

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) was declared as a pandemic on March 11, 2020 by the World Health Organization (WHO),1 causing a public health crisis, triggering disruptions to healthcare systems, and endangering the control and prevention of common endemic diseases. A recent survey targeted at healthcare professionals suggested that diabetes, chronic obstructive pulmonary disease, and hypertension were the most impacted chronic illnesses, due to reduction in access to routine care.2 Management of tuberculosis (TB), one of the oldest endemic infectious diseases, was unavoidably affected by the COVID-19 pandemic. Many experts warn of a severe effect on TB management and control.34
After experiencing a huge outbreak of COVID-19 in late February 2020 in Daegu, with widespread transmission throughout the country, the Korean government raised the country's infectious disease alert to the highest level on February 23, 2020.5 Subsequently, all of Korea's capabilities were focused on COVID-19 management, which resulted in severe reductions in health service availability and access to care for patients with other chronic diseases, such as TB. Kwak et al.6 reported that TB notification decreased significantly with the surge of COVID-19 in Korea. This could result in delays in TB diagnosis and treatment and increased risk of poor treatment outcomes, which are important areas for further research.
The national Public-Private Mix (PPM) TB control project was implemented in 2011 in order to provide comprehensive management for TB patients at private hospitals in Korea.7 The Korean PPM monitoring database was established to evaluate the activities of PPM project-participant hospitals and provides quarterly monitoring indicators of TB management from 2014 onwards. Herein, we investigated the nationwide effects of COVID-19 on the PPM project in Korea, using monitoring indicators from the Korean PPM monitoring database.
METHODS
Setting
Korea, an intermediate-TB burden country, has a high TB incidence rate among high-income countries. In 2019, the overall notification rate of new TB cases was 46.4 per 100,000 population, with a reduction of 9.9% from the previous year's rate.8 In 2017, 127 PPM hospitals participated in the national PPM TB control project, which managed 68.7% of TB cases throughout the country. The PPM project is operated by the Korean Academy of Tuberculosis and Respiratory Diseases, under the supervision of the Korea Disease Control and Prevention Agency (KDCA). There is a central steering committee and 21 regional committees to monitor patient management in PPM hospitals.
Korean PPM monitoring database
TB is a nationally notifiable disease in Korea and is monitored using the Korean National TB Surveillance System (KNTSS), a web-based system launched in 2000.9 The Korean PPM monitoring database includes data from patients reported at PPM hospitals. The KDCA has the primary responsibility for accessing the TB notification data of the KNTSS. Based on the notification date, TB patients at PPM hospitals are enrolled in each quarter of the calendar year, which forms a cohort. Indicators of each cohort are generated every quarter and released in the first month of the next quarter. Every cohort is updated and analyzed five times, thus followed up for at least 12 months to identify treatment outcomes (Supplementary Methods).
Definitions of the monitoring indicators
Of the 25 monitoring indicators,7 data on the following six for active TB cases were collected in this study: 1) sputum acid-fast bacilli (AFB) smear test coverage among pulmonary TB cases, 2) sputum culture test coverage among pulmonary TB cases, 3) adherence to initial standard anti-TB treatment, 4) drug susceptibility test (DST) coverage among all culture-confirmed TB cases, 5) loss to follow-up (LTFU) rate among the drug-susceptible TB cohort, and 6) treatment success rate among the smear-positive drug-susceptible pulmonary TB cohort. The final treatment outcomes were reported in accordance with the WHO treatment definitions,10 which are endorsed by the Korean TB guidelines.11
Data collection
Data updated between July 2019 (the third quarter of 2019) and June 2020 (the second quarter of 2020) were collected for the purpose of the current study.7 To evaluate changes in smear and culture coverages and adherence to standard regimens before and after the COVID-19 outbreak, cohort data from the third and fourth quarters of 2019 and the first and second quarters of 2020 were collected and analyzed. For DST coverage, cohort data from the second, third, and fourth quarters of 2019 and the first quarter of 2020, which were collected and updated for the second analysis, were used. For LTFU and treatment success rates, cohort data from the third and fourth quarters of 2018 and the first and second quarters of 2019, which were collected and updated for the fifth analysis, were used.
All the data from each cohort throughout the country were collated to provide the national data. The five regions with the most reported cased of COVID-19 as of July 4, 2020 were selected and re-categorized into two regions based on their proximity: Daegu and Gyeongbuk, and Seoul Metropolitan Area (Seoul, Incheon, and Gyeonggi).12 In addition, two regions with the fewest reported cases of COVID-19 were selected and combined into one region: Jeonnam and Jeonbuk. All the data from each cohort in the prespecified regions were collated to provide the regional data.
Statistical analysis
Data were presented as numbers with percentages. Categorical variables were compared using the χ2 test for trend to evaluate the quarterly trends of each monitoring indicator at the national level and in the pre-specified regions. All tests were two-tailed, and P < 0.05 indicated statistical significance. Statistical analyses were performed using SPSS Statistics for Windows, version 17.0 (SPSS Inc., Chicago, IL, USA). We also calculated percentage changes in treatment success rates before and after COVID-19 for each administrative region. Cohort data from the third and fourth quarters of 2018 were collated to comprise the “before COVID-19” cohort. Cohort data from the first and second quarters of 2019 were collated to comprise the ‘after COVID-19’ cohort.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki. The Institutional Review Board (IRB) of Daejeon St. Mary's Hospital, The Catholic University of Korea approved the study protocol, and waived the need for informed consent because no patients were at risk (IRB No. DC20ZADI0069). The KDCA, Republic of Korea, has authority to hold and analyze surveillance data for public health and research purposes.
RESULTS
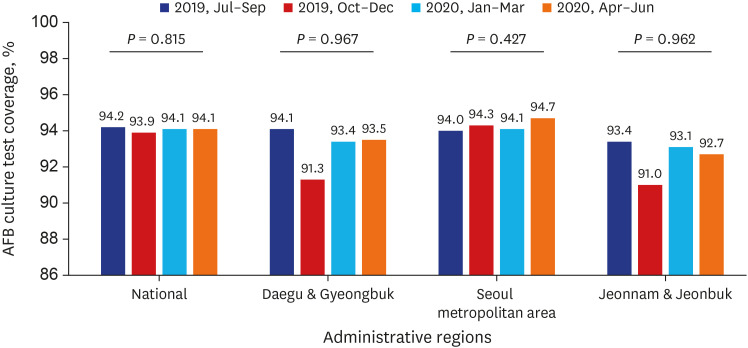
The number of pulmonary TB cases notified at PPM hospitals nationwide decreased from 6,066 in the third quarter of 2019 to 4,893 in the second quarter of 2020 (Supplementary Table 1). However, sputum AFB smear test coverage at the national level was not significantly different between the same periods (P = 0.622) (Fig. 1). Sputum smear test coverage in other regions also showed similar results. Sputum AFB culture test coverage at the national level was not significantly different between the same periods (P = 0.815) (Fig. 2 and Supplementary Table 2). Sputum culture test coverage in other regions also showed similar results.
Fig. 1
Sputum AFB smear test coverage among pulmonary TB cases, which were initially registered for the third and fourth quarters of 2019 and the first and second quarters of 2020.
Sputum AFB smear test coverage was calculated as the number of patients who had sputum smear test performed divided by the number of patients with pulmonary TB. Cohort data from the third and fourth quarters of 2019 and the first and second quarters of 2020 were collected and updated between July 2019 (the third quarter of 2019) and June 2020 (the second quarter of 2020).
AFB = acid-fast bacilli, TB = tuberculosis.
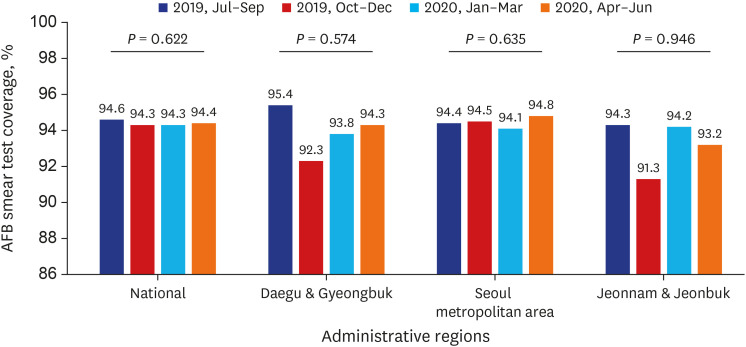
Fig. 2
Sputum AFB culture test coverage among pulmonary TB cases, which were initially registered for the third and fourth quarters of 2019 and the first and second quarters of 2020.
Sputum AFB culture test coverage was calculated as the number of patients who had sputum culture test performed divided by the number of patients with pulmonary TB. Cohort data from the third and fourth quarters of 2019 and the first and second quarters of 2020 were collected and updated between July 2019 (the third quarter of 2019) and June 2020 (the second quarter of 2020).
AFB = acid-fast bacilli, TB = tuberculosis.
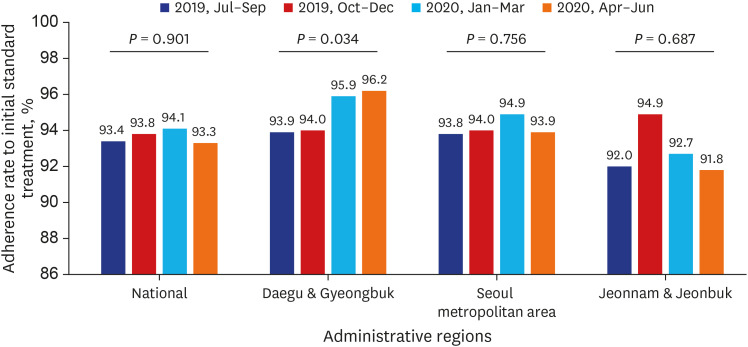
Adherence rate to initial standard anti-TB treatment recommended by the guidelines at the national level was not significantly different between the same periods (P = 0.901) (Fig. 3 and Supplementary Table 3). However, adherence rate to standard treatment in the Daegu-Gyeongbuk area increased significantly from the third quarter of 2019 to the second quarter of 2020 (P = 0.034).
Fig. 3
Adherence to initial standard anti-TB treatment recommended by the guidelines among TB cases, which were initially registered for the third and fourth quarters of 2019 and the first and second quarters of 2020.
Adherence to initial standard anti-TB treatment was calculated as the number of patients treated with initial standard regimens, including H+R+E+Z, H+R+E, H+E+Z+Rfb, or H+E+Rfb, divided by the number of patients eligible for initial standard anti-TB treatment recommended by the guidelines. Patients with isoniazid-resistant TB, RR-TB, and MDR-TB were excluded. Patients whose data regarding anti-TB drugs were not entered in the Korean National TB Surveillance System were excluded. Patients registered as “treatment after failure” were excluded. Cohort data from the third and fourth quarters of 2019 and the first and second quarters of 2020 were collected and updated between July 2019 (the third quarter of 2019) and June 2020 (the second quarter of 2020).
TB = tuberculosis, H = isoniazid, R = rifampicin, E = ethambutol, Z = pyrazinamide, Rfb = rifabutin. RR = rifampicina resistant, MDR = multidrug resistant.
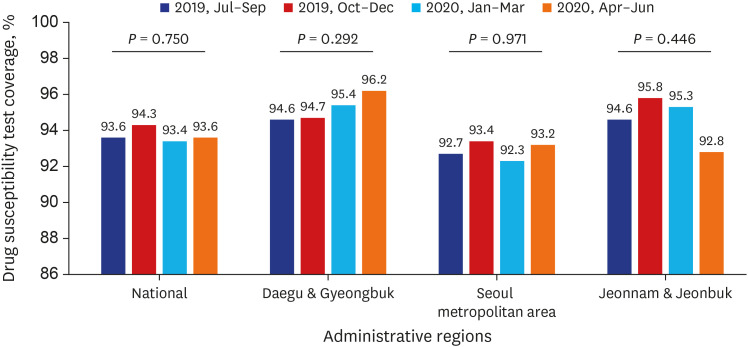
DST coverage among culture-confirmed TB cases from the cohort data from the second, third, and fourth quarters of 2019 and the first quarter of 2020 were updated for the second analysis between July 2019 and June 2020 and was not significantly different at the national level (P = 0.750) (Fig. 4 and Supplementary Table 4). DST coverage in other regions between the same periods also showed similar results.
Fig. 4
Drug susceptibility test coverage among culture-confirmed TB cases, which were initially registered for the second, third, and fourth quarters of 2019 and the first quarters of 2020.
Drug susceptibility test coverage was calculated as the number of patients with culture-based or molecular drug-susceptible test results divided by the number of patients with culture-confirmed TB cases. Cohort data from the second, third, and fourth quarters of 2019 and the first quarter of 2020 were collected and updated between July 2019 (the third quarter of 2019) and June 2020 (the second quarter of 2020).
TB = tuberculosis.
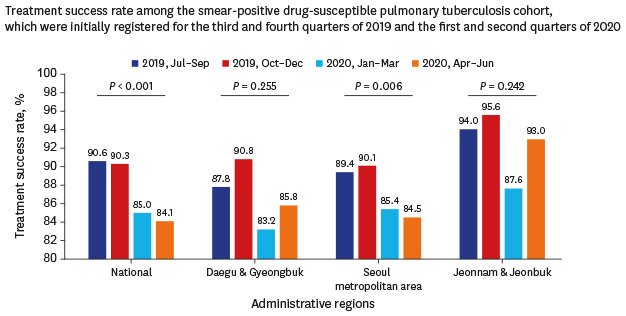
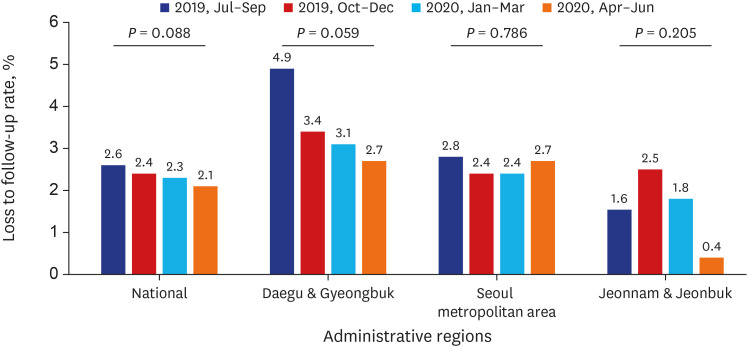
Treatment success rate and LTFU rate from the cohort data from the third and fourth quarters of 2018 and the first and second quarters of 2019 were updated for the final analysis between July 2019 and June 2020. Treatment success rate among the smear-positive drug-susceptible pulmonary TB cohort significantly decreased from 90.6% to 84.1% (P < 0.001) (Fig. 5 and Table 1). Treatment success rate in the Seoul Metropolitan Area also significantly decreased, from 89.4% to 84.5% (P = 0.006). The LTFU rate among tuberculosis cases at the national level decreased from 2.6% to 2.1% but was not statistically significant (P = 0.088) (Fig. 6 and Supplementary Table 5). The LTFU rate in other regions between the same periods also did not show significant changes.
Fig. 5
Treatment success rate among the smear-positive drug-susceptible pulmonary TB cohort, which were initially registered for the third and fourth quarters of 2018 and the first and second quarters of 2019.
Treatment success rate was calculated as the number of smear-positive drug-susceptible pulmonary TB cases that were successfully treated divided by the number of smear-positive drug-susceptible pulmonary TB cases registered as treatment success, treatment failed, loss to follow-up, died, and still on treatment. Smear-positive pulmonary TB cases are defined by ICD-10 codes (A15.00 or A15.01) and positive results of sputum AFB smear tests. Patients with RR-TB and MDR-TB were excluded. Patients who were “transferred out” to another treatment unit, returned to their home country, and died of non-TB-related causes were excluded. Cohort data from the third and fourth quarters of 2018 and the first and second quarters of 2019 were collected and updated between July 2019 (the third quarter of 2019) and June 2020 (the second quarter of 2020).
TB = tuberculosis, ICD = International Classification of Diseases, AFB = acid-fast bacilli, RR = rifampicina resistant, MDR = multidrug resistant.
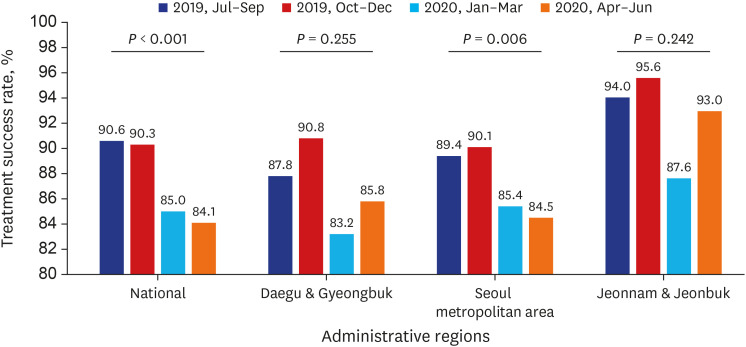
Table 1
Treatment success rate among the smear-positive drug-susceptible pulmonary TB cohort, initially registered for the third and fourth quarters of 2018 and the first and second quarters of 2019
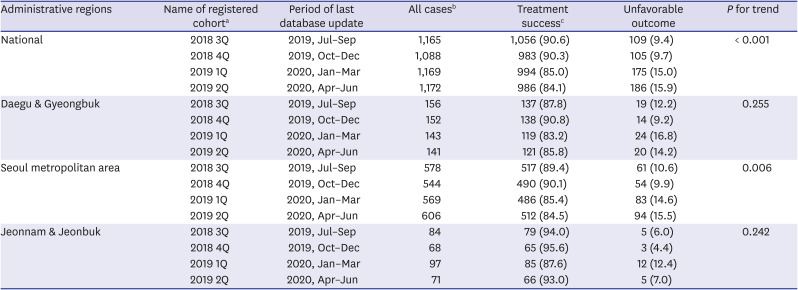
Data are presented as number (%).
TB = tuberculosis, Q = quarter, ICD = International Classification of Diseases, AFB = acid-fast bacilli, RR = rifampicina resistant, MDR = multidrug resistant.
aCohort data from the third and fourth quarters of 2018 and the first and second quarters of 2019 were collected and updated between July 2019 (the third quarter of 2019) and June 2020 (the second quarter of 2020); bDenominator: number of smear-positive drug-susceptible pulmonary TB cases registered as treatment success, treatment failed, loss to follow-up, died, and still on treatment. Smear-positive pulmonary TB cases are defined by ICD-10 codes (A15.00 or A15.01) and positive results of sputum AFB smear tests. Patients with RR-TB and MDR-TB were excluded. Patients who were “transferred out” to another treatment unit, returned to their home country, and died due to non-TB-related causes were excluded; cNumerator: number of smear-positive drug-susceptible pulmonary TB cases in patients who were successfully treated.
Fig. 6
Loss to follow-up rate among TB cases, which were initially registered for the third and fourth quarters of 2018 and the first and second quarters of 2019.
Loss to follow-up rate was calculated as the number of TB cases that were registered as loss to follow-up divided by the number of TB cases registered as treatment success, treatment failed, loss to follow-up, died, and still on treatment. Patients with RR-TB and MDR-TB were excluded. Patients who were “transferred out” to another treatment unit, returned to their home country, and died due to non-TB-related causes were excluded. Cohort data from the third and fourth quarters of 2018 and the first and second quarters of 2019 were collected and updated between July 2019 (the third quarter of 2019) and June 2020 (the second quarter of 2020).
TB = tuberculosis, RR = rifampicina resistant, MDR = multidrug resistant.
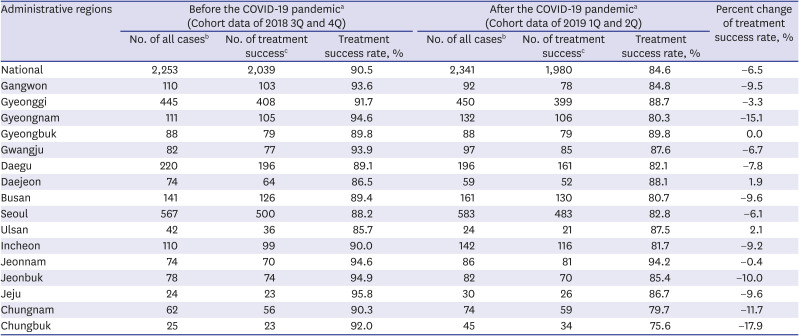
Treatment success rate at the national level decreased from 90.5% before COVID-19 to 84.6% after COVID-19, with percentage change of −6.5% (Table 2). Chungbuk province had the highest percentage change in the treatment success rate before and after COVID-19 (−17.9%), followed by Gyeongnam (−15.1%), Chungnam (−11.7%), and Jeonbuk (−10.0%).
Table 2
Treatment success rate among the smear-positive drug-susceptible pulmonary TB cohort before and after the COVID-19 pandemic
TB = tuberculosis, COVID-19 = coronavirus disease 2019, Q = quarter, ICD = International Classification of Diseases, AFB = acid-fast bacilli, RR = rifampicina resistant, MDR = multidrug resistant.
aCohort data from the third and fourth quarters of 2018 and the first and second quarters of 2019 were collected and updated between July 2019 (the third quarter of 2019) and June 2020 (the second quarter of 2020); bDenominator: number of smear-positive drug-susceptible pulmonary TB cases registered as treatment success, treatment failed, loss to follow-up, died, and still on treatment. Smear-positive pulmonary TB cases are defined by the ICD-10 codes (A15.00 or A15.01) and positive results of sputum AFB smear tests. Patients with RR-TB and MDR-TB were excluded. Patients who were “transferred out” to another treatment unit, returned to their home country, and died due to non-TB-related causes were excluded; cNumerator: number of smear-positive drug-susceptible pulmonary TB cases in patients who were successfully treated.
DISCUSSION
This is the first study to assess performance changes in the national PPM TB control project following the COVID-19 pandemic in Korea. Coverages of AFB smear and culture tests and DST were above 90% in our study, which implies that the initial case management of newly notified TB patients was carried out properly at PPM hospitals regardless of the pandemic. A previous study showed that the initial coverages of smear and culture tests and DST increased significantly from the first quarter of 2016 to the fourth quarter of 2017.7 High coverage of essential diagnostic tests in the current study could be ascribed to the comprehensive case management provided by TB specialist nurses under the PPM project. The WHO has highlighted that all measures should be taken to ensure continuity of services for people who need preventive and curative treatment for TB amid the COVID-19 pandemic.13 Since many countries are seeing a second wave of COVID-19 after relaxing social distancing rules, appropriate planning and monitoring activities regarding TB are essential to provide sustainability of essential TB services.
Treatment success rate among smear-positive pulmonary TB cohorts decreased from 90.5% before the pandemic to 84.6% after. As the treatment outcomes were assessed at the time of deregistration, all TB cases evaluated for treatment outcomes in our study were registered between the third quarter of 2018 and the second quarter of 2019. Thus, the true impacts of the COVID-19 pandemic on early TB management, which could consequently worsen the treatment outcomes, cannot be assessed in our study. Since the LTFU rate was not significantly different before and after the pandemic in our study, we could hypothesize that increasing numbers of cases with treatment interruption less than two months after the COVID-19 pandemic led to increasing numbers of still-on-treatment cases at the final (fifth) analysis. In addition, since the TB patients scheduled to finish their anti-TB treatment might miss their last visit to the outpatient clinics, the increased numbers of under-reported treatment success cases could account for the apparently low treatment success rates after the COVID-19 pandemic. Due to unavailability of individual data, we cannot elucidate the exact causes of decreasing treatment success rates during our study period. Advanced analysis, such as interrupted time series analysis,1415 with additional data from future cohorts is necessary to provide a more detailed assessment of the longitudinal effect of the COVID-19 pandemic and explore any seasonal trends.
Adherence rate to initial standard treatment recommended by the guidelines in the Daegu-Gyeongbuk Area significantly improved after the COVID-19 pandemic. One of the possible reasons for the low adherence rate to standard treatment in routine clinical settings in Korea is that TB patients, especially the elderly, are transferred to PPM hospitals after experiencing adverse drug reactions and often restart the treatment regimens with second-line anti-TB agents, which is counted as a non-adherent case. Between late February and April 2020, movement between regions or hospitals was strictly prohibited due to persistent episodes of COVID-19 outbreaks in the Daegu-Gyeongbuk area. As of July 4, 2020, 63.4% of COVID-19 cases occurred in the Daegu-Gyeongbuk area.12 Thus, we can hypothesize that the number of TB patients who transferred to PPM hospitals in the Daegu-Gyeongbuk area has decreased, which could, in turn, improve adherence rates after the COVID-19 pandemic.
Comprehensive TB case management under the PPM project in 2011 and establishment of a TB epidemic investigation team in 2013 have had pivotal roles in continuing the annual reduction of TB incidence rates following the stagnation between 2000 and 2011 in Korea. The current COVID-19 pandemic is a global health crisis, causing substantial disruption to healthcare systems. The recent outbreak of Ebola in West Africa has severely compromised TB programs and negatively affected treatment outcomes.1516 In addition to our current study results, it is important to identify long-term possible consequences of COVID-19 on the PPM project in Korea, such as (1) increased number of TB mortalities, LTFU, and treatment failure cases during the COVID-19 pandemic, (2) increased proportions of retreatment cases among all notified TB cases within one or two years, and (3) increased number of notified TB cases after COVID-19.
In conclusion, major disruptions such as natural disasters, war, and infectious disease pandemic have led to an increased burden of TB. The COVID-19 pandemic had enormous potential to hinder the efforts of TB services in prevention, case detection, and management, particularly in resource-limited settings.17 Our study showed that initial TB management amid the COVID-19 pandemic was properly managed under the national PPM TB control project in Korea. However, our study cannot confirm a decreased treatment success rate after the COVID-19 pandemic due to limited data. In addition, interventions such as TB contact investigation and preventive therapy may have been deprioritized and delayed during the pandemic. Further research studies are necessary to assess the potential effects of COVID-19 on TB prevention and control in many different ways and to confirm our results.
 XML Download
XML Download