

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The number of confirmed cases surged not only in the early stages of the coronavirus disease 2019 (COVID-19) epidemic, but throughout the summer and the winter of 2020 in South Korea.1 To respond to the pandemic, the Korean government has enhanced social distancing,2 developed a COVID-19 confirmed case management framework, and strengthened the pandemic supply chain, such as personal protective equipment, testing supplies, medical equipment, and hospital beds.3 The government also installed residential treatment centers (RTC)4 and dedicated hospitals for infectious disease response to secure sickbeds.56 In addition, various other efforts, such as forming a team for joint response to COVID-19 in metropolitan area6 and cooperating with private medical institutions, have been made.78910
Despite these efforts, the government was unable to fully contain the spread of COVID-19 and avoid the situation of the number of confirmed patients exceeding the supply of hospital beds. Especially in March of 2020, Daegu experienced a complete depletion of ‘intensive care units (ICUs)’ and ‘negative pressure isolation rooms’ due to mass infection.11 Dozens to hundreds of confirmed cases had to wait for hospitalization for at least a day, and unfortunately, some died while waiting.1213 This experience has highlighted the need to re-establish the framework of treatment by rethinking the classification system of patients during a pandemic. In addition, the experience in Daegu has brought on discussions about the need to develop a safe and effective management of COVID-19 patients in their own homes until hospitalization becomes available.14
Many countries have already been recommending self-isolation to confirmed COVID-19 patients.15161718 The US Centers for Disease Control and Prevention (CDC) recommends confirmed patients to stay home and ‘watch for warning signs,’ and ‘follow self-check protocols.’ European Centers for Disease Control and Prevention (ECDC) also suggests self-isolation to the confirmed cases with mild symptoms of COVID-19,19 and the World Health Organization also recommends self-isolation for those under the age of 60 without underlying diseases and symptoms.20
In Korea, however, there were no such guidelines until the Korean disease control authorities introduced the term, ‘self-treatment.’ The term, ‘self-isolation,’ in Korea is primarily used for suspected patients to undergo self-quarantine, and to distinguish suspected patients from confirmed patients, the Korean government used the term, ‘self-treatment,’ to refer to self-isolation of confirmed patients. For this reason, a populous self-governing province in Korea, known as Gyeonggi-do, has developed a home management system (HMS)21 to minimize the risk while the confirmed patients await their hospitalization and to date, HMS has been operating effectively. Therefore, this paper proposes the experience of one local government in South Korea on how it coped with and managed the shortage of supplies via HMS.
Since the third surge of COVID-19 in South Korea, self-treatment was introduced by the national government as the Infectious Disease Control and Prevention Act was amended.22 However, as the initial target of self-treatment is limited by pediatric patients or their parents with clinically good status,23 the government is under a consideration of expanding the target range to all patients. Self-treatment is suggested as one of the appropriate healthcare measures during a pandemic;24 however, despite good measures, the risk of rapid deterioration of patient condition remains high.11 To prevent any dangerous situations, the national government should establish a protocol that allows safe self-treatment at home. In Korea, the concept of self-treatment is just beginning; and thus, the government can use this opportunity to construct a new innovative protocol. Therefore, to assist the government in the newly adopted self-treatment policy, this paper proposes a novel HMS. Furthermore, the paper also proposes some recommendations for other countries in similar situation.
DEVELOPMENT OF HMS
Goal and objectives
The goal of HMS is to supplement the government's COVID-19 confirmed case management system by managing patients waiting for hospitalization due to lack of hospital and RTC beds, so that the system can not only respond to but withstand the pressures of a further and rapid increase in the number of confirmed cases.
The objectives of HMS are as follows: 1) to reduce the workload and burden on the local governments in responding to COVID-19 (i.e., public healthcare centers are the frontline responders in combating infectious diseases in Korea, 2) to prevent emergency situations (e.g., sudden change of severity, psychiatric change, trauma, a refusal of the isolation, and escape etc.) that may occur while awaiting hospitalization at home by continuously monitoring patient's severity and conditions, as well as supporting the medical and psychological needs of patients through counseling services.
Target patients
Confirmed patients awaiting hospitalization have to meet the following three conditions to receive the service of HMS: 1) the patient must meet clinical safety standards to be waiting at home, with consideration of age under 60, no underlying diseases (e.g., chronic kidney disease, chronic lung disease, neurological conditions, diabetes, heart conditions, HIV infection, cancer, etc.),25 and general health condition must be evaluated as a good status by a triage/sickbed assignment team; 2) whether the patient is safe to stay home while waiting to be hospitalized must be confirmed by a triage/sickbed assignment team; and 3) patient must agree to receive management services provided by HMS while at home. However, standards may be changed in situations when COVID-19 sickbeds are insufficient.
OPERATION OF HMS26
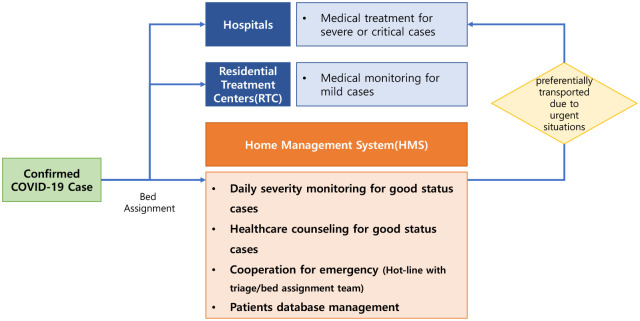
HMS starts with a local public healthcare center notifying the patient that he/she has been confirmed positive and that he/she has to await hospitalization at home (Fig. 1). The triage/bed assignment team allocates the confirmed case to either the hospitals or RTC based on severity, or the team decides to have the patient with clinically good conditions await hospitalization at home, in the event of lack of hospital beds.27 The triage/bed assignment team then notifies the assignment result to the public healthcare center in which the patient resides. The center informs the assignment to the HMS, which in turn notifies the patient. If the patient agrees to receive services from the system, the center transfers patient information to HMS team, and HMS team begins providing services to the patient.
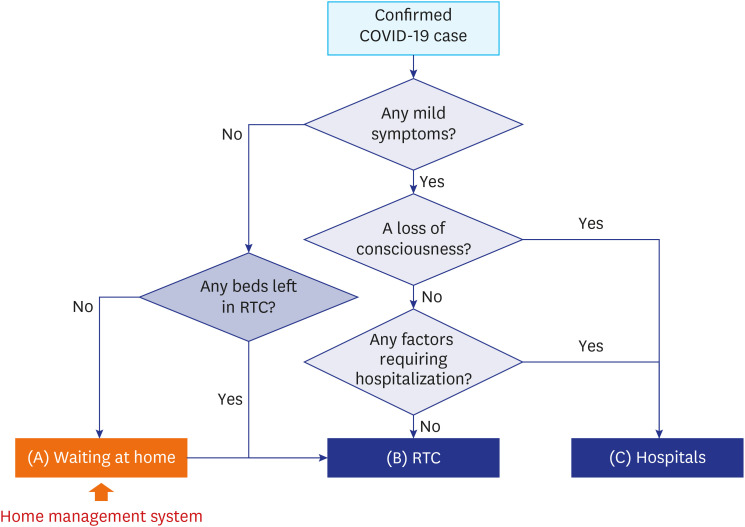
Fig. 1
A decision tree of the assignment process for confirmed cases.
(A) The confirmed case is assigned to ‘self-treat’ and stay at home if the patient has little or no symptoms and there is no bed at the RTC. The confirmed patient can receive home management while awaiting hospitalization. (B) The confirmed case is assigned to RTC if the patient has mild symptoms (e.g., cough, sore throat, chill). (C) The confirmed case is assigned to hospitals if the patient has any severe symptoms, loss of consciousness, or any other factors requiring hospitalization (e.g., dyspnea, heart failure, diabetes, dialysis patients, chronic lung disease, chemotherapy, organ transplantation, bedridden).
COVID-19 = coronavirus disease 2019, RTC = residential treatment center.
![]()
Organizations
Gyeonggi-do formed the HMS team for the management and operation of HMS. The first operating HMS team was formed in August of 2020, and it was comprised of 12 medical staff members, including 3 public health doctors and 9 nurses.21 The second operating HMS team was developed in December of 2020, and it consisted of 15 staff members, including 3 Korean medicine doctors (KMD), 11 nurses, and 1 general manager.28 A center of HMS was set up in the province control tower with a local disease control leader. In addition, the HMS team has cooperated with the triage/bed assignment team via an online communication channel to link HMS with the national government's confirmed cases management framework.
Main functions of HMS26
Daily severity monitoring
One of the main goals of HMS is for a medical staff – in most cases, a nurse – of HMS team to conduct a phone call to patients in efforts to monitor their condition once a day. It is designed to identify any significant changes in health and severity of condition. Additionally, patients can also call anytime as needed, and they are especially encouraged to make the call if new symptoms arise. Since the system is not a face-to-face measure and does not take place in a healthcare setting (i.e., home), delicate severity criteria had been developed for systematic monitoring based on Modified Early Warning Score (MEWS)29 and National Early Warning Score (NEWS).30 The severity of the patient is scored by 4-likert scale on four factors as body temperature, cardiopulmonary function, level of consciousness, and psychological status. If any factor's score or the sum of factors' score is greater than two points, HMS team assesses the severity and notifies the triage/bed assignment team. The triage/bed assignment team then takes action, such as requesting the patient to be admitted to RTC or hospitals. Detailed information of severity criteria is presented in Supplementary Table 1.
Healthcare counseling
A two-way communication channel between patients and HMS team has opened to allow patients to receive medical or psychological help if needed. Patients are encouraged to call HMS team member when they notice a change in their health status or have a medical question, such as how to receive medicine.
Cooperation for emergency
HMS team cooperates with the triage/bed assignment team to respond to the patient's emergency, such as a sudden change in the severity or other urgent situations (e.g., psychiatric, trauma, a refusal of the isolation, and escape). The staff not only immediately reports such case to the leader of HMS team, but also gets in contact with the triage/bed assignment team if the patient is determined to need a prompt treatment. The triage/bed assignment team then checks the condition of the patient, notifying the local public healthcare center, and takes necessary measures to admit the patient to hospitals or RTC.
Patients database management
The development of a database is essential to systematically manage and monitor confirmed cases in real time. The local government developed a real-time database platform ‘Gyeonggi-Do COVID-19 Management System (G-CoMS)’ to efficiently manage confirmed patients awaiting hospitalization at home.31 HMS team collects all information regarding these cases using the G-CoMS platform, including health status, monitoring and counseling results, etc. The platform can be used not only by the HMS team, but also by the triage/bed assignment team to check patients' severity.
OPERATION RESULTS OF HMS
HMS was operated for the first time for 17 days from August 28, 2020 to September 13, 2020 during the second surge of COVID-19 in South Korea. A total of 181 confirmed cases were eligible for the service, of which 8 cases were transported to the hospitals, and 63 cases were transported to RTC. Most of patients receiving the service were sequentially admitted to hospitals or RTC, but some patients were transported promptly if worsening of the severity was observed. HMS team terminated the service for the patient when triage/bed assignment team determined that the patient will be transferred to the hospital or RTC whether a reason of transporting was by sequential order or due to severity change. After the patient was transferred to the hospital/RTC, the patient was treated according to the government's COVID-19 response guidelines.
HMS was restarted during the third surge of COVID-19.32 It was re-operated on December 3, 2020, and is still being operated as of January 25. Out of a total of 4,696 confirmed cases who are waiting for hospitalization, 3,707 cases (78.9%) agreed to receive the service during the waiting so far. 3,668 cases assigned to the hospitals or RTC sequentially or promptly. Since December of 2020, the service can be terminated when the patient is officially released from isolation based on the government guidelines. If the patient is confirmed positive for COVID-19, and for a duration of 10 days he/she presents no clinical symptoms, then the public healthcare center officially declares the patient to be released from isolation.33 According to this rule, there were 21 cases released from isolation as more than 10 days have passed at home. As a result, there was no case of dying at home while awaiting hospitalization in the community.
DISCUSSION
Since self-treatment was not approved until the winter of 2020 in South Korea, all confirmed COVID-19 cases could only receive treatment after being admitted to hospitals or RTCs. Some cases inevitably had to wait several days at home without government support when the supply of COVID-19 sickbeds became scarce. The local government of Gyeonggi-do, which is the most populous self-governing province in South Korea, wanted to initiate a self-treatment plan to allow patients awaiting hospitalization to receive some medical attention at home to minimize health risks. However, there was no government guideline at the national level for self-treatment, and it was impossible for the local government to establish a system for self-treatment at the time. Therefore, the local government developed the HMS to safely manage the confirmed patients while they wait to be hospitalized.
HMS has several benefits. First, it was possible to manage medical supplies efficiently by re-arranging the confirmed cases based on a set of priorities. HMS prevented the number of deaths while awaiting hospitalization at home. Second, HMS supplemented the government's COVID-19 confirmed case management framework by monitoring and managing patients waiting for hospitalization at home. Also, such a continuous monitoring and open channel of communication allowed patients to get the relief of psychological anxiety as well as anxiety of their family members. Although this study did not derive a clear bases of it, it should be analyzed through patient satisfaction survey in future study. Third, it was possible to reduce the workload of the public healthcare centers. The burden of having to monitor patients was relieved by utilizing the HMS and the manpower of HMS team. These public healthcare centers were able to focus more on big-picture tasks, such as epidemiological investigation, environmental disinfection, and confirmed case transportation, and delegate individual monitoring of confirmed cases to HMS team. It can be said that the adaptation of HMS in Gyeonggi-do has inspired other provinces and self-governing cities to consider adopting such a system.
As mentioned above, the national government introduced the concept of self-treatment and amended the law - Article 41 of the Infectious Disease Prevention Act - in the winter of 2020 as a way to better respond to the pandemic. Several strategies should be considered in improving limits and integrating the HMS with self-treatment. First, it may be necessary to expand the breadth of services. Some patients did not have the basic medical equipment, such as thermometers, and lacked even simple medicines (e.g., antipyretics) at home. To build a better system, support and delivery of goods – medicines, daily necessities, and simple medical equipment – to patients at home may be required. Second, infection control guidance manuals to patients at home and their families should also be distributed.26 The spread of the infection was a concern if patients had family staying at the same home. It would be the best if there were spaces that patients could completely and physically self-isolate, but it is difficult in reality, so that manuals should be prepared to prevent the spread between families. Third, it is essential to establish a hotline so that patients can be transported quickly to hospitals or RTCs. HMS has established a communication channel between patients and the triage/bed assignment team; it may be necessary to establish an additional parallel communication channel with the local police office, EMS, and public healthcare center to provide faster action to patients. In addition, hospital beds must be prepared in dedicated hospitals to treat patients in crisis.26 Fourth, HMS should be organically linked within the confirmed cases management framework of the national government. There is promising news about the development of vaccines for COVID-19; however, it will take time to form herd immunity within the country.34 In preparation for the possible surge in the future, it is essential to secure medical supplies and to supplement the system and self-treatment. Finally, the most essential strategy is the active cooperation between the various players, including role-sharing, within the self-governing cities. City governments and public healthcare centers are essential players to better respond to infectious diseases, not just in South Korea, but elsewhere. In order to implement the system or self-treatment as a response measure to COVID-19, the city governments should prepare specific strategies. To sum up, the national government must create policy and guidelines, and the local governments must develop a system based on the national policy and guidelines. Local governments must then share roles with public healthcare centers, cooperate with local doctors, and encourage the community to proactively participate in the response of the pandemic.
In conclusion, this paper introduces the HMS of Gyeonggi-do and provides an overview of the development of this system and how it can evolve moving forward. Institutional limitations placed on the HMS should be mitigated and develop strategies to integrate and expand self-treatment. The roles of local and city governments are more important than the national government in the pandemic. The efforts of local governments, such as the development of HMS, will play a key role in pandemic preparedness.
 XML Download
XML Download