

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Classic fever of unknown origin (FUO) represents a diagnostically challenging, febrile condition in otherwise healthy, immune-competent patients in whom the cause of fever remains unidentifiable following intensive diagnostic work-up.1 Inflammation of unknown origin (IUO) is a group of inflammatory conditions that has similar underlying causes to FUO, but manifests with different clinical presentations such as the absence of fever > 100.9°F (38.3°C).2 The diagnostic criteria of FUO have evolved by incorporating advances in diagnostic technologies and adapting the availability of such new testing modalities in outpatient settings.1 The accessibility of these new tests has also altered the spectrum of causes of FUO, which has made diagnosis even more challenging. For example, the prevalence of the three classic causes of FUO, malignancies, infections, and non-infectious inflammatory diseases (NIIDs), varies by geographic location,1 and many undiagnosed cases have been observed in countries with more diagnostic resources.3
Planar images and single photon emission computed tomography scans using gallium-67-citrate (Ga-SPECT), and positron emission tomography using fluorine-18-fluorodeoxy glucose, combined with computed tomography (FDG-PET/CT), are nuclear imaging tests that use tracers accumulate in the tumor or inflammatory cells. These imaging tests represent the advances in diagnostic technologies that have the ability to wide screen to localize the foci of fever or inflammation. Over the last few decades, several small primary studies and meta-analyses found that FDG-PET/CT correctly localized the foci of FUO in approximately 60% of patients.45 This was subsequently validated in two large studies that included patients with either FUO or IUO, one prospective study from Germany (240 patients)6 and one retrospective study from China (376 patients).7 Furthermore, a recent prospective, paired-design study has shown that FDG-PET/CT is more sensitive than Ga-SPECT in identifying the foci of FUO.8 On this basis, expert consensus now recommends FDG-PET/CT as the modality of choice when diagnostic clues are absent in the work-up.591011 However, previous studies have inconsistently reported patient characteristics that were associated with successful localization of FUO/IUO foci by FDG-PET/CT.4561213141516 Therefore, whether clinicians can tailor the application of FDG-PET/CT to individuals with particular characteristics is uncertain. Furthermore, prognosis of unexplained FUO/IUO patients after an unsuccessful work-up with FDG-PET/CT has not been well described.17
To address these uncertainties, the current study focused on the following two points. First, we assessed the characteristics associated with successful identification of foci of FUO/IUO by FDG-PET/CT in the context of diagnostically challenging cases. Second, we assessed whether a negative FDG-PET/CT scan result was associated with spontaneous remission in patients where the etiology of FUO or IUO was unidentifiable despite intensive work-up, including FDG-PET/CT.
METHODS
Eligibility criteria of FUO and IUO
We included all patients with classic FUO or IUO who required an FDG-PET/CT scan as an additional test after an unsuccessful diagnostic work-up, including whole-body CT, between April 1, 2013, and December 31, 2019. Both outpatients and hospitalized patients were included. The inclusion was not consecutive, because similar patients who underwent Ga-SPECT/CT and were not assessed with FDG-PET/CT were excluded.18 We defined FUO as (a) body temperature of ≥ 38.3°C (101°F) on at least two occasions, (b) ≥ 3-week duration of illness, and (c) failure to identify the etiology after 3 visits to the outpatient clinic or a 3-day inpatient investigation.19 For patients not satisfying the first febrile criterion, a C-reactive protein (CRP) > 7 mg/L or an erythrocyte sedimentation rate (ESR) > age/2 in men or (age + 10)/2 in women was required to satisfy the definition of IUO.620 None of the eligible patients were infected with human immunodeficiency virus, neutropenic, or already hospitalized for other pre-existing illness. However, we included the patients who received low-dose corticosteroids (< 5 mg of prednisone daily or equivalent doses) for autoimmune disorders or had a history of malignancy.
Pre-FDG-PET/CT diagnostic work-up
According to a recent expert opinion,1 we operationally defined obligatory investigations in the first-stage of diagnostic work-up as follows: thorough history-taking and physical examination, ESR or CRP, hemoglobin (Hb) concentration, platelet count, white blood cell (WBC) count with differentiation, electrolytes, creatinine, total protein, alkaline phosphatase, aspartate aminotransferase, alanine aminotransferase, lactate dehydrogenase, creatine phosphokinase, antinuclear antibodies, rheumatoid factor, protein electrophoresis, urinalysis, blood cultures, urine culture, chest X-ray, abdominal ultrasonography, and interferon-γ release assay (T-SPOT.TB.; Oxford Immunotec, Oxford, UK). Other specific tests were performed individually if they were indicated through the clinical presentations and/or physical examinations.
FDG-PET/CT
PET/CT images were obtained through Biograph mCT TrueV (Siemens Healthineers, Erlangen, Germany) and uMI 510 (Shanghai United Imaging Healthcare, Shanghai, China) according to the existing procedure guidelines, before and after May 1, 2017, respectively.212223 After measurement of fasting blood glucose, 3.7 MBq/kg of FDG was administered, and PET imaging was performed after 60 minutes. If necessary, delayed imaging was additionally obtained at 120 minutes. Image reconstruction was performed using three-dimensional ordered subset expectation maximization, point-spread function, and time-of-flight correction methods, and attenuation correction was achieved based on the low-dose CT images that were obtained concurrently.
At least one board-certified nuclear medicine specialist interpreted the imaging visually and semi-quantitatively using the maximum standardized uptake values (SUVmax) within the region of interest. The interpreters were informed of all clinical information and were unaware of the final diagnosis. Positive findings were defined as focal or diffuse area(s) of increased activity that were not explained by physiological uptakes. No cutoff values for the SUVmax were specified a priori.
Diagnosis of the etiology of FUO or IUO
All diagnostic and therapeutic interventions were performed in the presence of the FDG-PET/CT findings at the discretion of the treating physicians. Typically, biopsy and histological assessment was performed for positive PET/CT findings suggestive of malignancy. Clinical diagnosis was established in the case of suspected NIIDs. Local pathologists made the histopathological diagnosis in view of all clinical information, including the PET/CT findings.
Data extraction
A single investigator (AW) searched the institutional imaging repository to identify potential eligible patients. Eligible patients were selected from all FDG-PET/CT scans that physicians from the General Internal Medicine department ordered for any test objectives; we did not employ electronic code searches of the hospital databases based on the International Classification of Diseases diagnosis codes to identify the eligible patients. Another investigator (ST), who was blinded to the PET/CT reports, extracted the following data from the medical records: demographics, history, symptoms, vital signs, and physical examination results; results for the aforementioned obligatory and other investigations; radiology reports of body CT, FDG-PET/CT, and other imaging studies, if any; and the final diagnosis. For each patient, the same investigator verified the final diagnosis with other clinical information available from the medical records, such as microbiology and pathology reports. The investigator then extracted data from the PET/CT reports. No disease codes, including the International Classification of Diseases, were used to determine the final diagnosis.
Outcomes
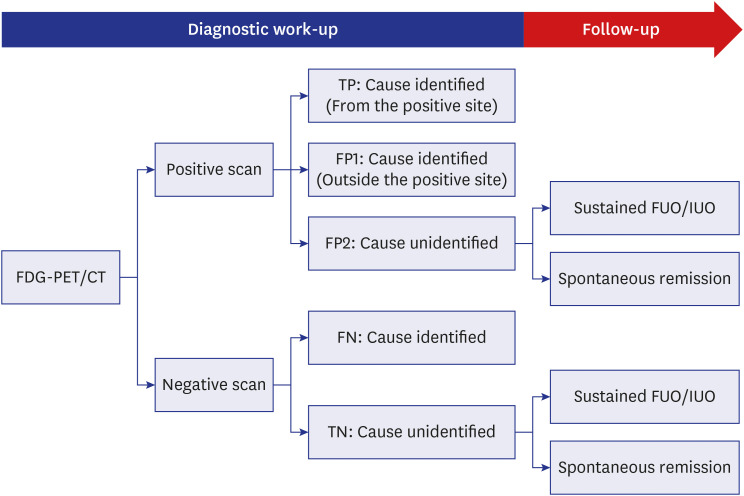
Recognizing that patients with sustained symptomatic, undiagnosed FUO or IUO are conventionally regarded as “no target condition,” although theoretically no true cases of “no target condition” exist,45 we operationally defined a modified cross-classification system comprising five groups as shown in Fig. 1 (true positive [TP]; false positive [FP], comprising FP1 and FP2; false negative [FN]; and true negative [TN] cases) based on whether the PET/CT was positive or negative, as well as whether a specific etiology of FUO or IUO was identified or not (i.e., sustained symptomatic, undiagnosed FUO, or IUO). When an FUO or IUO etiology was identified for a case with a positive PET/CT scan, we explicitly classified TP vs. FP1 based on whether the identified lesion was within vs. outside the PET/CT positive site(s), respectively.
Our primary outcome of interest was successful localization of FUO/IUO foci. We used diagnostic yield as a measure of successful localization, which was conventionally defined as the proportion of patients categorized as TP to the total number of tested patients45:
Symptoms of FUO or IUO can remit spontaneously in patients with sustained symptomatic, undiagnosed FUO, or IUO with variable frequencies.24 Therefore, a negative PET/CT can be beneficial in such patients by avoiding unnecessary invasive diagnostic procedures.25 Our secondary outcome was overall clinical helpfulness to take additional account of this beneficial aspect. We calculated the proportion of patients categorized as TP and those categorized as TN, whose symptoms spontaneously remitted only to the total number of tested patients:
Statistical analyses
All statistical analyses were performed using Stata SE, version 15.1 (StataCorp, College Station, TX, USA). The P values for all analyses were two-tailed, and were considered statistically significant if they were < 0.05. Because this study was based on convenience sampling, no formal sample size calculation was performed. We descriptively analyzed all variables as means and standard deviations or medians and interquartile ranges (IQRs) depending on the distribution of the variables, or as numbers and percentages. We estimated the 95% confidence intervals (CIs) of proportions using the standard exact method. Because of the limited number of observations, we only qualitatively assessed the differences in clinical characteristics and outcomes between patients with FUO and those with IUO, and did not perform formal statistical comparisons.
We performed multivariable logistic regression using fractional polynomials to model non-linear relations with continuous variables in order to assess the predictive ability of previously reported patient characteristics that were associated with an improved diagnostic yield of FDG-PET/CT.26 As recommended, we a priori included all candidate clinical variables in the model,27 and missing values were imputed by multiple imputation by chained equations (Supplementary Data 1).28 We selected age, sex, duration of symptoms, temperature, serum concentrations of CRP, WBC, ESR, and Hb as the candidate predictors.61213141516 We post hoc selected serum concentrations of soluble interleukin-2 receptor as an additional variable. Although we planned to include two physical examination findings (lymphadenopathy and abnormal cutaneous findings) as candidate predictors before analysis, we post hoc excluded these values due to few observations causing complete separation. We fitted the fractional polynomial logistic regression based on the likelihood-ratio type tests and Wald type tests; since both generated congruent results, we only reported the results based on the Wald type tests.
Regarding long-term prognosis of unsuccessful diagnosis, we assessed whether a negative FDG-PET/CT scan result was associated with more spontaneous remissions in patients whose etiological diagnosis was unsuccessful despite intensive work-up, including FDG-PET/CT. We calculated the survival probabilities using the Kaplan–Meier method, and between-group comparisons were performed using the log-rank test. We did not perform multivariable analysis using the Cox regression due to the small sample size and limited outcome events.
Ethics statement
This observational study was based on retrospective chart reviews and was conducted at Fujita Health University Hospital, a 1,435-bed tertiary referral hospital in Japan. The Institutional Review Board of Fujita Health University approved this study and waived the requirement for informed consent (approval No. HM17-460).
RESULTS
Participants
A total of 50 patients (35 with FUO and 15 with IUO) who underwent FDG-PET/CT as an additional triage test were included. Table 1 shows the characteristics of the included patients. The median age was 71 years (IQR, 61‒77 years). Nine patients (18%) had diabetes, and three had underlying autoimmune disorders and were on maintenance treatment of oral prednisolone (< 5 mg/day). Six patients had a history of cancer. Most patients (40/50, 80%) underwent FDG-PET/CT within 3 months of the symptom onset. Compared to patients with FUO, the patients with IUO were older (median age, 68 [FUO] vs. 75 years [IUO]), had longer symptomatic durations (median duration, 43 [FUO] vs. 68 days [IUO]), and had lower concentrations of CRP (median CRP concentration, 13.5 [FUO] vs. 5.3 mg/dL [IUO]).
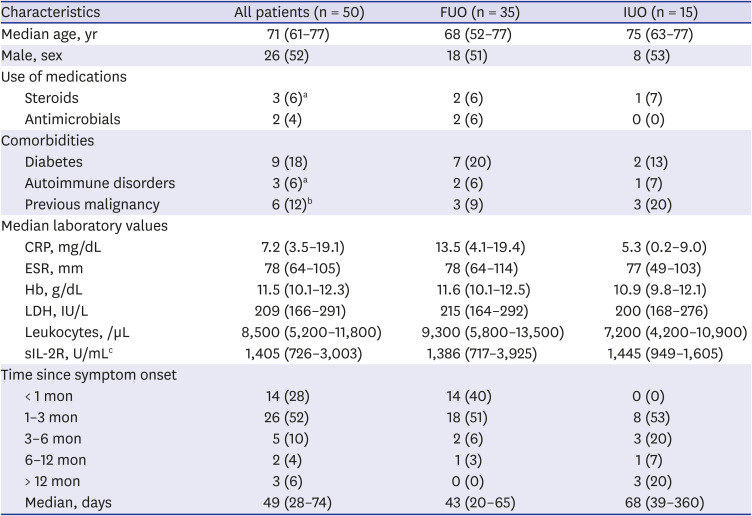
Table 1
Patient characteristics
Values are presented as median (interquartile range) or number (%).
FUO = fever of unknown origin, IUO = inflammation of unknown origin, CRP = C-reactive protein, ESR = erythrocyte sedimentation rate, Hb = hemoglobin, LDH = lactate dehydrogenase, sIL-2R = soluble interleukin-2 receptor.
aOne each patient with FUO who had idiopathic thrombocytopenic purpura and rheumatoid arthritis, respectively, and another with IUO who had polymyalgia rheumatica were treated with a maintenance dose of prednisolone at < 5 mg daily; bTwo patients with breast cancer and one each with esophageal cancer, thyroid cancer, rectal cancer, and colon cancer; cBased on a total of 38 patients (28 FUO patients and 10 IUO patients).
![]()
Pre-FDG-PET/CT diagnostic work-up
Although the majority of the obligatory investigations were performed in each patient, only 21 patients (42%) completed all the investigation items (Supplementary Table 1). All patients underwent non-enhanced thoracico-abdomino-pelvic CT. Completion rates were low with regards to rheumatoid factor (36/50, 72%) and urine culture (28/50, 56%). No specific diagnostic clues were recorded from the physical examinations, with the exception of lymphadenopathy (three patients with FUO) and abnormal cutaneous findings (one patient with FUO). Seven patients (four with FUO and three with IUO) underwent FDG-PET/CT as second-line nuclear imaging after an unsuccessful localization by Ga-SPECT/CT.
Reference standards
Pathological explorations were performed in 20 (40%) patients, and the proportions of pathological assessment were similar for patients with FUO (14/35, 40%) and IUO (6/15, 40%) (Supplementary Table 2). Pathological assessment led to etiologic diagnosis in a total of 19 out of 37 patients (53%) in whom a cause was successfully identified. Pathological exploration only failed in one patient, and in the remaining 18 successfully diagnosed patients, diagnosis relied on the PET/CT findings in 11 patients (61%), 9 with NIIDs and 2 with malignancy (Supplementary Table 2).
Successful localization
Of 50 eligible patients, other than one case with infection (aseptic meningitis), all identified etiologies were either malignancy or NIIDs (each category with 18 patients, 36%) (Table 2). No cause was identified in 13 patients (26%; patients with IUO [7/15, 47%] and FUO [6/35, 17%]). No recurrent cancer was identified as the cause of FUO/IUO in the six patients with a history of cancer, whereas disease flare was clinically diagnosed as the cause of FUO/IUO in two of the three patients who had received maintenance corticosteroid therapy (one with polymyalgia rheumatica and another with rheumatoid arthritis).
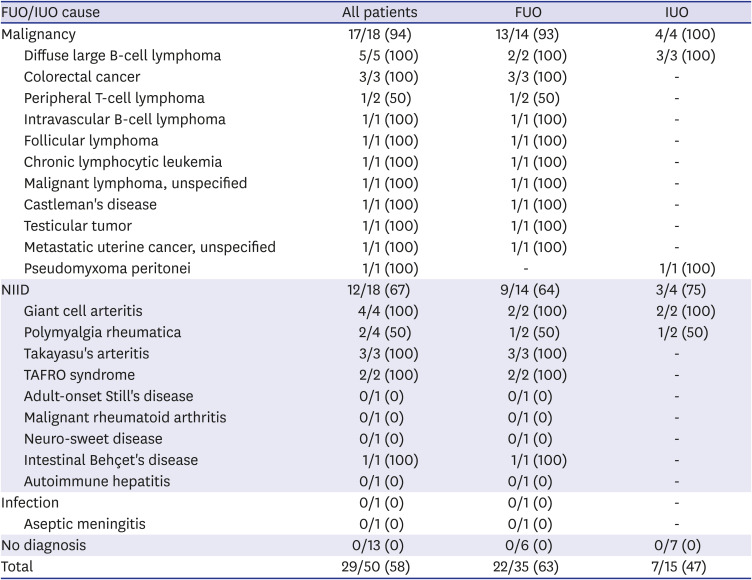
Table 2
Final diagnosis and diagnostic yield of patients with FUO or IUO
Values are presented as number (%).
FUO = fever of unknown origin; IUO = inflammation of unknown origin; NIID = non-infectious inflammatory disease; TAFRO = thrombocytopenia, anasarca, fever, reticulin fibrosis, renal dysfunction, and organomegaly.
![]()
FDG-PET/CT correctly localized the foci of FUO or IUO in 29 patients (diagnostic yield, 58% [29/50]; 95% CI, 43–72%). The diagnostic yield was similar for the subgroups of patients with FUO (diagnostic yield, 63%; 95% CI, 45–79%) and IUO (diagnostic yield, 47%; 95% CI, 21–73%). FDG-PET/CT was useful for identifying both malignancy and NIIDs, whereby the cause was successfully localized in 17 of the 18 patients with malignancy (94%) and in 12 of the 18 patients with NIID (67%) (Table 2). FDG-PET/CT failed to localize a focus in a total of eight patients: two with polymyalgia rheumatica and one patient each with peripheral T-cell lymphoma, adult-onset Still's disease, malignant rheumatoid arthritis, neuro-Sweet disease, autoimmune hepatitis, and aseptic meningitis.
Predictors of successful localization
None of the selected clinical characteristics were significantly associated with a higher or lower diagnostic yield of FDG-PET/CT for localizing the foci of FUO or IUO (Table 3). The results in the sensitivity analysis, restricted to 38 patients without missing data, were congruent.
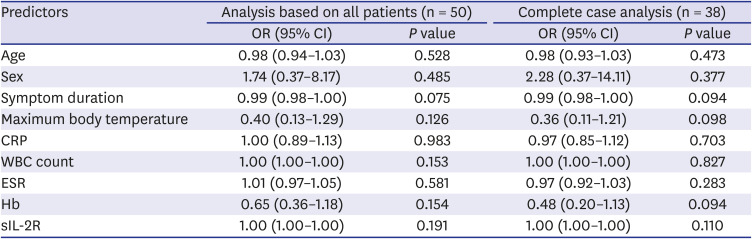
Table 3
Association between clinical variables and diagnostic yield of FDG-PET/CT in patients with FUO or IUO
FDG = fluorodeoxyglucose; PET = positron emission tomography; CT = computed tomography; FUO = fever of unknown origin; IUO = inflammation of unknown origin; OR = odds ratio; CI = confidence interval, CRP = C-reactive protein; WBC = white blood cell, ESR = erythrocyte sedimentation rate; Hb = hemoglobin; sIL-2R = soluble interleukin-2 receptor.
![]()
Spontaneous remission and overall clinical helpfulness
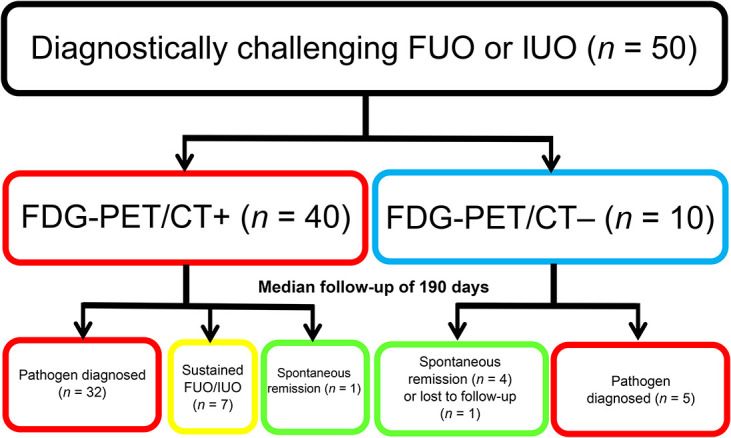
In total, 10 of the 50 patients died from the cause of FUO or IUO, with a median follow-up of 243 (IQR, 111–613) days (Fig. 2). None of the 13 patients whose FUO or IUO cause remained unexplained after FDG-PET/CT died during the follow-up. Similarly, all 10 patients with a negative FDG-PET/CT result were still alive during follow-up. Of the 13 patients with unexplained FUO or IUO, patients with a negative FDG-PET/CT had a significantly higher chance of spontaneous remission than those with a positive FDG-PET/CT with a median follow-up of 190 days (80% [4/5] in patients with a negative result vs. 13% [1/8] with a positive result; log-rank *P = 0.018).
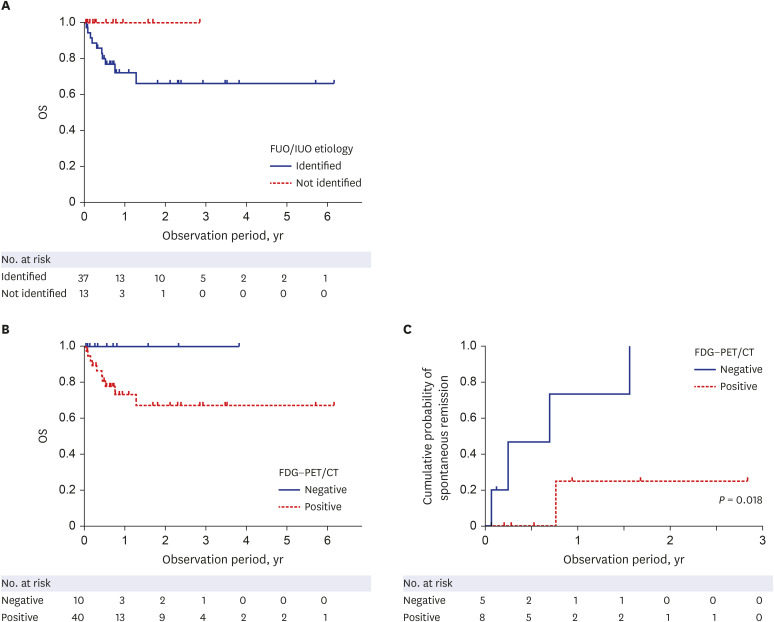
Fig. 2
Prognosis of patients with FUO or IUO assessed by FDG-PET/CT. Kaplan-Meier plots showing the overall survival of all 50 patients by FUO or IUO etiology (A), positivity of FDG-PET/CT (B), and cumulative probability of spontaneous remission of symptoms by positivity of FDG-PET/CT (C).
OS = overall survival, FUO = fever of unknown origin, IUO = inflammation of unknown origin, FDG = fluorodeoxyglucose, PET = positron emission tomograph, CT = computed tomography.
![]()
In addition to successful localizations, when patients with negative PET/CT findings, whose symptoms regressed spontaneously during follow-up, were additionally counted as favorable events, FDG-PET/CT was deemed clinically helpful in 33 patients (overall clinical helpfulness, 66% [33/50]; 95% CI, 51–79%). The results were similar for patients with FUO (overall clinical helpfulness, 69%; 95% CI, 50–83%) and IUO (overall clinical helpfulness, 60%; 95% CI, 32–84%).
DISCUSSION
This retrospective, single-center study, in a tertiary university hospital, validated the clinical usefulness of FDG-PET/CT in 50 patients with diagnostically challenging FUO or IUO after a standard diagnostic work-up. FDG-PET/CT had a diagnostic yield of 58% for localizing the cause of FUO or IUO, which was congruent to the results of previous studies.46 The overall clinical helpfulness increased to 66% when patients with a negative FDG-PET/CT result and whose symptoms remitted spontaneously were additionally considered as favorable events. However, the proposed clinical variables were not significantly associated with successful localization of the cause in our cohort. Patients in whom the cause could not be identified despite FDG-PET/CT scanning generally had a good prognosis, and spontaneous remission appeared common in those with a negative scan.
First, the follow-up for patients with sustained unexplained causes in our cohort, particularly those who underwent PET/CT in the later study period, was short, which could bias the results. Second, although we restricted the number of candidate predictors to nine (eight previously proposed and another post hoc added variable), our sample size (50 patients, with 29 successful and 21 failure events) may lack an adequate power to validate nine variables.2729 Third, although FDG-PET/CT successfully localized the FUO/IUO foci in the few patients who presented with two potentially important predictors (lymphadenopathy and skin lesions),1215 we excluded these variables due to perfect separation. However, inclusion of such rarely observed characteristics is discouraged.27 In light of these limitations, the finding that previously proposed characteristics were not predictive should be interpreted with care.
The prevalence of infections identified in the reported studies of FDG-PET/CT for FUO or IUO from East Asia ranges between 27% and 63%, while the prevalence of miscellaneous causes is reportedly up to 7%.7133031323334 In our present cohort, we only identified a single case of non-malignant or -NIID cause (2%), which is considerably lower than has been previously reported. Our cohort comprised patients who already underwent an extensive work-up, and patients with common or easily identifiable causes were excluded. Typically, common causes such as bacterial infections are ruled out early in such aggressive work-up, including whole-body CT and microbiological evaluations. Alternatively, such patients may have already been excluded before referral; indeed, infection causes are rare in tertiary care university hospital settings in Japan.35 Therefore, despite the limitations in study methodologies, our results may be reasonably applicable to such referral settings where common FUO or IUO causes are already excluded.
In conclusion, FDG-PET/CT appears to be useful to localize the foci of FUO or IUO, even in diagnostically challenging cases referred to tertiary academic hospitals. In this setting, evidence is inconclusive as to whether patients with specific variables are associated with successful localization. Our limited observation suggests that negative FDG-PET/CT may be prognostic for spontaneous remission in patients with unexplained FUO or IUO. Given the high cost of FDG-PET/CT, future research is required to identify reliable predictors to help develop risk-oriented diagnostic algorithms. Such predictors should ideally be jointly established as a clinical prediction model in studies with a large sample size.
 XML Download
XML Download