

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
With the rising numbers of older adults and hospitalized patients, continued management of the patient after discharge and the prevention of rehospitalization have become important issues. Older inpatients spent 26 trillion KRW on medical expenses in 2018.1 The prevalence of rehospitalization for patients over the age of 65 was 12.2%, while, patients under the age of 65 had a rehospitalization rate of only 8.2% in 2013.2 Hospital-associated deconditioning of older adults often results in the experience of difficulties in performing activities of daily living (ADLs) and developing various complications, such as atelectasis, pneumonia, acute delirium, and depression.3 Frailty is a common occurrence in older adult patients after discharge, with increasing risk within 1 month. The condition can cause socioeconomic burden and reduction of quality of life.34
Optimal hospital discharge planning considers the appropriate equipment, home modifications, information about the utilization of medical resources, and education on self-care for older adults and their caregivers that can promote independent functioning and reduce safety risks after discharge.5 Transitional care encompasses a broad range of services and environments designed to promote the safe and timely transition of patients between levels of health care and across care settings.6 The World Health Organization explains that “transitions of care” occur at “the various points where a patient moves to, or returns from, a particular physical location or makes contact with a health care professional,” including the home, hospital, and residential care facility.7 Recently, the Korean Ministry of Health and Welfare established a nationwide system for the cooperation of essential medical care in local communities and institutionalized transitional care.8 In 2020, a dedicated team of doctor, nurses, and social workers from 27 public medical hospitals across the country was set up to implement transition care.8
Several studies have demonstrated that home visits or phone calls after discharge may aid older adults in meeting their health care needs.910 However, one Dutch study found that home visits after discharge did not appear to have any effect in older adults with poor health status.11 A systematic review of 8 studies in Western countries showed similar results.12 However, the effect of transitional care is relatively unknown except in Western countries, and the effect of transitional care in the medical environment in Korea is not yet known. Furthermore, because the relationship between hospitals and community care organizations tends to be different according to medical policy and is in most cases fragmented, it is difficult to apply the results of studies from other countries without first having a detailed understanding of the situation in Korea.13
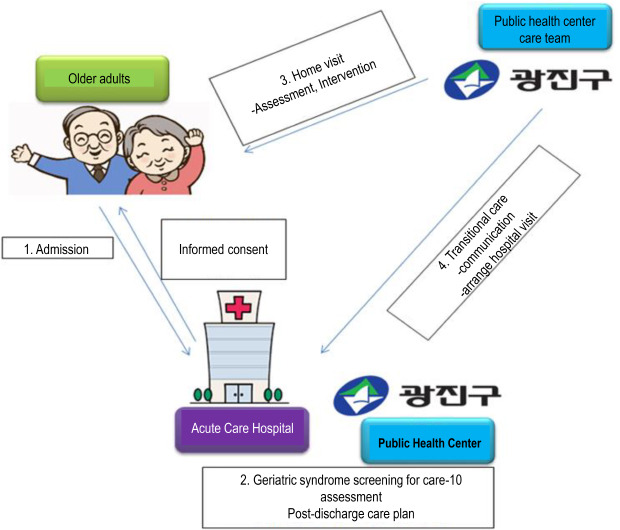
In Korea, there is currently no system to assess and manage the overall health status of older adult patients who have been discharged from the hospital. Recently, the concept of “being citizen-oriented” was introduced in Korea as a framework for providing customized services. A senior-specific, citizen-oriented healthcare service system was first implemented in our acute care hospital in 2017.14 The older inpatients were connected to a public health center for continued care at home after discharge. We have signed an agreement with the Gwangjin-gu Public Health Center (Seoul, Korea) for transitional care of older adult patients who have been discharged from our hospital.
The present study aimed to describe the experience of providing older adult patients with transitional care from an acute care hospital to home in cooperation with a public health center, to present the barriers to that care and suggest better organizational methods.
METHODS
Study participants
This study included participants who were hospitalized patients, aged 65 years or above living in the Gwangjin-gu district. Eligibility for transitional care from a public health center was determined by residency. Among the 659 patients who were admitted to the general ward of an acute care hospital in Seoul between June 24, 2019, and January 23, 2020, 45 were finally analyzed after excluding 614 based on the following exclusion criteria: 1) Persons with a severe disease such as cancer treatment, regular dialysis, or inability to communicate (n = 209) that were unable to participate in a general health care program through a public health center, and death (n = 1). 2) The patient declined participation in the program (n = 202). 3) The patient was unable to complete the inpatient assessment due to his or her treatment plan (n = 145). 4) The patient was already registered in a health care program at a public health center, as a member of a vulnerable group (n = 57). In Korea, since 2007, individuals aged 65 years and above who are members of vulnerable groups, in terms of socioeconomic and health status, have received healthcare management through the home visiting health service programs of public health centers.15 A transitional care plan containing the treatment summary, the results of the Geriatric Screening for Care-10 (GSC-10) assessment, and post-discharge plan, and official documents applied with information security were delivered to the representative of the public health center by e-mail. The hospital communicated with the center for the transitional care plan weekly. A visiting nurse called first to confirm the consent of participation and to adjust the visiting schedule. If older patients needed medical consultation or emergency treatment during this service, the visiting nurse informed the transitional care team. There were no additional costs to patients for this service. Training for all visiting nurses in the public health center was conducted to increase the understanding of transitional care (assessment, physical rehabilitation, etc.) by the medical staff of acute care hospital twice a year.
Measurements
Geriatric syndrome screening for care (GSC) has been performed for all older adult inpatients aged 65 years or above within 48 hours of hospitalization regardless of the reason for hospitalization. The aims of geriatric syndrome screening with the GSC-10 is to detect the risks of functional deterioration and the loss of independence at home after discharge. The GSC-10 are as follows: cognitive impairment, delirium, depression, polypharmacy (more than 5 medications), functional immobility, dysphagia, malnutrition, pain, urinary, and fecal incontinence, which were developed from the literature review, benchmarking, focus group interviews, and expert consultation.14 The GSC-10 was based on proven associations with readmission for older inpatients and mobility decline.1617 Patients with problematic issues are referred to a multidisciplinary team that performs a comprehensive consultation. Within 48 hours of the patient's admission, an attending nurse who had been designated at admission administered the GSC-10 assessment to the patient. The nurse also re-administered the assessment before discharge (Supplementary Table 1). The assessment using GSC-10 was able to be completed within five minutes by electronic health records. In the assessment of functional mobility, “requires assistance” and “unable to perform” were categorized as functional immobility. Malnutrition was defined as a score of more than 2 on the malnutrition screening test, weight loss in the past 6 months (yes: 1, no: 0), and decreased appetite (yes: 1, no: 0). The presence of cognitive impairment, depression, delirium, polypharmacy (5 or more medications), dysphagia, and incontinence in the past month was relevant when participants responded “yes.” A numerical pain score greater or equal to 4 was also relevant.
We classified the results of the transition from hospital inpatient care to public health center services as follows: attending interventions and delay in transition to home because of hospitalization in a nursing hospital or nursing home. We calculated days from discharge to request for transition, and from request for transition to contact with the participant at home. We obtained data on age, sex, cause of hospitalization, hospital stay, comorbidities, and type of medical insurance from patient medical records.
We investigated the contents of the care provided by the public health center, which were as follows: hospitalized disease management, chronic disease care and prevention (including glucose and blood pressure monitoring), nutritional support (i.e., the provision of nutritious porridge), education on physical activity and fall prevention, participation in frailty care for 8 weeks, physical rehabilitation programs, and enhancement of cognitive function, and others (e.g., refer to the mood management team, Foley catheter care, oral health care, and smoking cessation). We assessed all interventions that had been applied. Finally, we investigated the reasons for the refusal of transitional care after discharge.
Statistical analysis
Descriptive statistics of the study participants, results of the GSC-10 assessment, and transition outcomes, such as the length of time and contents of provided care, were expressed as mean values ± standard deviation for continuous variables and as numbers (proportion) for categorical variables in a cross-sectional study design. Because a lot of patients were initially excluded, we performed the comparisons of final participants (n = 45) and non-participants who withdraw after agreeing to participants (n = 26) using the Fisher's exact test (Supplementary Table 2). All statistical analyses were performed using IBM SPSS Statistics for Windows, version 24.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Characteristics of the study population
The process of selecting subjects for this study has schemed in Fig. 1. The mean age of the participants was 76.2 years (range, 65–90 years). Of all the participants, 51.1% were females (Table 1). The most common cause of hospitalization was bone and musculoskeletal disease (37.8%). The mean hospital stay was 18.6 days. The most common comorbidity was hypertension, and the percentage of participants with a history of any type of surgery was high (62.2%). Most of the participants had general health insurance (93.3%).
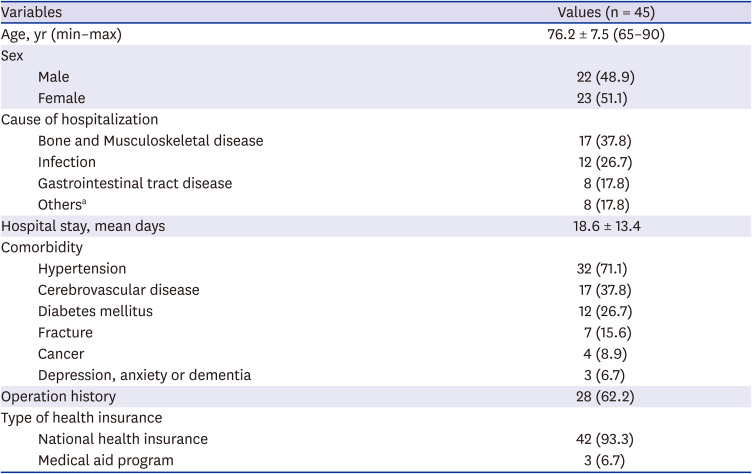
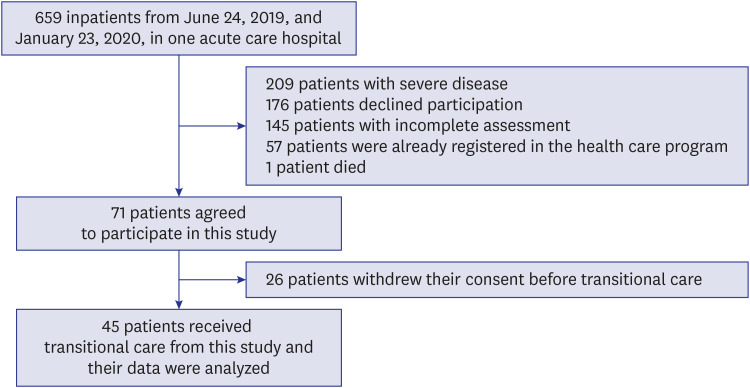
Table 1
The characteristics of study participants
Data are presented as mean ± standard deviation or number (%).
aCerebrovascular disease, hepatobiliary tract disease, renal disease and gynecologic disease.
![]()
Results of the GSC-10 assessment
Of all the participants, 64.4% had more than one of the GSC-10 concerns (Table 2). Among the GSC-10 domains, functional immobility was found to be the most prevalent problem (35.6%). The second most prevalent problem was polypharmacy (22.2%). In general, the study population did not have any significant problems in the remaining domains.
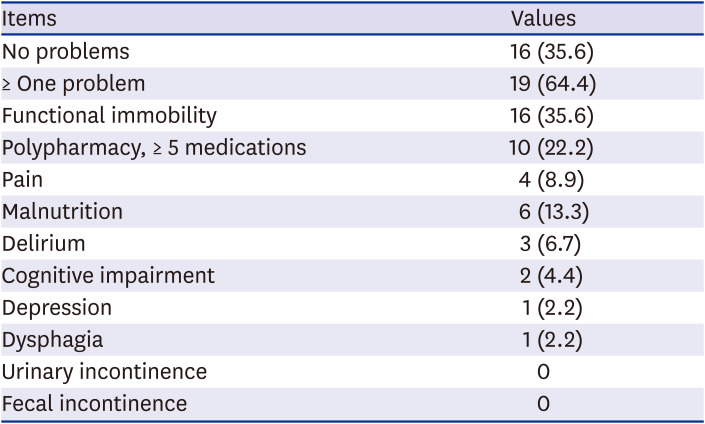
Table 2
The results of geriatric syndrome screening for care (n = 45)
![]()
Outcomes of transitional care
Among 45 participants, 7 patients (16%) were readmitted to a nursing home or hospital. A total of 38 participants received the transitional care intervention (Table 3). The mean time from discharge to request for the transition was 8.0 days, and the mean time from request for transition to contact with the participant was 8.5 days. The average length of time between discharge and a home visit was 16.5 days. Multiple contents of the care were provided (102 administered interventions/38 participants, the mean number of administered interventions per participant: 2.68). The most frequent content of the care was to manage the hospitalized disease. In addition, chronic disease care, nutritional support, and education on physical activity and fall prevention were the main services provided. Seven of the 38 cases are described in detail in Supplementary Table 3.
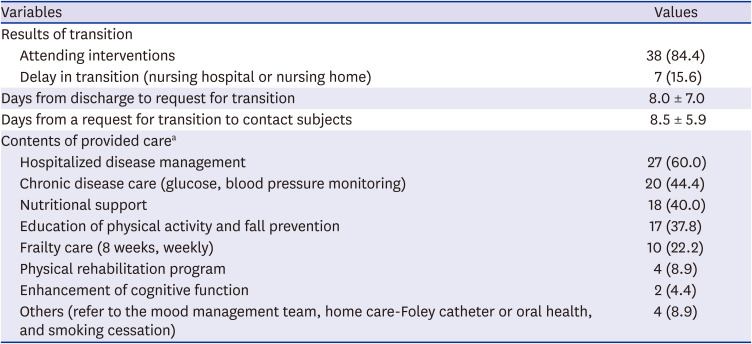
Table 3
Outcomes of transition care with managing by a public health center (n = 45)
![]()
Barriers faced by nurse practitioners and patients' reasons for refusing transitional care services
Patients' reasons for refusing transitional care services at the time of requesting consent and applying transitional care services are described in Supplementary Table 4. The major reason was that the patient felt that he or she did not need the services (64.2%) and the patient still participated in economic activities or that he or she did not have much time at home (26.7%) at requesting consent. Uncomfortable from a stranger's visit (30.8%), not wanting to provide their personal information to others (23.1%), and no need for the services (23.1%) were the reasons for refusal before applying transitional care services.
DISCUSSION
This study described the experience of providing older adult patients with transitional care from an acute care hospital to home in cooperation with a public health center. We conducted a comprehensive geriatric screening during hospitalization (using the GSC-10) and designed a post-discharge plan for each patient that included a treatment summary, medication list, and plans for further care based on the current health status of the participant. Then a public health center provided personalized care (using previously operated interventions) or home visiting care by a nurse practitioner. In addition to hospitalized disease management, various interventions were administered based on each patient's individual needs. To our knowledge, our study was the first to explore continued individual health care after discharge for older adult patients, through assessment of their overall health condition and hospitalization-related illnesses. Although only for a short period of time, we evaluated the usefulness of the GSC-10 in transitional care.
Among the various domains of the GSC-10, immobility was the most prevalent disability of the study participants, similar to a US study.18 Low mobilization during hospital stays is a common phenomenon; up to 83% of an older adult patient's time is spent lying in bed.1920 Decreased levels of mobility during hospitalization or preadmission can lead to functional decline after discharge.19 One previous study found that among older adults who had low levels of mobility during hospitalization, 86% had declines in ADLs at discharge, and 73% in ADLs, and 63% in instrumental ADLs at 1 months' follow-up.19 Disability in walking or moving requires the patient to have support of another person or an instrument.
Polypharmacy is also a common health problem in older adult patients who have been discharged from the hospital. It is closely associated with frailty, falls, and functional decline.21 Although we did not survey the specific names of the prescribed medications, one previous study reported that the most common medications were analgesics and antiulcer medications.21 This finding was due to the large number of patients hospitalized for fractures or orthopedic disorders. The patients in our study were expected to have a high frequency of being prescribed these drugs because they had similar diseases. Therefore, regular medication reviews should be performed. Analgesics and antiulcer medications can be stopped if symptoms improve. A time of discontinuation can be set through coordination with the public health center.
Home-based health management of older adults has been performed by visiting nurse practitioners from outreach community health services in Korea since 2015.15 The public health center is able to provide care and prevention services for both chronic and acute diseases, including nutritional support, rehabilitation services, and exercise assistance. Because these health services were supplied by the public health center as available resources of this transitional care model, there were no additional costs. As the GSC-10 assessment identified their needs of the subjects, transitional care including total health care management could be carried out extensively.
However, our study was able to identify some of the major problems that may be encountered in the implementation of transitional care in Korea. First, the percentage of people who wanted to participate was low. Many older adult patients initially reject transitional care services that they did not need. It may be that transitional care was unfamiliar to them because few other hospitals offered it. Participants responded that they could not receive home visiting care because they were engaged in economic activities or spent much of their time outside. In such cases, transitional care may not be required because it is likely that there are no health care vulnerabilities. Even about 36% of the participants of this study had no problems in the assessment of GSC-10. For this reason, the rate of rejection may be high in this study. To increase the participation rate of transitional care, appropriate criteria are needed to select the subjects for transitional care application, like inpatients with any concerns of GSC-10. Additionally, it is necessary to develop the contents of the service that can meet the needs of the subjects.
Second, of the patients who had initially agreed to receive transitional care services, several patients eventually withdrew their consent. The most common reason was that they were uncomfortable with the idea of receiving a stranger's visit, even if he or she visited as a health manager. Even though we did not produce the statistics, some patients could not decide whether to accept a health manager's visit and asked or took advice from their family members. Those who responded in this manner may actually need transitional care. Therefore, we need to come up with a plan that will not burden the health manager's visit. Digital health including mobile health, wearable device, telehealth, and telemedicine may be an alternative,22 but it is difficult to use in older adults, and the effect of the previous study has not been confirmed,23 so further research will be needed.
Third, it took an average of 16.5 days for new health services to be applied after patients had been discharged from the hospital. It was longer than in other studies (24 hours–2 weeks).2425 If the intervention is made long after discharge, the frequency of rejection may be high and outcomes may be affected. The reason for the long period of time before patients were contacted was that a small number of medical staff had been in charge of the transitional care process while also carrying out their other duties. Therefore, it is important to establish a connecting system that can deliver a care plan with medical staff whose primary duties include transitional care services. In the Australian enhanced primary care initiative, if the response had not been returned by the general practitioner within 24 hours, follow-up by the designated nurse of the hospital was performed.25 Therefore, it is necessary to keep track of the progress of the service in acute care hospitals. In addition, a study will be needed to confirm the proper timing of the transitional care after discharge.
In order for transitional care after discharge in older adult patients to be implemented smoothly, all medical staff must agree on the need for the service, evaluate the patient's current health status in terms of geriatric syndromes, and communicate with one another. Sharing medical records through electronic health records would be a helpful practice in large hospitals. A professional care manager could be responsible for developing the post-discharge care plan and for coordinating the efforts of hospital staff and community care staff in providing long-term care services, similar to the Japanese model.26 In addition, we hope to diversify the health care services of the public health center to apply according to the severity of the older adult's health status. In this study, patients with serious illness were excluded initially, because there was no suitable service or lack of training for visiting nurses. Additionally, we hope to organize the designated multidisciplinary team of acute care hospitals and public health centers so that the services can be tailored to match patients' individual needs. If this model of transitional care expands in conjunction with the government's health management plan, it will be able to be established successfully.26
This study had several limitations. First, there may have been bias in the selection of target patients because a lot of candidates were excluded and there was a high rejection rate. We excluded patients with severe diseases such as acute myocardial infarction or cancer with uncontrolled symptoms. The reason for excluding these patients was that visiting nurses who care for these patients experience more burden of care. We also considered a previous finding that home visiting programs have no effect on older adults with poor health in a previous study.1227 Because the same nurse practitioner worked for both this study and a health care program for vulnerable community-dwelling older adults, patients who were already registered in the health care program were excluded from this study. Second, there can be a variety of transitional care models, depending on whether the patient goes home or to another hospital after discharge. Because we collaborated with only 1 public health center, our findings cannot be generalized to other settings or to non-senior patients. Third, we could not measure outcomes of transitional care such as hospital readmission,28 visits to emergency departments,29 the quality and safety of care,30 or the cost-effectiveness of reducing healthcare costs.31 Although we have presented fragmentary results to share our experience, and the effect of the intervention should be interpreted keeping the results of previous studies in mind,28293031 we have set up a framework of transitional care for older adult Korean patients. In the future, we will attempt to involve more hospitals and to apply the intervention to more patients for a longer period of time.
In conclusion, we implemented a transitional care model from an acute care hospital to home for patients aged 65 years or older, in cooperation with a public health center, and found several barriers from this experience. More research in various medical settings with target patients should be conducted in order to develop a transitional care model that matches the Korean medical situation.
 XML Download
XML Download