

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
β-blockers (BBs) constitute a cornerstone of therapy in patients with chronic heart failure (HF) with reduced ejection fraction (HFrEF) based on the results of landmark trials.12 According to both European and American guidelines, the use of BBs in symptomatic patients with HFrEF has a class 1A recommendation.12 Nonetheless, there is a suboptimal utilization of recommended medications in patients at the greatest risk of death who are least likely to receive evidence-based therapy.3 BBs have not been fully evaluated in clinical trials, and there have been concerns regarding treatment efficacy, particularly in patients with acute decompensated HF, atrial fibrillation (AF), and HF with preserved ejection fraction.
Acute heart failure (AHF) is a life-threatening medical condition with high inpatient mortality (typically > 4%).4 However, evidence supporting the benefits of BB treatment (reduced mortality) in AHF is lacking and there are concerns about the negative inotropic effects of BBs; thus, the potential worsening of hemodynamics leads many physicians to stop BB treatment in AHF. The same concern about the beneficial effect of BB has been conclusively demonstrated to be inappropriate with regard to chronic HF management.567 On the other hand, AF is common in patients with HF because the pathophysiology and risk factors for HF and AF are closely associated.8 Furthermore, patients with concomitant HF and AF have significantly poorer prognoses.9 Although BBs are widely used in AF with and without HF as first-line control therapy, a recently performed meta-analysis of key BB randomized control trials (RCTs) involving chronic stable HFrEF patients showed that BBs were not effective in reducing all-cause mortality in patients with AF, but were effective in patients with normal sinus rhythm (NSR).101112 In addition, no treatment to date has convincingly reduced morbidity or mortality in patients with HF with preserved ejection fraction (HFpEF) especially when combined with AF.13 Previous analyses in these patient subsets have lacked statistical power. Thus, the present study assessed whether BBs prescribed at discharge could improve prognosis in AHF patients with AF in a large nationwide prospective cohort.
METHODS
Study population
The Korean Acute Heart Failure (KorAHF) study is a multicenter prospective cohort study that enrolled 5,625 consecutive patients who were hospitalized for AHF at 10 tertiary university hospitals between March 2011 and February 2014. Detailed information on the study design and the results of the KorAHF registry has been provided previously.14 Briefly, the registry included patients with signs or symptoms of HF who met at least one of the following criteria: 1) lung congestion or 2) objective findings of left ventricular (LV) dysfunction or structural heart disease. From this population, we selected patients with HF and AF who had survived hospitalization with available 1-year follow-up data.
Study variables and clinical outcomes
HFrEF was defined as left ventricular ejection fraction (LVEF) < 40% and HFpEF as LVEF ≥ 50%.2 AF was confirmed with 12-lead electrocardiography at admission or during hospitalization. Patients who received only guideline-recommended BBs, including bisoprolol, carvedilol, sustained-release metoprolol succinate, and nebivolol at discharge, were considered as BB-treated.12 Patients not eligible for BB therapy whose systolic blood pressure was < 90 mmHg or resting heart rate was < 50 bpm at discharge were excluded.2 In this study, the outcomes were defined as 60-day and 1-year all-cause mortality, rehospitalization because of aggravated HF, and a composite endpoint of mortality and HF rehospitalization. The attending physician collected follow-up data through a web-based case report form. The outcome data for subjects who were not followed up were ascertained by a telephone interview and confirmed from the National Death Records. All clinical events were monitored and verified by a Clinical Event Committee, comprising independent experts on HF who did not participate in patient enrollment for the study.14
Statistical analysis
Statistical analyses were conducted by the Center of Biomedical Data Science, Yonsei University, Wonju College of Medicine. Propensity score (PS) analysis was used to account for selection bias of BB prescription when assessing the association. The variables selected for the score were age, sex, body mass index, systolic blood pressure, heart rate at admission, history of hypertension, ischemic heart disease, chronic lung disease, chronic kidney disease, LVEF and other discharge medications including angiotensin converting enzyme inhibitor (ACEi), angiotensin-receptor II blocker (ARB), mineralocorticoid receptor antagonists (MRA), and anticoagulants. BB-treated and -untreated patients were then matched 1:1 using the nearest neighbor method with caliper < 0.01 and no replacement. Continuous variables were reported as mean ± standard deviation and were compared with the independent t-test. Categorical variables were presented as frequencies and percentages and were compared using the χ2 test. Individual and composite clinical outcomes were analyzed based on time to the first event. Kaplan-Meier survival curves were plotted, and the groups were compared using the log-rank test. To assess the relationship between outcomes and use of BBs, Cox proportional hazards regression models were used and adjusted for sex, age, history of hypertension, diabetes mellitus, ischemic heart disease, chronic obstructive pulmonary disease, and systolic blood pressure. The models also adjusted for heart rate, serum sodium levels, hemoglobin levels, creatinine levels, LVEF, discharge medication including ACEi or ARB, MRA and anticoagulation in the matching cohort. The proportional hazards assumption was confirmed using log (-log) survival plots and time interaction terms. In all cases, a P value < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS Version 23.0 (IBM, Armonk, NY, USA).
Ethics statement
The study protocol was approved by the Institutional Review Boarad at each hospital and the Wonju Christian Hospital, Wonju College of Medicine, Yonsei University (Approval No. CR311003), and written informed consent was obtained from each patient or their relative or legal representative.
RESULTS
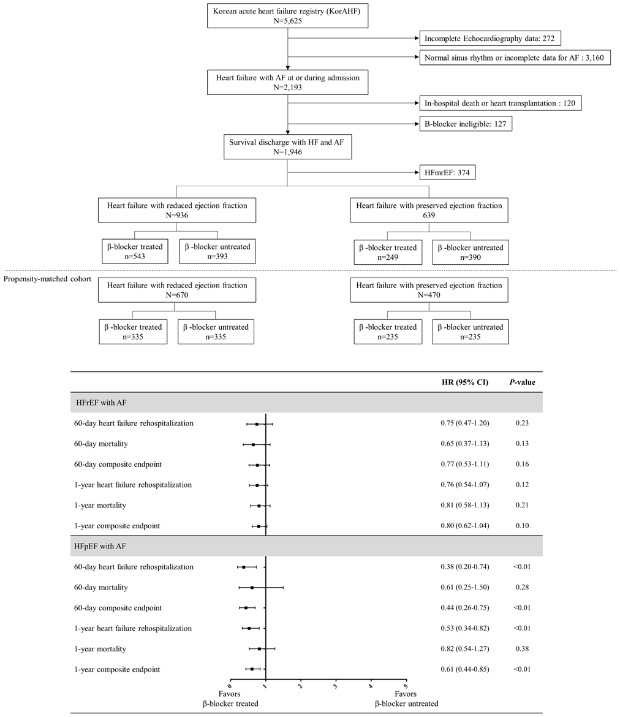
The number of AF patients eligible for BB therapy was 1,946 out of the 5,625 patients in the KorAHF registry. In addition, among these HF patients with AF, 936 were diagnosed HFrEF and 639 were HFpEF. BB was used in 543 (58%) patients with HFrEF and in 249 (40.0%) with HFpEF. After PS matching, the analysis was restricted to 1,140 patients: 670 HFrEF and 470 HFpEF.
Baseline characteristics and medication at discharge of HFrEF and AF
In HFrEF patients with AF, the median age of the cohort was 71 (interquartile range [IQR], 61–78) years and 62.1% were males. BB-treated and BB-untreated patients differed with regard to most of the baseline characteristics (Table 1). Patients who did not receive BBs were older, had a lower body mass index and diastolic blood pressure, different pattern of comorbidities (more likely chronic kidney disease and obstructive pulmonary disease), different etiology of HF, and laboratory characteristics (lower levels of sodium and hemoglobin and lower ejection fraction). At discharge, other pharmacological therapies including ACEi and MRA were less frequently prescribed in BB-untreated patients (Supplementary Table 1). After PS matching, there were no statistically significant differences in baseline characteristics between BB-treated and BB-untreated patients, except in left bundle branch on the electrocardiogram and serum sodium levels (Table 1).
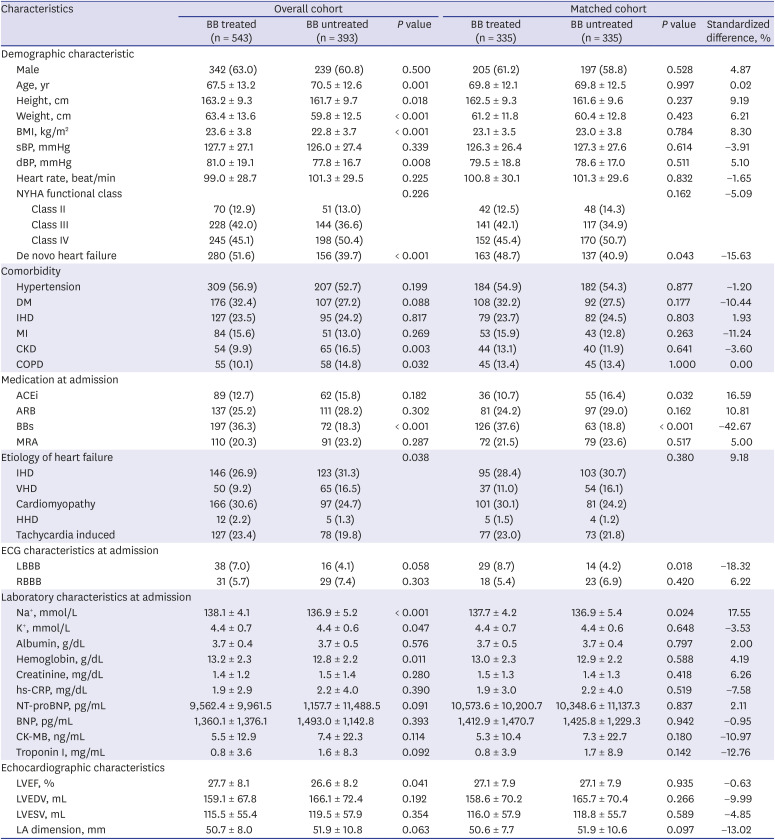
Table 1
Baseline characteristics of patients with heart failure with reduced ejection fraction and atrial fibrillation according to the use of β-blockers
Values are presented as numbers (%) or mean ± standard deviation. unless otherwise indicated.
BBs = β-blockers, BMI = indicates body mass index, sBP = systolic blood pressure, dBP = diastolic blood pressure, NYHA = New York Heart Association, DM = diabetes mellitus, IHD = ischemic heart disease, MI = myocardial infarction, CKD = chronic kidney disease, COPD = chronic obstructive pulmonary disease, ACEi = angiotensin converting enzyme inhibitor, ARB = angiotensin-receptor II blocker, MRA = mineralocorticoid receptor antagonists, VHD = valvular heart disease, HHD = hypertensive heart disease, ECG = electrocardiography, LBBB = left bundle branch block, RBBB = right bundle branch block, hs-CRP = high-sensitivity C-reactive protein, NT-proBNP = N-terminal pro-brain natriuretic peptide, BNP = B-type natriuretic peptide, CK-MB = Creatine kinase-MB, LVEF = left ventricular ejection fraction, LVEDV = left ventricular end-diastolic volume, LVESV = left ventricular end-systolic volume, LA = left atrium.
![]()
Baseline characteristics and medication at discharge of patients with HFpEF and AF
In HFpEF patients with AF, the median age of the cohort was 76 (IQR, 69–82) years and 36.8% were males. BB-untreated patients differed from the treated patients with regard to most of the baseline characteristics, as described in HFrEF (Table 2). BB-untreated patients had lower diastolic blood pressure, more likely hypertension, different etiologies of HF, and laboratory characteristics (lower levels of sodium, hemoglobin, left atrial dimension, and higher prevalence of left bundle branch block). At discharge, the prescription rate of other medication was not different between the groups (Supplementary Table 2). After PS matching, there were no statistically significant differences in baseline characteristics between BB-treated and BB-untreated patients, except in the etiology of HF and prevalence of left bundle branch block (Table 2).
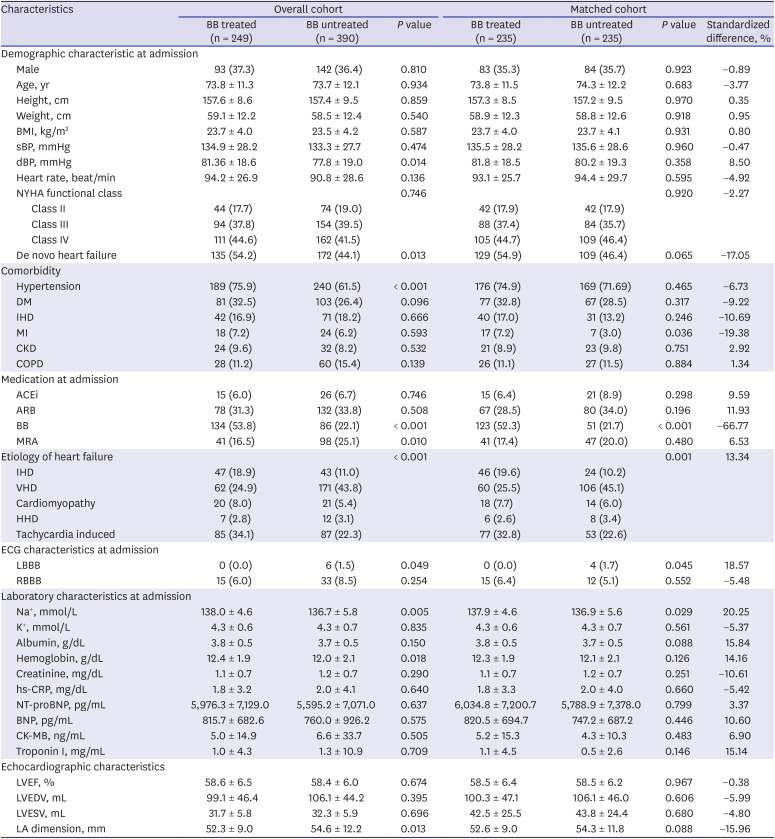
Table 2
Baseline characteristics of patients with heart failure with preserved ejection fraction and atrial fibrillation according to the use of β-blockers
Values are presented as numbers (%) or mean ± standard deviation, unless otherwise indicated.
BB = β-blockers, BMI = indicates body mass index, sBP = systolic blood pressure, dBP = diastolic blood pressure, NYHA = New York Heart Association, DM = diabetes mellitus, IHD = ischemic heart disease, MI = myocardial infarction, CKD = chronic kidney disease, COPD = chronic obstructive pulmonary disease, ACEi = angiotensin converting enzyme inhibitor, ARB = angiotensin-receptor II blocker, MRA = mineralocorticoid receptor antagonists, VHD = valvular heart disease, HHD = hypertensive heart disease, ECG = electrocardiography, LBBB = left bundle branch block, RBBB = right bundle branch block, hs-CRP = high-sensitivity C-reactive protein, NT-proBNP = N-terminal pro-brain natriuretic peptide, BNP = B-type natriuretic peptide, CK-MB = Creatine kinase-MB, LVEF = left ventricular ejection fraction, LVEDV = left ventricular end-diastolic volume, LVESV = left ventricular end-systolic volume, LA = left atrium.
![]()
Association between BB use and outcomes for patients with HFrEF and AF
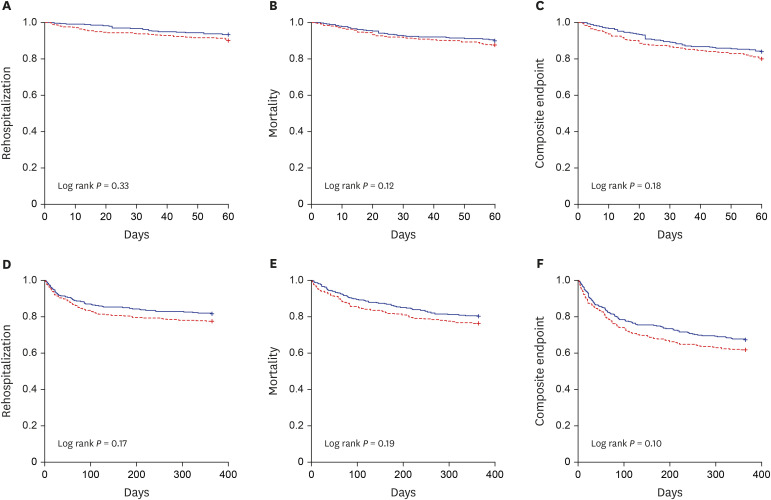
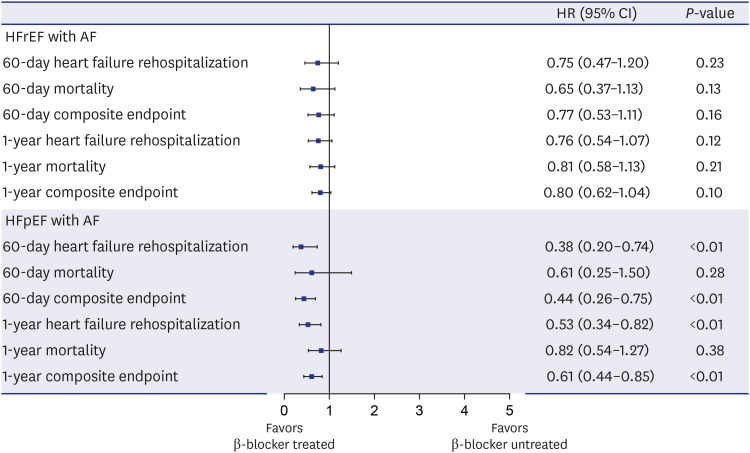
At discharge in the matched cohort, the heart rate was significantly lower in BB-treated patients (75.3 ± 14.4 bpm vs. 78.5 ± 13.7 bpm, P < 0.01) and systolic blood pressure at 1-year follow up was lower in BB-treated patients (113.5 ± 16.4 mmHg vs. 117.6 ± 16.6 mmHg, P < 0.01) (Supplementary Table 3). In the overall cohort of HFrEF patients, 187 (20%) patients died from any cause and 184 (19.7%) were hospitalized due to worsening HF. All clinical events occurred more frequently in BB-untreated patients except 60-day rehospitalization (Supplementary Table 4); however, after PS matching, there was no difference in clinical outcomes (Supplementary Table 4). Event-free survival was not different according to the use of BB (Fig. 1), and after adjusting for covariates in the multivariable Cox model of matching cohort, there was no association between BB treatment and all clinical outcomes at the 60-day and 1-year follow up (Fig. 2). This statistical significance did not change after including digoxin and amiodarone at discharge as covariates (Supplementary Table 5).
In an exploratory subgroup analysis for 1-year rehospitalization and mortality, no significant interactions were observed at clinical cutoffs for variables, including age, sex, history of hypertension, diabetes mellitus, ischemic heart disease, myocardial infarction, chronic obstructive lung disease, type of HF, heart rate at admission and at discharge, as well as concomitant use of digoxin and amiodarone. However, in the subgroup of patients who had a history of myocardial infarction, the rate of rehospitalization (HR, 0.34; 95% CI, 0.13–0.88) and mortality (HR, 0.17; 95% CI, 0.06–0.49) was significantly lower in BB treated patients (Supplementary Fig. 1).
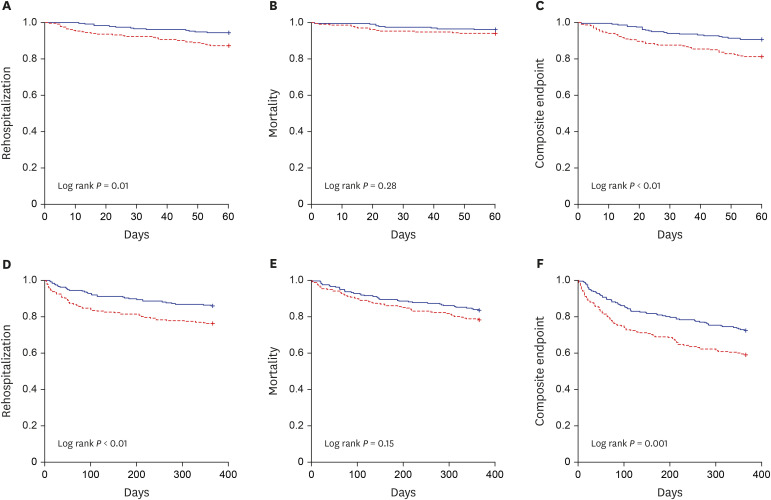
Association between BB use and outcomes for patients with HFpEF and AF
Heart rate was significantly lower in BB-treated patients at discharge and 1-year follow up (74.9 ± 13.1 bpm vs. 79.0 ± 13.9 bpm, P = 0.001) (76.7 ± 15.9 bpm vs. 82.5 ± 19.4 bpm, P = 0.01) (Supplementary Table 3). In the overall cohort of HFpEF patients, 123 (19.2%) patients died and 123 (19.2%) were rehospitalized. BB-untreated patients were more frequently hospitalized at the 60-day (12.3% vs. 5.2%, P < 0.01) and 1-year follow up (13.3% vs. 23.1%, P < 0.01), but mortality was not different (Supplementary Table 6). In addition, the 60-day and 1-year rehospitalization free survival rates were more favorable in BB-treated patients (Fig. 3). After PS matching, the higher occurrence of 6-month and 1-year rehospitalization in BB-untreated patients was also confirmed (Supplementary Table 6), while rehospitalization-free survival during the 6-month and 1-year follow-up was higher in BB users (Fig. 2). Furthermore, in the multivariable Cox model of the PS-matched cohort, BB use was associated with reduced 6-month (HR, 0.38; 95% CI, 0.20–0.74) and 1-year rehospitalization (HR, 0.53; 95% CI, 0.34–0.82). Because of reduced rehospitalization, BB use was associated with reduction of 6-month and 1-year composite endpoint (Fig. 2). This statistical significance also did not change after including digoxin and amiodarone at discharge as covariates (Supplementary Table 5). In a subgroup analysis for 1-year rehospitalization, there was significant interaction in patients with concomitant use of digoxin (P for interaction = 0.03). For 1-year mortality, significant interaction was observed for age (P for interaction = 0.03) (Supplementary Fig. 2).
DISCUSSION
Our analysis showed that there was no significant implication of BB on 60-day and 1-year clinical outcomes in HFrEF patients with AF. However, the use of BB in HFpEF with AF was associated with reduced rehospitalization rates at 6- month and 1-year follow up.
BBs and outcomes in HFrEF with AF
Evidence-based benefits, including reduced ejection fraction (HFrEF) and NSR, of guideline-directed therapy for HF have been documented but there are limited and conflicting data regarding the prognostic implications of guideline-directed therapy for HFrEF patients with AF. In our previous study, a higher level of adherence to guidelines was associated with better 60-day and 1-year prognoses in HFrEF patients with AF.15 The current guideline recommends BBs as a cornerstone therapy of HFrEF and it is based on clinical trials that demonstrated an improvement in clinical outcomes in HF patients. However, RCTs examining the efficacy of BBs in HF patients with concomitant AF, especially patients admitted to hospital with AHF, are scarce. Meta-analysis studies and cohort data have reported the efficacy of BBs in HFrEF patients with AF but results are conflicting. A recent meta-analysis evaluating the use of BBs in HFrEF patients with AF documented that BBs did not reduce mortality in HF patients with AF.111216 Additionally, in a meta-analysis of four RCTs evaluating HFrEF with AF, BB showed reduced mortality in NSR (HR, 0.63; 95% CI, 0.54–0.73; P < 0.001), but did not reduce mortality in AF patients (HR, 0.86; 95% CI, 0.66–1.13; P = 0.28).11 In another meta-analysis using individual-patient data, BB therapy did not lead to a significant reduction in all-cause mortality in patients with AF (HR, 0.97; 95% CI, 0.83–1.14; P = 0.73).12 In contrast to these meta-analyses, cohort studies have reported positive results for BBs. In the report from the Swedish Heart Failure Registry, BBs showed a protective effect on mortality (HR, 0.71; 95% CI, 0.61–0.84; P < 0.001).17 In the Danish nationwide cohort, evidence of a lower mortality with BB therapy was observed in the PS-matched analysis (HR, 0.75; 95% CI, 0.71–0.79).18
Although the exact reason is not clear in this study, there are several possible explanations for the conflicting results of the effects of BB therapy in HFrEF patients with AF. First, there are several mechanisms for the beneficial effects of BBs. One of the most important is the reduction of the heart rate and not a blockage of central sympathetic outflow.19 In HFrEF with NSR, lower heart rate has a better outcome with or without BBs.1620 However, heart rate has no prognostic implications in patients with AF.1620 Patients with AF may need a higher heart rate to maintain a similar cardiac output; higher heart rate might be needed during HF. Further, a low heart rate in AF may be an expression of an underlying conduction disorder, which itself may be associated with impaired outcome.11 Second, AF in patients with HF may be a marker of a poorer clinical condition, leading to a worse outcome that is less modifiable by BB therapy.21
BB and outcomes in HFpEF with AF
Evidence that BBs improve symptoms is conflicting in HFpEF patients even with NSR.13 In a recent individual patient meta-analysis, BBs were effective in HFrEF but not in HFpEF patients with NSR or AF.22 Though the exact mechanism for the lack of positive prognostic effect of BBs in patients with HFpEF is not known, there is a possible explanation. In the pathophysiological view, the beneficial effect of BBs is mediated by a reduction of the resting heart rate in NSR. The hemodynamic effects of acute change of heart rate in patients with HFpEF have been reported to be different compared with those in patients with normal ventricular function.23 Increasing heart rate decreased LV end-diastolic pressure strikingly, while end-diastolic, end-systolic, and stroke volumes all declined. These hemodynamic effects were similar in the groups with and without BBs.23 Further, because LV end-diastolic pressure declines substantially with heart rate elevations in HFpEF, it is likely that slowing the resting heart rate will raise filling pressures. Because increases in the heart rate in patients with HFpEF were associated with LV volume reductions that resulted in a blunted heart rate—cardiac output relationship, slowing of the resting heart rate may modestly reduce the cardiac output. This, along with increased filling pressures, is obviously undesirable in patients with HFpEF and suggests that higher resting heart rate provides hemodynamic benefits.24 No study has been conducted on chronic resting heart rate elevation in HFpEF. In the RACE II trial (Rate Control Efficacy in Permanent Atrial Fibrillation: a Comparison Between Lenient Versus Strict Rate Control II) including a high proportion of cases with hypertensive heart disease and diastolic dysfunction, a more lenient heart rate control strategy of up to 110 per minutes was non-inferior to strict control strategy.25 This could provide the clue that different significance of HR in HFpEF especially combined with AF.
However, there were some studies reporting contradictory results for the association between heart rate and prognosis in HFpEF. The data from the OPTIMIZE-HF (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure) registry reported that heart rate <70 beats/min was also associated with a lower risk for the combined endpoint of HF readmission or all-cause mortality (HR, 0.90; 95% CI, 0.84–0.96; P = 0.002).26 Recently the data based on the Swedish Heart Failure Registry demonstrated that higher heart rate was associated with increased mortality during the initial years of follow-up in HFpEF with AF.27 In a large-scale cohort study, BB was associated with reduced mortality (HR, 0.93; 95% CI, 0.86–0.996; P = 0.04).28 Although the exact reason is not clear in this study, BB was associated with reduced 6-month and 1-year rehospitalization. There can be several hypotheses. First, HFpEF might be over diagnosed in patients with HFpEF and AF because symptoms might reflect AF alone. BBs could have reduced symptoms associated with AF and this could give rise to reduction in rehospitalization. Second, heart rate reduction with BBs in HFpEF with AF could have prevented tachycardia-induced HF and rehospitalization. In this study, heart rate was lower in the BB-treated group during follow up (Supplementary Table 3).
Several limitations of the present study should be noted and caution is needed in the interpretation. First, because the sample size was relatively small, this study might be underpowered. There is the possibility of a type II error, especially in HF rehospitalization, because the survival curves of patients with HFrEF, especially rehospitalization, diverge. We calculated the power for rehospitalization outcome in HFrEF patients. A two-sided test of whether the HR was one with an overall sample size of 748 subjects (of which 335 are in the control group and 335 are in the treatment group) achieved 32% power at a 0.050 significance level when the HR was actually 0.699. It was anticipated that proportions of subjects having the event during the study should be 0.123 for the control group and 0.087 for the treatment group. This study was not powered to investigate several outcomes, especially the influence of BB on rehospitalization. Thus, the present findings might be due to a Type II error. Second, subgroup analysis had many limitations because of the small sample size. In the report from the Swedish Heart Failure Registry, heart rate >100 beats per minute was associated with an increased mortality in HFrEF with AF.17 In this study, the number of patients with heart rate > 100 beats per minute on discharge was small; hence, subgroup analysis for the patients with a high heart rate could not be performed. In addition, BB has more pronounced prognostic implication in patients with a history of myocardial infarction. However, the number of patients with a history of myocardial infarction was very small in patients with HFpEF and AF; therefore, subgroup analysis was not possible in these patients. In the myocardial infarction and ischemic heart disease subgroup, the insignificant interaction for 1-year mortality might also be caused by the small sample size. Third, this observational cohort study was likely subject to selection bias, because treatment was entirely dependent on the attending physician's decision. The PS matching method was applied to balance confounders as much as possible; however, because of the limited sample size, few variables were available for extensive adjustment using PS matching. The Cox regression models were then constructed to adjust for baseline confounders to reduce residual confounders as much as possible, although we could not rule out potential unmeasured confounders. Fourth, AF-specific information was limited, as AF diagnosis was based on electrocardiography at admission or during hospitalization; this may have led to an underestimation of AF. Finally, the purpose of this study was to evaluate whether BB therapy at discharge has prognostic implications. Treatment with BB was defined at discharge and the likely crossover throughout the follow-up; hence, this might have interfered with the potential associations with outcomes (Supplementary Fig. 3). Moreover, BB-untreated patients may have been at a higher risk due to past intolerance or perceived risk of future intolerance. With decreasing numbers of patients at risk and increasing crossover patients over time, findings at longer durations of follow-up should be interpreted with caution and may underestimate benefits associated with BB use.
In conclusion, the use of BBs at discharge was not associated with clinical outcomes at the 60-day and 1-year follow-ups in real-world hospitalized patients with HFrEF and AF. In HFpEF with AF, BB was only associated with lower incidence of rehospitalization at the 6-month and 1-year follow up. Further investigations are required for the development of optimal therapeutic options for this patient subgroup.
 XML Download
XML Download