

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Studies have suggested that long-term exposure to ambient particulate matter leads to an estimated 42,241,000 premature deaths globally.1 Elderly persons aged 70 years or older account for the largest share of deaths (2,228,300 deaths).1 When exposed to air pollution, elderly adults are more susceptible to cardiovascular and pulmonary conditions than younger adults.23 Previous studies have shown that an increase in particulate matter of less than 2.5 μm (PM2.5) in size is associated with an increase in systolic and diastolic blood pressure (SBP and DBP).45678 An association between exposure to air pollution and decline of peak expiratory flow rate in elderly adults in Korea was also suggested.9
Because the health impact of PM2.5 is considerably large and there is a need to employ strategies to reduce emission of pollutants and exposure to air pollution, several studies have investigated person-level strategies for preventing air pollution-associated health effects. The investigation of personal protection measures such as particulate respirators, air purifiers, supplementation drugs, and dietary intake patterns have shown inconsistent effects.10111213141516171819202122 Most studies have investigated the efficacy of person-level protection among young healthy populations, while only a few have examined air filtration, supplementation, and nutrition in elderly adults.111719 However, to the best of our knowledge, no previous studies have examined the health protection effects of particulate respirators in elderly adults. Moreover, it is unclear whether particulate respirators are safe for extended use in this population. In a previous study, long-hour use of respirators for health care providers caused headache, shortness of breath, and discomfort.23 Occupational health studies have also suggested that workers experience poorer performance and anxiety while wearing respirators.2425 For elderly adults, particulate respirator use may cause adverse effects, including physiological stress.26 However, no studies have examined whether particulate respirators both reduce exposure to particulate matter and elevate stress in elderly adults.
Given the effects of PM2.5 exposure on cardiopulmonary function, we aimed to investigate the efficacy of particulate respirators in protecting elderly adults against exposure to particulate matter. In a quasi-experimental study, we compared cardiopulmonary indicators before and after the use of particulate respirators among elderly women.
METHODS
Participants
We conducted a quasi-experimental study in women aged 65 years or older in Seoul, Korea from May to July 2018. To control for gender effects in the small study, we recruited older women participants only. We estimated that with a sample of 20 participants, the study would have a 90% power to detect a mean difference of SBP that was 7 mmHg lower while wearing particulate respirators compared with the control group,15 using a log-rank test at 5% significance level. Assuming a 5% dropout rate, we recruited 21 women aged 65 years or older who agreed to participate, had no history of tobacco smoking, and no clinically-diagnosed chronic diseases such as myocardial infarction, diabetes, asthma, dementia, and cancer.
Intervention
A total of 21 women participated in the intervention. Participants served as their own control and underwent the following study protocol for three consecutive weeks to avoid potential confounders, including long-term and seasonal trends in health outcomes: one control period in which participants wore no particulate respirators, one experimental period in which they did wear respirators, and an additional control period in which they again wore no respirators. No participants missed any health examinations. At the recruitment, participants were asked to draw a number out of a hat. The participants were randomly assigned a date (one of the weekdays) from May–July 2018 for an initial health visit and were followed for three consecutive weeks (e.g., 1st Control, May 11th– May 17th; Experiment, May 18th – May 24th; and 2nd Control, May 25th– May 31st). On the last day of each period (May 17th, 24th, and 31st in the above example), the participants completed questionnaires and underwent thorough cardiopulmonary and heart rate variability tests as well as urine and blood sampling. On the day before the last day of each period, participants were asked to visit the study site at 9 am and wear a direct reading personal aerosol monitor for at least 12 hours (from 10:00 am to 9:59 pm) or for as long as possible. For the experiment, participants were given 6 particulate respirators (one per day) and were instructed to wear the same respirator each day for 6 days (May 19th to May 24th in the above example) until the health examination and for as long as possible except while eating, sleeping, and washing.
Health examinations
Standing height (cm) and weight (kg) were recorded at the first visit to the study site. We collected information on demographic characteristics such as age, education years, income, physical activity, smoking, alcohol consumption, diagnosed diseases, and dietary patterns via questionnaire. Cardiopulmonary tests included measurements of BP (SBP, DBP, mean arterial pressure [MAP], and pulse pressure [PP]) and lung function (forced expiratory volume in 1 second [FEV1, L], forced vital capacity [FVC, L], the ratio of FEV1 to FVC [FEV1/FVC, %], and forced expiratory flow at 25%–75% of the FVC [FEF25–75, L/s]).
Changes in heart rate variability (HRV) explain increased respiration rate while wearing respirators.27 We measured four HRV markers, including two time-domain (the standard deviation of normal-to-normal intervals [SDNN] and square root of the mean squared differences of successive NN intervals [rMSSD]) and two normalized frequency-domain variables (high frequency [HF] and low frequency [LF]). The ratio of LF to HF was also computed. Additionally, increased oxidative stress indicates an imbalance between prooxidants and antioxidants in the body, which can also be viewed as physiological stress.28 Therefore, urinary 8-hydroxy-2′-deoxyguanosine (8-OHdG) was measured as an oxidative stress marker. Detailed methods for measuring BP, lung function, HRV, and 8-OHdG are described in Supplementary Method 1.
Particulate respirators
Disposable particulate respirators (PNTD, Mungyeong, Korea) were used during the quasi-experimental study. The minimum measured filtration efficiency of the respirators was 80% for 0.6 µm nonoil particulates.29 A respirator fitting test assessing the face-to-respirator seal was performed using the Mask Fitting Tester MT-03 (SIBATA Science Technology, Saitama, Japan). Detailed methods for the particulate respirator and the associated fitting test are described in Supplementary Method 2.
Environmental data
We used moving averages of daily ambient PM2.5 concentrations and apparent temperature (AT, °C) on the concurrent days and up to previous five days (lag 05) to control for short-term and cumulative exposure to PM2.5 and AT. Additionally, we used a 24-hour direct reading monitor to obtain data regarding personal exposure to PM2.5. Detailed methods for measurements of ambient PM2.5 and AT and personal exposure to PM2.5 are described in Supplementary Method 3.
Statistical analysis
We used linear mixed-effect models to account for repeated measurements and to investigate the effects of particulate respirators on cardiopulmonary function and physiological stress. HRV (SDNN, rMSSD, HF, LF, and the ratio of LF to HF) and pulmonary test results (FEV1, FVC, and FEV1/FVC) were log-transformed for normality before regression analysis. The intervention was coded as a dummy variable (0 for control and 1 for experiment) and examined in the regression model. In the model, we controlled for age, weight (kg), height (cm), regular alcohol drinking (yes or no), and antihypertensive medication use (0 for no and 1 for yes). The covariates were included in the fixed term, whereas random intercepts for subjects were incorporated into the model to account for correlation within individuals. The effects were expressed as either changed values or percentages among those with a particulate respirator compared with the control groups who did not wear particulate respirators (who were evaluated before and after those with the respirators, with the corresponding 95% confidence intervals [CI]). Because we observed similar results between the control groups (pre- and post-respirator period), we combined the two control periods for the main analysis and performed a separate analysis for the individual control groups (i.e., before and after the respirators). The results of these analyses are shown in the supplementary materials. In addition, PM2.5 and AT during each period were controlled for in the model to reduce the confounding effects of the background environment during the control and experimental periods and estimate independent effects of particulate respirators on cardiopulmonary and stress markers from environmental factors (PM2.5 and AT). In an additional analysis, we compared the efficacy of particulate respirators among those with and without antihypertensive medication use. In a sensitivity analysis, we repeated the analysis for those who had low compliance for wearing their particulate respirators. All statistical analyses were performed using the “gamm4” package for R software (version 3.5.1; R Project for Statistical Computing, Vienna, Austria).
Ethics statement
All subjects voluntarily participated and provided written informed consent, and this study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. H-1710-046-892). An independent data and safety monitoring board monitored the study. The protocol was in accordance with the Declaration of Helsinki and institutional guidelines.
RESULTS
The mean age of participants was 72.7 years (min, 64.0; max, 79.0; SD, 3.8), and mean weight and height were 56.6 kg and 152.5 cm, respectively. One person was exposed to secondhand smoking at home for an average of 2 hours per day, whereas the other participants were not exposed to secondhand smoking at home or any other indoor places. Only four elderly women were current drinkers, and all participants were never-smokers. Eight elderly women were under antihypertensive treatment (38.1%) (Table 1). Prior to participating in the study, all participants reported that they usually did not wear particulate respirators unless they were in areas with a high level of dust. However, during the study period, all participants adhered to the study guidelines except for two women as described in Supplementary Method 4.
Table 1
Basic characteristics of participants (n = 21)
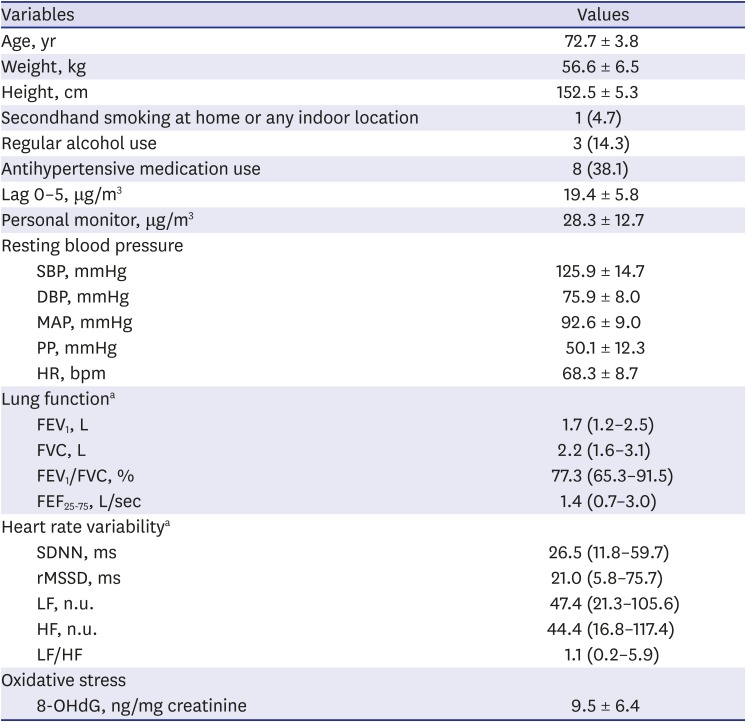
Data are presented as mean ± standard deviation or number (%).
SBP = systolic blood pressure, DBP = diastolic blood pressure, MAP = mean arterial pressure, PP = pulse pressure, HR = heart rate, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, FEV1/FVC = the ratio of FEV1 to FVC, FEF25–75 = forced expiratory flow at 25%–75% of the FVC, SDNN = the standard deviation of normal-to-normal intervals, rMSSD = square root of the mean squared differences of successive NN intervals, HF = high frequency (normalized), LF = low frequency (normalized), n.u. = none-unit, LF/HF = the ratio of LF to HF, 8-OHdG = 8-hydroxy-2′-deoxyguanosine.
aGeometric mean and 95% confidence limits.
Mean levels of PM2.5 concentrations during the two control periods and the experimental period are compared in Supplementary Table 1. Based on the 12-hour personal PM2.5 monitor, the mean levels of measured personal PM2.5 concentrations during the two control periods (pre- and post-non-respirator period) and the respirator period were 31.9 µg/m3, 25.6 µg/m3, and 27.4 µg/m3, respectively. Accounting for respirator fitting performance (Supplementary Table 2), we estimated plausible personal exposure to PM2.5 while wearing particulate respirators during the experimental period (Fig. 1). For persons wearing respirators during the experimental period, the mean estimated level of personal exposure to PM2.5 was 19.8 µg/m3, which was calculated by multiplying the personal monitored level with the individual's leaking rate. The difference in the mean level of exposure to PM2.5 between the experimental period and control periods, accounting for respirator fitting performance, was 9.0 µg/m3 (calculated by subtracting 19.8 µg/m3 from 28.8 µg/m3).
Fig. 1
Kernel density estimation of personal exposure to PM2.5 concentrations during control and experimental periods with and without particulate respirators after accounting for respirator fitting performance (n = 21). Two smoothing lines for the distribution of PM2.5 exposure levels with and without particulate respirators were derived based on Kernel density estimation.
PM2.5 = particulate matter < 2.5 µm in diameter.
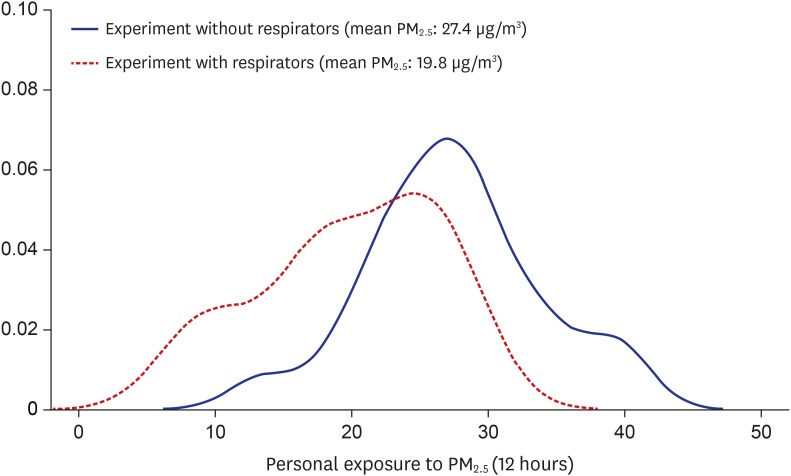
Fig. 2 and Supplementary Table 1 show cardiopulmonary and stress indicators during experiment and pre- and post-experiment control periods. The experiment period resulted in lower levels of SBP, DBP, MAP, PP, and log-HF than the control periods, but higher levels of log-FEV1, log-LF/HF, and 8-OHdG.
Fig. 2
Cardiopulmonary indicators during control (pre and post) and experimental periods (mean and 95% confidence limits in vertical lines). (A) SBP; (B) DBP; (C) MAP; (D) PP; (E) log-FEV1; (F) log-HF; (G) LF/HF; (H) 8-OHdG.
SBP = systolic blood pressure, DBP = diastolic blood pressure, MAP = mean arterial pressure, PP = pulse pressure, log-FEV1 = Forced expiratory volume in 1 second, log-HF = high frequency (normalized), LF/HF = the ratio of LF to HF, 8-OHdG = 8-hydroxy-2′-deoxyguanosine.
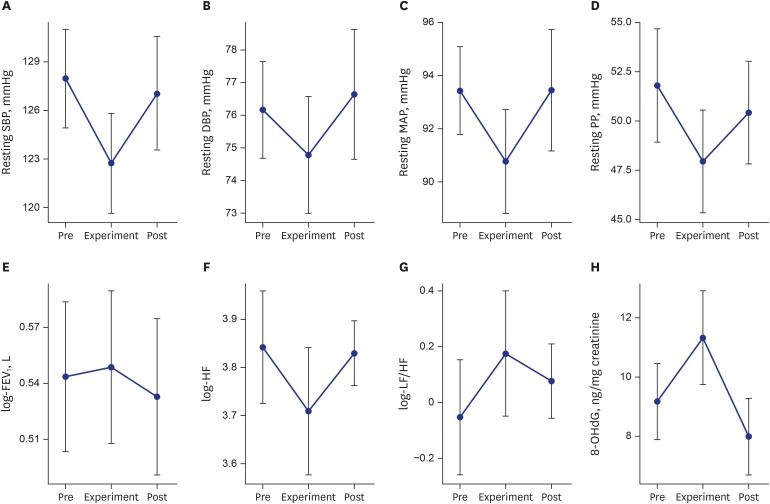
Table 2 shows the effects of particulate respirators on cardiopulmonary indicators after controlling for covariates, including PM2.5 levels. We observed a significant reduction in resting SBP (−5.3 mmHg [95% CI, −9.3 mmHg, −1.2 mmHg]), MAP (−2.9 mmHg [95% CI, −6.2 mmHg, 0.3 mmHg]), and PP (−3.6 mmHg [95% CI, −6.5 mmHg, −0.6 mmHg]). Participants using antihypertensive medications showed a slightly greater reduction in SBP, DBP, and MAP than those without antihypertensive medication use, although differences in BP between participants with and without antihypertensive medication use were not statistically significant (Supplementary Fig. 1). We also found associations for other outcome variables than primary outcome markers. Lung function indices generally indicated that wearing particulate respirators was protective (FEV1, 1.7% [95% CI, 0.0%, 3.3%]; FEF25-75, 1.9% [95% CI, −5.6%, 10.1%]); however, statistical significance was not confirmed (Table 2). A comparison among the three periods showed similar results (Supplementary Table 3). After excluding two women elderly adults with low compliance for wearing the respirators, results showed improvements in lung function (FEV1, 2.3% [95% CI, 0.5%, 4.1%]) (Supplementary Table 4).
Table 2
Changes in cardiopulmonary indicators during the experimental period compared with the control periods
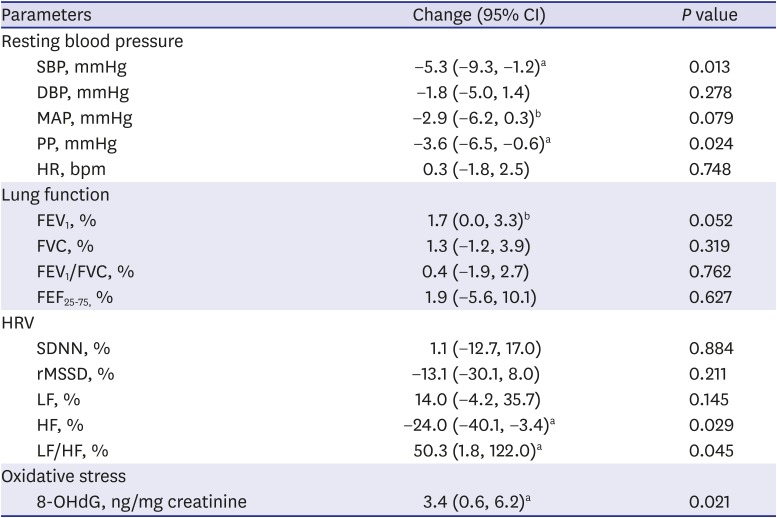
In the model, we controlled for age (years), weight (kg), height (cm), regular alcohol drinking (yes or no), antihypertensive medication use (0 for no and 1 for yes), PM2.5, and apparent temperature (reference: control periods).
CI = confidence interval, SBP = systolic blood pressure, DBP = diastolic blood pressure, MAP = mean arterial pressure, PP = pulse pressure, HR = heart rate, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, FEV1/FVC = the ratio of FEV1 to FVC, FEF25–75= forced expiratory flow at 25%–75% of the FVC, HRV = heart rate variability, SDNN = the standard deviation of normal-to-normal intervals, rMSSD = square root of the mean squared differences of successive NN intervals, HF = high frequency (normalized), LF = low frequency (normalized), LF/HF = the ratio of LF to HF, 8-OHdG = 8-hydroxy-2′-deoxyguanosine.
aP < 0.05; bP < 0.1.
Physiological stress markers were associated with wearing particulate respirators (Table 2). Parasympathetic activity (HF) significantly decreased (−24.0% [95% CI, −40.1%, −3.4%]) while wearing respirators, whereas sympathetic activity (LF/HF ratio) significantly increased (50.3% [95% CI, 1.8%, 122.0%]). We observed greater changes in LF, HF, and the LF/HF ratio among participants with antihypertensive medication use than those without (Supplementary Fig. 2). Furthermore, we observed that the oxidative stress marker 8-OHdG increased by 3.4 ng/mg creatinine (95% CI, 0.6 ng/mg creatinine, 6.2 ng/mg creatinine) during the experimental period compared with that during the control period. Similar to the BP markers, we observed slightly greater changes in physiological stress markers after excluding those with low compliance for wearing respirators. These changes for other outcomes can be regarded as exploratory findings at the moment, which need to be evaluated further in the future.
DISCUSSION
This study evaluated the effect of particulate respirators on cardiopulmonary indicators among elderly women in Korea. We observed a significant reduction in resting BP during the experimental period compared with that during the control period. Although lung function appeared to improve with the use of particulate respirators, this change was not statistically significant. Furthermore, we observed increased physiological stress markers, including increased sympathetic (LF/HF) and decreased parasympathetic (HF) activities and increased oxidative stress (8-OHdG) during the experimental period.
The beneficial effect of particulate respirators on BP was consistent with a previous study. Shi et al.30 investigated the effects of particulate respirators among university students, and their results showed the same direction in BP change as the present study. They found a 2.7 mmHg (95% CI, −5.2 mmHg, −0.1 mmHg) decrease in SBP during the experimental period (particulate respirator use) compared with that during the control period (no particulate respirator use). Our results suggest that the benefit of particulate respirators is greater among elderly adults (5.3 mmHg).
However, we also observed an increase in physiological stress markers among our participants. Increased sympathetic (LF/HF ratio) and decreased parasympathetic (HF) activities are related to respiration rate27 and psychological stress.3132 Increased oxidative stress was also associated with particulate respirator use in our study. Particulate respirator use may protect from exposure to particulate matter,33 but it may also lead to increased skin temperature,25 anxiety,24 shortness of breath, discomfort, and headache.23 Furthermore, hypertensive participants seem to be more sensitive to wearing particulate respirators compared with non-hypertensive participants, in terms of changes in HRV and oxidative stress. In contrast to our findings, Shi et al.30 found that particulate respirators had protective effects on HRV markers, including decreased sympathetic (LF/HF ratio) and increased parasympathetic (HF) activities. Although we do not have a clear explanation for the discrepancy between the study by Shi et al. and the present study, it may be due to differences in the studies’ parameters, including ambient PM2.5 levels (19 µg/m3 vs. 74 µg/m3), age (elderly adults vs. college students), brand/type of particulate respirator (KF80 vs. N95), and other unknown factors that may have impacted the results.
This quasi-experimental study is the first to investigate the effects of particulate respirator use in an elderly population, using one experimental and two control periods to measure personal exposure to PM2.5, cardiopulmonary function, and physiological stress indicators. Our study had several limitations. First, we restricted participant inclusion criteria to relatively healthy, nonsmoking, and women elderly subjects with no critical health conditions (except hypertension). Therefore, generalization of the results to the elderly population is limited due to the high prevalence of diabetes, dyslipidemia, and other chronic diseases in this population.3435 Additionally, because we used a specific type of particulate respirator (KF80), we cannot generalize our results to other types of particulate respirators that have a different particle filtration quality.
Second, we conducted the study in participants' ordinary life settings. Therefore, we could not control for other factors that may influence PM2.5 exposure and health indicators. However, in this quasi-experimental study, an individual was randomly assigned to an intervention date and acted as her own control, which permitted between- and within-group comparisons, resulting in a reduction in measured and unmeasured confounders.3637 Although the comparison of pre- and post-experiment was not randomized, the resulting schedule for the comparison of pre- and post-experiment was decided by the first random allocation to participants. Moreover, the open-label trial could have affected the outcome by changing behaviors, which we did not measure in the study. Therefore, the open-label effect is a limitation of the study.
Third, we investigated the effects of particulate respirators with similar levels of PM2.5 (around 20 µg/m3) during the control and experimental periods. Therefore, we could not estimate changes in markers associated with wearing particulate respirators by different PM2.5 levels (e.g., low vs. high concentration of PM2.5). Because recent studies have shown a nonlinear dose-response relationship,38394041 the intervention-benefit relationship may also not be linear. Our study is limited in that we cannot apply our result directly to different ranges of PM2.5 levels. Moreover, we cannot recommend the optimal PM2.5 level at which particulate respirators should be worn by elderly people. Further studies examining a wide range of PM2.5 levels are needed to determine the level at which the positive effects of wearing a particulate respirator outweigh the adverse effects.
Finally, the present study lacked a wash-out period (usually lasting for approximately two weeks) between the control and respirator periods to eliminate any influence of one period on another. Although a wash-out period would have been important to control for the potential impact of wearing the respirator on the second control period, we did not consider this in the study. However, we did observe that the two control periods had similar outcomes (e.g., SBP and DBP levels), although these differed from those of the respirator period. Therefore, we assumed that wearing respirators could have immediate rather than delayed effects.
Our study suggests that particulate respirators have protective effects in the elderly population, which include the prevention of PM2.5-induced elevated BP and the increase of physiological stress when wearing particulate respirators. Therefore, those with cardiovascular disease may benefit from the effects of particulate respirators. Due to the limitations of our study design, caution should be exercised when interpreting the results of this study and when applying the findings in clinical practice. Further studies are warranted to compare the effects of particulate respirator use with various PM2.5 levels in healthy elderly adults versus those with chronic illness such as respiratory disease, cardiovascular disease, and diabetes.
 XML Download
XML Download