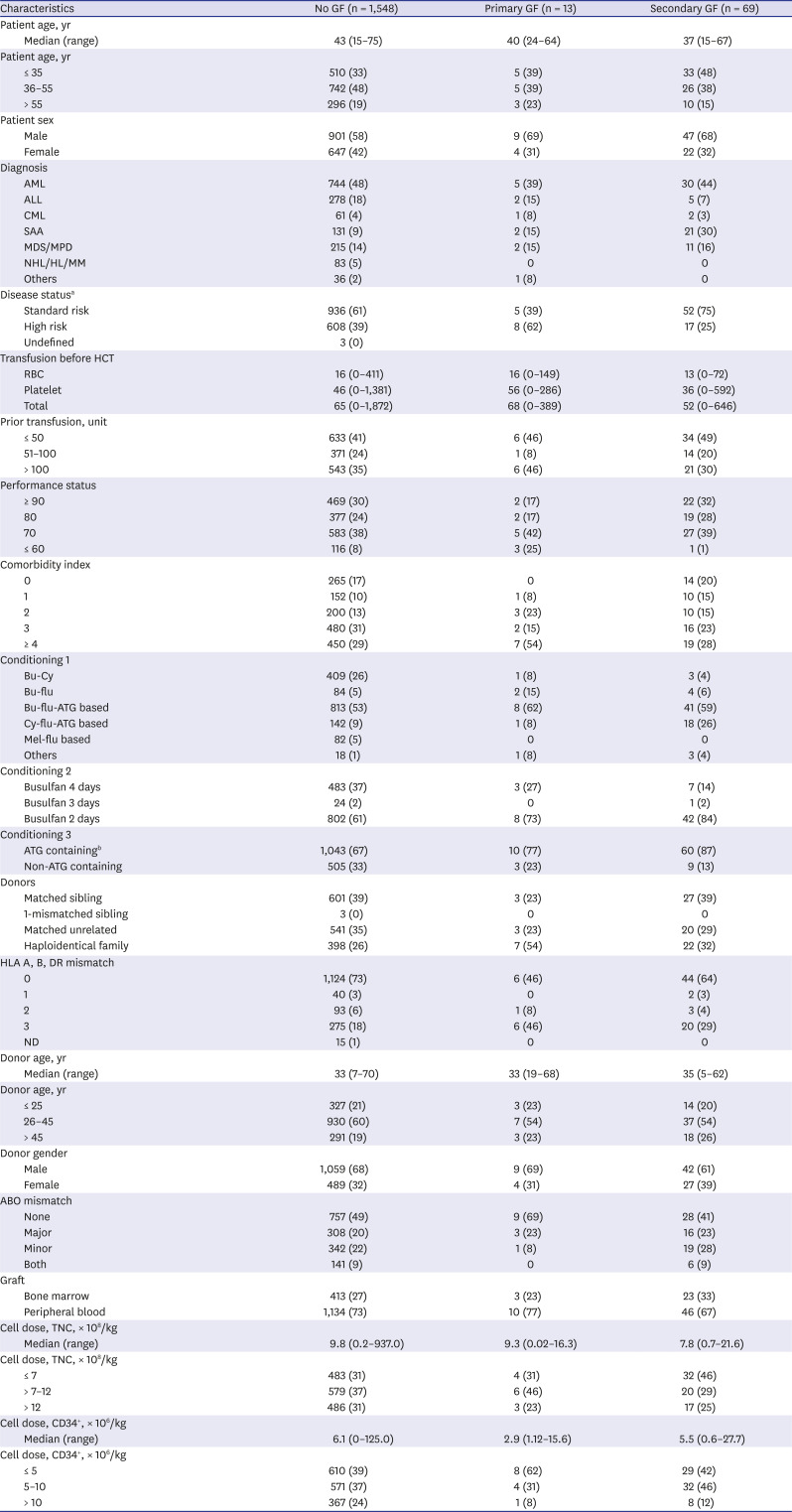
Table 1
Patient and donor characteristics (n = 1,630)
Values are presented as number (%).
GF = graft failure, AML = acute myeloid leukemia, ALL = acute lymphoblastic leukemia, CML = chronic myeloid leukemia, SAA = severe aplastic anemia, MDS = myelodysplastic syndrome, MPD = myeloproliferative disorder, NHL = non-Hodgkin lymphoma, HL = Hodgkin lymphoma, MM = multiple myeloma, HCT = hematopoietic stem cell transplantation, RBC = red blood cell, ATG = antithymocyte globulin, HLA = human leukocyte antigen, ND = not defined, TNC = total nucleated cell.
aHigh risk disease status is defined as follows: patients with acute leukemia in first remission by salvage chemotherapy, relapse or in second or subsequent remission, CML in accelerated or blastic phase, drug resistant or relapsed NHL/HD/MM or solid tumor, MDS (bone marrow blasts > 5% at transplant), and non-malignant hematologic disorder with active infection or bleeding; bOf 1,113 patients who received ATG, 1,041 received rabbit-ATG (thymoglobulin, genzyme) and 72 received horse-ATG (52 ATGAM, and 20 lymphoglobulin).
![]()
Graft failure
In 1,630 HCT recipients, the incidence of primary GF was 0.80% (n = 13), and the 10-year cumulative incidence of secondary GF was 4.5% (n = 69). The median follow-up duration after HCT in patients with successful initial engraftment, primary GF, and secondary GF was 31.2 months, 2.15 months, and 14.1 months, respectively.
Primary GF
Of 13 patients who experienced primary GF after HCT, the median age was 43 years, 84.6% were diagnosed with malignant disease, and 2 (15.4%) underwent HCT for severe AA. RIC was used in 69.2% and MAC was used in 30.8%. In univariate analysis, none of the pretransplant variables significantly predicted the occurrence of primary GF. However, the percentage of the following characteristics were prominently larger in the primary GF group than the control group: diagnosis of severe AA (15.4% vs. 8.5%), high risk status at time of HCT (61.5% vs. 39.3%), Karnofsky performance status of 60 or less (23.0% vs. 7.5%), comorbidity index of 4 or higher (53.8% vs. 30.3%), 3 HLA mismatch (46.2% vs. 17.8%), haploidentical HCT (53.8% vs. 25.7%), and CD34+ cell dose infused with 5 × 106/kg or less (61.5% vs. 39.4%). Multivariate analysis was impossible on account of statistical insignificance of univariate analysis.
The median survival after the onset of primary GF was 2.15 months (range, 0.1–14.0), and the mortality rate was 100%. Regardless of the type of treatment given, patients had persistent profound cytopenia and eventually died in a short period. The most common causes of death were progression (46.2%) and bacterial sepsis (38.5%). At the time of GF, 11 of 13 patients were in a range of 0–2% of donor chimerism, and the other 2 patients had 100% donor chimerism.
Cumulative incidence of secondary GF
A total 69 cases of secondary GF occurred with a 10-year cumulative incidence of 4.5% (95% confidence interval [CI], 3.5–5.7), which presented at a median of 3.0 months (range, 0.8–135.4) after HCT. The median patient age was 37 years, malignant disease and severe AA counted for 70% and 30% of cases, respectively, and high-risk status at HCT comprised only 25%. RIC regimen was administered in 85%.
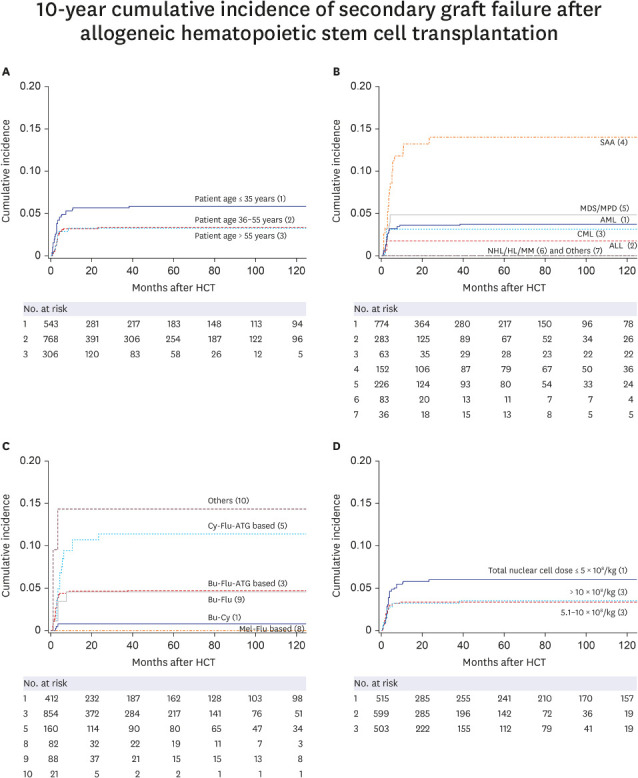
In univariate analysis (Supplementary Table 1), the 10-year cumulative incidence of secondary GF was higher in the following subgroups (Fig. 2): patients aged ≤ 35 years than those aged 36–55 years and older than 55 years (5.9% vs. 3.4% and 3.3%, P = 0.042), diagnosis of severe AA compared with malignant disease (14.0% vs. 1.8–4.9%, P < 0.001). Cy-Flu-ATG conditioning exhibited a significantly high cumulative incidence of secondary GF (11.4% vs. 0.7–5.8%, P < 0.001), which was intended for mostly transplantation for severe AA. MAC with 4 days administration of busulfan (3.2 mg/kg/day) showed a lower cumulative incidence of secondary GF than regimens containing 2 or 3 days (1.4% vs. 6.0% and 4.0%, P = 0.003). ATG administration was associated with higher cumulative incidence, which was mostly employed in RIC regimens (6.1% vs. 1.8%, P < 0.001). Lower doses of mononuclear cells (MNC) in graft (< 7 × 108/kg) were associated with higher cumulative incidence compared with the group that received 7–12 × 108/kg or more than 12 × 108/kg of MNCs (6.4% vs. 3.3% and 3.5%, P = 0.049). There was a trend toward a protective effect in patients received CD34+ cell more than 10 × 106/kg compared with patients who received CD34+ cells ≤ 5 × 106/kg, and 5–10 × 106/kg (2.2% vs. 4.9% and 5.3%, P = 0.052).
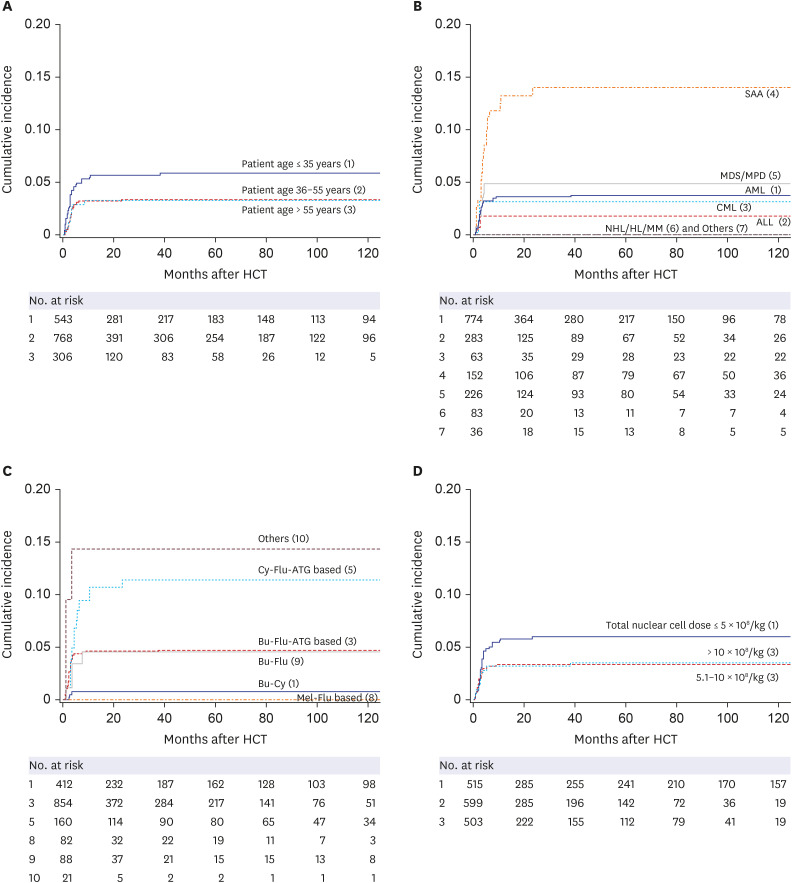
Fig. 2
Ten-year cumulative incidence of secondary graft failure. (A) Patient age group and cumulative incidence of secondary graft failure (P = 0.042). (B) Pretransplant diagnosis and cumulative incidence of secondary graft failure (P < 0.001). (C) Conditioning regimen and cumulative incidence of secondary graft failure (P < 0.001). Note that most of the Cy-flu-ATG recipients were diagnosed with severe aplastic anemia. (D) Total nuclear cell dose and cumulative incidence of secondary graft failure (P = 0.049).
HCT = hematopoietic stem cell transplantation, SAA = severe aplastic anemia, MDS = myelodysplastic syndrome, MPD = myeloproliferative disorder, AML = acute myeloid leukemia, CML = chronic myeloid leukemia, ALL = acute lymphoblastic leukemia, NHL = non-Hodgkin lymphoma, HL = Hodgkin lymphoma, MM = multiple myeloma, ATG = antithymocyte globulin.
![]()
In multivariate analysis (Table 2), RIC regimens (RR, 9.965–28.007), lower CD34+ cell dose (RR, 2.440-2.849, P = 0.021) were associated with higher cumulative incidence of secondary GF.
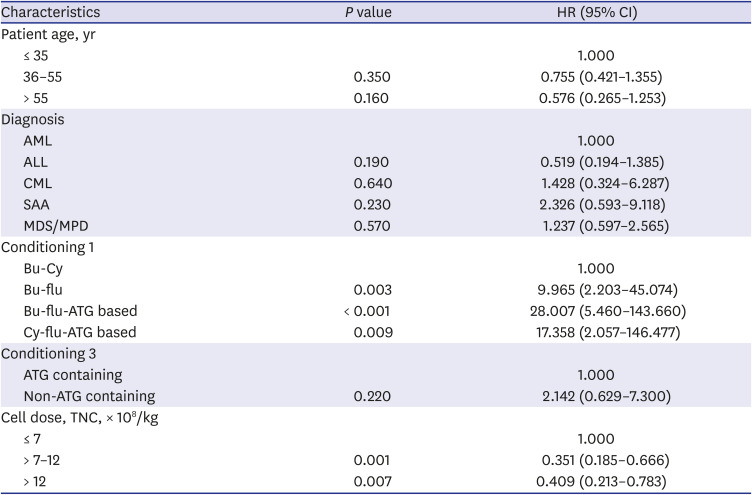
Table 2
Multivariate analysis of pretransplant risk factors in secondary graft failure
HR = hazard ratio, CI = confidence interval, AML = acute myeloid leukemia, ALL = acute lymphoblastic leukemia, CML = chronic myeloid leukemia, SAA = severe aplastic anemia, MDS = myelodysplastic syndrome, MPD = myeloproliferative disorder, ATG = antithymocyte globulin, TNC = total nucleated cell.
![]()
Outcomes of secondary GF
Among 69 secondary GF cases, 22 patients (31.9%) survived with cellular recovery and the remaining 47 patients (68.1%) had deceased. The median duration of follow-up for survivors was 63.8 months (range, 4.9–172.5), and the 5-year Kaplan-Meier survival rate was 28.8%. Chimerism study at the time of GF was 0% for donor in 77.6% of patients, and ≥ 10% in 22.4% of patients. The most common causes of death were bacterial sepsis in 29.4%, relapse/progression of underlying diseases in 16.2%, and GVHD in 7.4%. AR ensued in 8 patients (11.6%) after secondary GF. Donor reconstitution was divided into recovery with first HCT allograft (n = 4) and recovery with the second rescue HCT allograft (n = 8).
Management of secondary GF
As management of secondary GF, conservative care was given in 1.4%, support of growth factors in 31.8%, immunosuppression in 8.7%, mobilized donor leukocyte infusion (DLI) in 29.0%, and second HCT was conducted in 29.0%. The 5-year survival rate (5YSR) for patients receiving conservative care was 0%, support of growth factors was 18.2%, immunosuppression was 33.3%, mobilized DLI was 30.0%, and second HCT was 40.0%.
With administration of growth factors alone (n = 22), 18.2% of patients recovered with AR. Immunosuppression (n = 6) resulted in a 33.3% rate of donor reconstitution and mobilized DLI (n = 20) resulted in a 20% rate of AR and a 10% rate of donor reconstitution. In patients who received rescue HCT (n = 20) for secondary GF, 40% experienced donor reconstitution with a second HCT allograft. Regardless of the management given, 45.5–66.7% of patients (overall, 54.4%) did not recover from cytopenia and subsequently died. The relapse rate was highest (36.4%) in the granulocyte colony-stimulating factor (G-CSF) treatment group and was 0% to 10% in patients managed with immunosuppression, mobilized DLI, and second HCT. A summary of management and outcomes of secondary GF is provided in Table 3.

Table 3
Outcomes of secondary graft failure by types of management
Values are presented as number (%).
AR = autologous reconstitution, DLI = donor leukocyte infusion, HCT = hematopoietic stem cell transplantation.
![]()
Analysis of survival prognostic factors in patients with secondary GF
In the univariate analysis using the Kaplan-Meier survival rate, different type of management did not result in a significant difference in 5YSR. However, diagnosis of severe AA, and CML (45.7% and 50.0% vs. 0–28.9%, P = 0.049), low risk status at HCT (38.9% vs. 0%, P < 0.001), performance status ≥ 70 (19.5–41.4% vs. 0%, P < 0.001), RIC regimens (25.1–47.5% vs. 0%, P = 0.001), and ATG administration (33.2% vs. 0%, P < 0.001) was associated with significant survival benefit (Fig. 3). GF followed by MAC regimen exhibited a 5YSR of 0%.
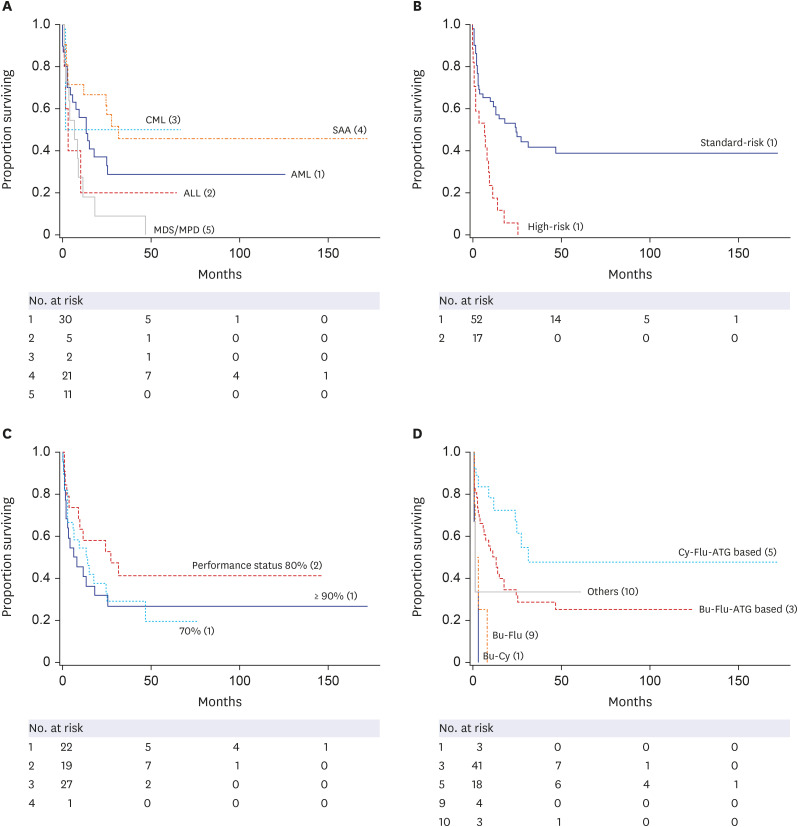
Fig. 3
K-M survival rate in secondary graft failure. (A) K-M survival rate in patients with severe aplastic anemia and malignant disease (P = 0.049). (B) K-M survival rate in patients with standard risk status compared with those in high-risk status at time of HCT (P < 0.001). (C) Performance status and K-M survival rate (P < 0.001). (D) K-M survival rate compared between conditioning regimens. Patients experienced secondary graft failure after myeloablative conditioning regimen had shorter survival (P = 0.001).
CML = chronic myeloid leukemia, SAA = severe aplastic anemia, AML = acute myeloid leukemia, ALL = acute lymphoblastic leukemia, MDS = myelodysplastic syndrome, MPD = myeloproliferative disorder, ATG = antithymocyte globulin, K-M = Kaplan-Meier.
![]()
In multivariate analysis, a lower Karnofsky performance score negatively influenced the 5YSR: score of 80 (odds ratio [OR], 0.119; 95% CI, 0.031–0.465; P = 0.002) and 70 (OR, 0.268; 95% CI, 0.088–0.821; P = 0.021). A full list of univariate and multivariate analysis of Kaplan-Meier 5YSR in secondary GF group is provided in Supplementary Tables 2 and 3.
Autologous reconstitution after secondary GF
In eighteen years of period, a total of 8 cases of AR occurred after secondary GF (Table 4). The incidence of AR was 0.49% of the overall study population (n = 1,630) and 11.6% among patients with secondary GF (n = 69). The median onset of AR was 7.0 months (range, 2.3–16.7) after onset of secondary GF. The median age in the AR group was 25 years (range, 17–60). Five patients (62.5%) never experienced profound neutropenia with their nadir ANC ≥ 500/µL. Five had a diagnosis of malignancy (4 AML, 1 ALL), 3 patients underwent HCT for severe AA. All 8 cases were of standard risk status at time of HCT. The entire group received an ATG containing RIC. Five patients received a graft from a full-matched donor and 3 underwent haploidentical HCT.
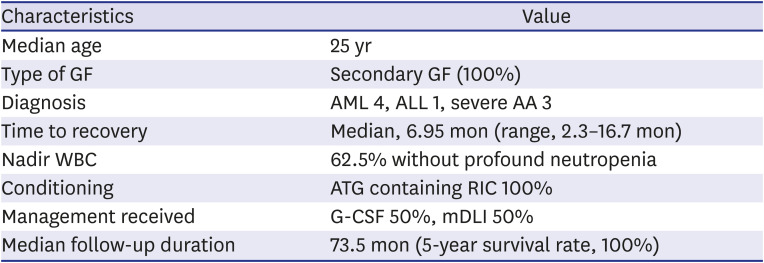
Table 4
Characteristics of 8 patients with autologous reconstitution
GF = graft failure, AML = acute myeloid leukemia, ALL = acute lymphoblastic leukemia, AA = aplastic anemia, WBC = white blood cell, ATG = antithymocyte globulin, RIC = reduced intensity conditioning, G-CSF = granulocyte colony-stimulating factor, mDLI = mobilized donor lymphocyte infusion.
![]()
Four patients were treated with growth factors only, and the remaining patients received mobilized DLIs. At the time of recovery from cytopenia, all cases had donor chimerism less than 10%. All patients who achieved AR were surviving at a median follow-up from secondary GF of 73.5 months (range, 38.5–170). Univariate analysis of pretransplant variables using the Gray method did not identify a significant predictive variable.
DISCUSSION
In this retrospective cohort study consisting of 1,630 allogenic HCT recipients, the incidence of primary and secondary GF (10-year cumulative incidence) was 0.80% and 4.5%, respectively. RIC usage in 62% of recipients, which is larger than previous studies RIC comprised of 31–43%, reflects relatively higher percentage of haploidentical HCTs.12 Compared with incidence of primary GF reported in CIBMTR study of 5.5%, incidence of primary GF in this study 0.8% is significantly low.4 More employment of PB graft (73.0% vs. 38.7%), G-CSF support (100% vs. 38.2%), and higher TNC counts in this study compared with CIBMTR registry, seem to have contributed to discrepancy in incidence of primary GF. Moreover, PB graft is known to have higher engraftment rate, thought as a result of higher T-cell component and TNC counts. The insufficient statistic power in univariate analysis for predictors of primary GF is thought to be partly due to the small number of primary GF (n = 13). The mortality rate in primary GF was 100%, with 1-year survival of 7.7% was considerably worse outcome compared with previous studies that reported 1-year survival as 11–45%.520 This finding is speculated as a result of profound neutropenia and a high proportion of poor risk status at time of HCT.
Higher 10-year cumulative incidence of secondary GF was associated with age ≤ 35 years, diagnosis of AA, RIC regimen, and low MNC count. On the contrary, MAC regimen and high CD34 count appeared to be protective of secondary GF. These findings are in concordance with previous studies. However, in the setting of GF, RIC regimen was associated with better survival, compared with 0% of 5YSR in GF after MAC. In addition, in the survival analysis of EFS and OS in the whole cohort, RIC had better outcomes compared with MAC. Therefore, it is erroneous to conclude that the outcomes of RIC regimen are inferior to myeloablative regimen, which is in line with previous studies.1521
The rate of cellular recovery was better in patients managed with mobilized DLI or rescue allogeneic HCT than conservative care. However, this interpretation should be cautious, because a considerable number of patients probably had no choice but to receive growth factor due to their comorbidities. As a salvage therapy for GF, Harada et al.22 reported outcomes of salvage haploidentical HCT was associated with better ANC recovery and lower NRM compared with cord blood graft HCT. Rudakova et al.23 reported a 48% response and prolonged survival with thrombopoietin agonists in GF after HCT.
Interpretation of data in patients experienced AR is limited due to very small numbers. These patients had common advantageous host factors, such as young median age, moderate neutropenia and favorable risk status at time of HCT. It appears that these host factors allowed the patients to avoid death due to severe infection. In a previous study reporting 45 AR cases in 1,205 severe AA patients, AR cases had better long-term OS than even patients with successful engraftment.5 This is also concordant with our study. A nationwide registry review in Japan consisting 42 survivors experienced AR with residual chromosomal abnormalities described late relapse of underlying malignancy in minority of patients.24
There are several notable limitations in this study. First, this is a retrospective study conducted in a single referral center. Second, there was heterogeneity in diagnosis of HCT recipients including severe AA, MPN, lymphoma, and multiple myeloma, which have different nature of prognosis and outcome after allogeneic HCTs compared with acute leukemia. Third, a significant portion (26%) of recipients underwent HLA-haploidentical transplants, which has a slightly different pattern of outcomes of HCTs from matched transplantations. Lastly, decisions of type of treatment for graft failure (e.g., G-CSF support only vs. second transplantation) were based on individual clinical scenario and judgement, we could not clarify the standard criteria for selection of salvage therapy.
In the absence of established guidelines, management of patients with GF presents a predicament, and GF is associated with poor prognosis. Nevertheless, aggressive management such as mobilized DLI and rescue second HCT resulted in the most favorable outcome. AR may be expected in a small number of younger patients without severe cytopenia in the setting of secondary graft failure. Because the incidence of GF is not very prevalent and heterogeneity of management differs between centers exists, a multicenter study with a controlled treatment arm is necessary in the future.
 XML Download
XML Download