

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Olfactory dysfunction is a common problem encountered by otorhinolaryngologists. Olfaction is an important factor for sensing the world, and olfactory dysfunction influences the quality of life by altering the flavor of foods and causing difficulty in detecting environmental hazards such as spoiled foods, natural gas, and smoke. The prevalence of olfactory dysfunction has remained quite high due to industrial accidents, rhinologic diseases, aging, and neurodegenerative diseases.12 The assessment of patients with olfactory dysfunction should involve a detail medical history, focusing on the events that may be related to the onset of olfactory dysfunction, such as nasal and paranasal sinus disease, upper respiratory infections, head trauma, and exposure to environmental chemicals.3 To properly evaluate patients with olfactory dysfunction, we have used several olfactory function tests, including the University of Pennsylvania Smell Identification Test (UPSIT),4 Sniffin' Sticks Test,5 Toyoda and Takagi's Perfumist's Strip Method (T&T olfactometry),6 Butanol Threshold Test (BTT),7 and Cross Cultural Smell Identification Test (CCSIT).8 These tests are widely used for olfactory function evaluation, but do not measure the objective body response to odorants, and have limitations as psychophysical tests that rely on the subjective response of the patient. There are tests that can be performed by the patients themselves, but many tests must be conducted according to the tester's instructions.
Recent studies have reported that patients with coronavirus disease 2019 (COVID-19), a worldwide pandemic infection, frequently complain of olfactory disorders.910111213 However, face-to-face examinations performed by an examiner are very difficult in these highly infectious patients. In addition, there may be a situation in which it is very difficult to perform olfactory tests for all infected people in a situation in which COVID-19 occurs on a large scale worldwide. To address these difficulties, there is a need for a way to supplement or replace these psychophysical tests. A questionnaire for olfactory symptoms has the potential to serve this purpose. In this circumstance, the olfactory function questionnaire can be an alternative tool to evaluate olfactory dysfunction and help assess patients. In addition, the odors used in the olfactory function tests, such as in the CCSIT, were limited and did not reflect all the odors in daily life. Therefore, a questionnaire with odors in daily life may provide supplementary information for evaluating patients with olfactory dysfunction. Several previous studies have shown that olfactory dysfunction can be assessed to some extent by surveying olfactory symptoms.1415161718 The “Questionnaire of Olfactory Disorder” was developed in a previous study, and has been widely used to evaluate olfactory dysfunction.15 However, it focuses on qualitative olfactory dysfunction (e.g., parosmia) and quality of life. Therefore, a questionnaire with established reliability and validity that quantifies olfactory dysfunction is necessary when olfactory function testing is not available. The sense of smell, unlike other senses, is highly influenced by culture. Therefore, the questionnaire for evaluating olfactory impairment should consider the cultural environment related to olfaction, such as eating habits. This study aimed to develop and verify questionnaires to evaluate olfactory function that reflect cultural factors related to the sense of smell in Koreans and can be easily evaluated by those who complain of olfactory dysfunction.
METHODS
Development of olfactory questionnaires
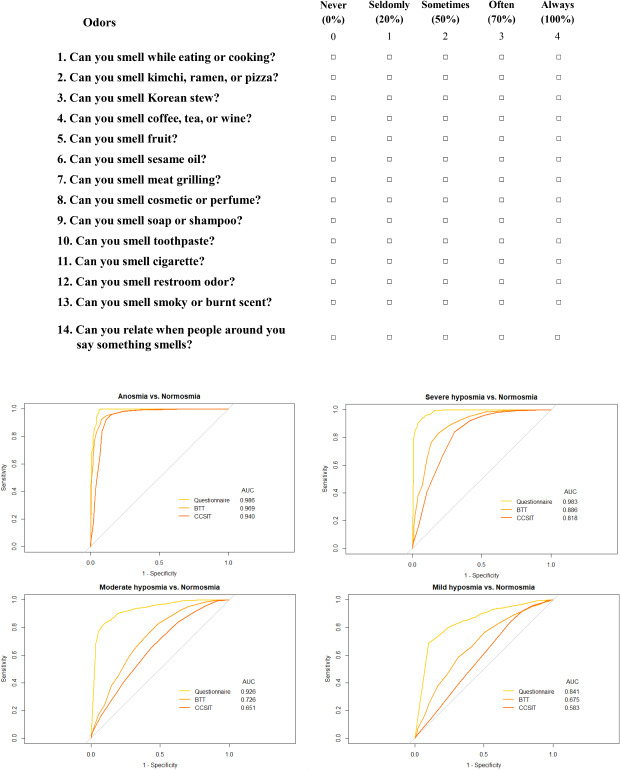
We developed an olfactory symptom questionnaire consisting of 14 questions with 1 question on odor occurring in daily life, 9 on specific odors familiar to Koreans, 3 on trigeminal nerve-related odors, and 1 on olfactory status evaluated by people around the subject. Four points were given when the subject smelled well, and 0 point when the subject did not smell at all (Table 1).
Table 1
Olfactory questionnaire with 14 items <Please indicate your sense of smell in 14 situations below>
Psychophysical olfactory tests
The BTT and CCSIT were performed as described above.19 A BTT test kit consisting of 13 levels was prepared by continuously diluting n-butanol (Sigma-Aldrich Co., St Louis, MO, USA) three times with odorless mineral oil. The subjects were given two bottles, one containing only mineral oil and the other containing diluted butanol. Subjects were forced to choose a bottle that they think smells butanol. The BTT started at the most diluted concentration (level 12) and proceeded to a higher concentration level by level. The CCSIT consisted of 12 items: banana, chocolate, cinnamon, gasoline, lemon, onion, paint thinner, pineapple, rose, soap, smoke, and turpentine. Subjects were forced to identify one of the four options. The BTT was performed separately in each nostril, while CCSIT was performed simultaneously in both nostrils.
Self-rating of olfactory dysfunction
The subjects were asked to rate their olfactory function that they feel subjectively from among five categories of olfactory function, including normosmia (“I can always smell.”) mild hyposmia (“I can often smell.”), moderate hyposmia (“I can sometimes smell”), severe hyposmia (“I can seldomly smell”), and anosmia (“I can never smell”).
Test-retest reliability
We asked volunteers to fill out the same olfactory symptom questionnaire twice to determine the final items of the olfactory function questionnaire. Volunteers received two tests at two-week intervals to reduce the carry-over effect,20 and we evaluated the test reliability by the degree of agreement between the respondents' options for the 14 items in tests 1 and 2. To assess test-retest reliability, the κ statistic was calculated, providing the estimate of agreement corrected for chance.21 Agreement was judged based on the classification of Landis and Koch22; the strength of agreement was considered almost perfect when κ was > 0.8, substantial when 0.6 < κ ≤ 0.8, and moderate when 0.4 < κ ≤ 0.6. Under the condition of κ0 = 0.4, alpha = 0.05, and a statistical power = 0.8, we assumed the true κ value 0.7 because the two tests were not completely independent. We thought the reasonable κ value for the strength of agreement was κ > 0.6 as it represents a substantial statistical significance, and the items with κ > 0.6 were included in the final version of the olfactory questionnaire. The minimal sample size for the assumption was 25 volunteers.23 As the reliability increase as the number of samples increases, we enrolled 45 volunteers for test-retest reliability.
Statistical analyses
Continuous variables, such as age and total score of the olfactory questionnaire, were presented as the mean ± standard deviation; these variables were analyzed using two-sample t-tests or analysis of variance (ANOVA). Post hoc analysis was performed using Tukey's method for the ANOVA results. In addition, the correlation between the items in the questionnaire and olfactory function test (BTT and CCSIT) was assessed using the Pearson correlation coefficient (r). The correlations between the total scores of the questionnaire and the olfactory function tests were compared using Fisher Z-transformation.24 We conducted multiple linear regressions to evaluate the correlation between the total score of the questionnaire and the olfactory function tests (BTT and CCSIT), adjusting for age and sex. A receiver operating characteristic (ROC) curve of the total score of the questionnaire was generated to find the best cutoff for predicting olfactory dysfunction. The area under the curve (AUC) for the total score of the questionnaire was calculated. Among several cutoff points, the lowest (1 − sensitivity)2 + (1 − specificity)2 value was selected as the optimal cutoff value. All statistical analyses were conducted using SPSS version 22.0 for Windows (IBM, Armonk, NY, USA) and R for Windows version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria). A P value of < 0.05 was considered significant.
Ethics statement
We retrospectively recruited patients over the age of 18 years who had been tested using the BTT and CCSIT, and surveyed olfactory symptom questionnaires at the smell clinic of the Seoul National University Bundang Hospital. This study was approved by the Institutional Review Roard (IRB) of the Seoul National University Bundang Hospital (IRB No. B-1509/314-114). The retrospective review of medical records was conducted with the exemptions of informed consent and test-retest reliability was assessed with the presence of informed consent.
RESULTS
Determination of questionnaire items by test–retest reliability test
Forty-five subjects (30 male) participated in the test-retest reliability test, and their mean age was 25.7 ± 2.1 years. Among the 14 items in the questionnaire, 3 questions had κ ≤ 0.6, and these items were excluded (Table 2). Therefore, 11 questions with a total score of 44 were selected for the final version of the olfactory questionnaire set.
Table 2
Kappa statistics of 14 items of the questionnaire
Correlation between total olfactory questionnaire scores and BTT or CCSIT scores
The BTT, CCSIT, and olfactory questionnaires from 2,273 subjects (1,260 males) between January 2012 and April 2015 were used for correlation analysis, and their mean age was 46.5 ±16.0 years. Of the 2,273 patients, 1,047 rated their olfactory function as normosmia, 305 as mild hyposmia, 264 as moderate hyposmia, 402 as severe hyposmia, and 255 as anosmia. When the subjects were classified into five groups according to the self-rating, the total score of the olfactory questionnaire was 41.1 ± 6.0, 31.6 ± 8.9, 24.5 ± 9.5, 12.8 ± 9.0, 4.8 ± 9.2 for normosmia, mild hyposmia, moderate hyposmia, severe hyposmia and anosmia, respectively (P < 0.001) (Table 3). In addition, post-hoc analysis revealed significant differences (P < 0.001 for all comparisons between different two groups). There were significant correlations between the total olfactory questionnaire score and the BTT or CCSIT scores (r = 0.643 and r = 0.615, respectively, P < 0.001 for both) (Fig. 1A and B). The correlation coefficient in the total olfactory questionnaire score was significantly higher in the BTT group than in the CCSIT group (P = 0.022). Multivariate analysis showed that the total olfactory questionnaire score also significantly correlated with the BTT (β = 0.222, P < 0.001) and CCSIT (β = 0.114, P < 0.001) scores, even when adjusted for age and sex.
Table 3
Total score of the verified questionnaire according to the subjective olfactory function scale

Determination of the cutoff value for hyposmia/anosmia
ROC curves were created to determine the predictive power of the olfactory questionnaire, BTT and CCSIT for mild hyposmia, moderate hyposmia, severe hyposmia, or anosmia from normosmia, respectively (Fig. 2). The self-rating scale for olfactory dysfunction was used as a reference. The predictive power of the olfactory questionnaire, BTT or CCSIT tends to be higher in severe olfactory dysfunction. The AUCs of the olfactory questionnaire, BTT and CCSIT were comparable when predicting anosmia from normosmia. However, the AUCs of BTT and CCSIT were much lower than AUC of olfactory questionnaire when predicting moderate or mild hyposmia from normosmia (Fig. 2C and D). In other words, the predictive power of olfactory questionnaire remains high in mild olfactory dysfunction, while the predictive power of BTT or CCSIT is low in mild olfactory dysfunction. To identify the cutoff threshold scores for olfactory questionnaire, ROC curves among the subclasses (anosmia vs. severe hyposmia, severe hyposmia vs. moderate hyposmia, moderate hyposmia vs. mild hyposmia, and mild hyposmia vs. normosmia) were created (Supplementary Fig. 1). Based on the cutoff threshold scores, we suggest the classification of total score of the questionnaire as 0–4, 5–17, 18–27, 28–41, and 42–44 for anosmia, severe hyposmia, moderate hyposmia, mild hyposmia, and normosmia, respectively (Table 4).
Fig. 2
ROC curves for the total score of the olfactory questionnaire, BTT and CCSIT scores to predict the four levels of olfactory dysfunction from normosmia: (A) anosmia, (B) severe hyposmia, (C) moderate hyposmia, and (D) mild hyposmia. The self-rating scale for olfactory dysfunction is used as a reference. The predictive ability is calculated based on the AUC.
ROC = receiver operating characteristic, BTT = Butanol Threshold Test, CCSIT = Cross Cultural Smell Identification Test, AUC = area under the curve.


DISCUSSION
In the present study, we developed and validated questionnaires for olfactory dysfunction and evaluated the correlations between the olfactory questionnaire score and psychophysical olfactory function tests such as the BTT and CCSIT. Although psychophysical olfactory function tests are widely used to evaluate olfactory problems in hospitals, these tests are not available in many general health exams because they require a certain amount of time and cost. In addition, some primary clinics do not have equipment for psychophysical olfactory function tests, and have difficulty in screening patients who have problems in smell. A recent study reported that olfactory dysfunction can be a biomarker for COVID-19, which suggests the role of olfactory function test as a screening tool.25 However, it is very difficult to perform olfactory tests for the many suspected cases of COVID-19 because of the risk of infection, even in clinics. To address these situations, in which psychophysical olfactory function tests were unavailable, an alternative tool to evaluate olfactory dysfunction is necessary. Our previous study showed a positive correlation between the questions for subjective olfactory function in daily life and the olfactory function test (Korean Version of Sniffin' Sticks Test and BTT).26 However, the questions in our previous study were not verified, and the sum of the scores for each question was not evaluated. Hence, an established questionnaire for olfactory function is necessary.
In this study, we developed the appropriate items for the questionnaire for Koreans and verified them by test-retest reliability. After validation, 11 out of 14 question items were selected for the questionnaires. The total score for the olfactory questionnaire significantly correlated with the BTT and CCSIT scores. Interestingly, the correlation coefficient between the total score of the questionnaire and the BTT score was significantly higher than that of the CCSIT. The olfactory questionnaire seems to be an identification test because it contains several questions for various odors. However, the answer to the questions is scaled, not “yes or no”, and it also plays the role of a threshold test. The correlation coefficient between the total score of the questionnaire and the CCSIT score was high (> 0.6), which indicates the role of the olfactory questionnaire as an identification test. Furthermore, the multivariate analysis revealed that the total score of the questionnaire significantly correlated with the BTT and CCSIT scores when adjusting for age and sex. The ROC values showed predictive power of the olfactory questionnaire in evaluating the severity of olfactory dysfunction. The AUCs for the olfactory questionnaire were high in predicting each level of olfactory dysfunction; however, the AUCs for BTT and CCSIT were low in predicting mild or moderate hyposmia. This result indicates that the olfactory questionnaire can be a supplementary tool to evaluate mild olfactory dysfunction. Based on the cutoff threshold scores elicited from the ROC curves between the subclasses, we suggest the classification of the questionnaire that is readily used. However, despite the good performance for discriminating mild or moderate hyposmia from normosmia, the AUC value for discriminating between mild and moderate hyposmia was low (AUC = 0.704). This may be because the difference between mild and moderate hyposmia is very uncertain and it is difficult to differentiate between the two groups.
This study has some limitations. First, we used a self-rating scale when eliciting the classification of olfactory questionnaire scores; however, these references do not always indicate the actual values for olfactory dysfunction. Although EEG can objectively evaluate patients with olfactory dysfunction, it is not commonly used in practice, and its accuracy is not 100%.2728 Therefore, the absence of an actual reference is an obstacle to evaluating olfactory function tests. However, we showed that the classification of olfactory questionnaire scores using a self-rating scale is comparable to those using the BTT and CCSIT, which supports the reliability of the classification. Second, the olfactory questionnaire is not a forced choice test, which is not able to distinguish malingering patients. The olfactory tests have the limitation to discriminate malingering patients because they are not completely objective. Therefore, the olfactory questionnaire has the same problem in discriminating the malingering patients as well. However, there might be a possibility to be able to distinguish malingering through comparison between the score of trigeminal nerve related odors and other scores, which needs to be validated in another prospective study design. Despite this limitation, this study has some distinct strengths. The items of the questionnaire underwent the verification process and were selected properly. Furthermore, in addition to evaluating the correlation between the scores of the questionnaire and the scores of olfactory function tests, we suggested the appropriate threshold values of the total score of the questionnaire to predict olfactory dysfunction, which may help the practical use of the questionnaire.
In conclusion, the olfactory questionnaire with 11 items was elicited by test-retest reliability. The total score of the questionnaires correlated with the BTT and CCSIT scores. The classification of olfactory dysfunction for the questionnaire was based on the self-rating scale. We believe this questionnaire is useful as an alternative diagnostic tool when olfactory function tests are not available.
 XML Download
XML Download