

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hypertension is a worldwide public health challenge affecting approximately one billion individuals [12]. Globally, high blood pressure contributed to the 92 million or 6.0% of all disability-adjusted life years (DALYs) among adults aged ≥ 45 years old [3]. The World Health Organization (WHO) reported 1.13 billion adults aged ≥ 18 years old had raised blood pressure in 2015 and the prevalence of hypertension among adults aged ≥ 20 years old was predicted to increase from 52.7% (972 million) in 2000 to approximately 60%, equating to 1.56 billion in 2025 [145].
The American Heart Association (AHA) documented aging, being male, family history and genetics as non-modifiable risk factors for hypertension and high body mass index (BMI), physical inactivity, low income, smoking and tobacco use, excess intake of alcohol as modifiable risk factors [67]. A diet high in sodium, saturated fatty and trans-fatty acids, and added sugar was associated with an increase in blood pressure [8910].
The US immigrant studies from national data found that Filipinos had the highest prevalence of hypertension and the highest hypertension mortality rate among Asian immigrants [1112]. One study conducted among female marriage immigrants in Korea reported that Filipino women had the highest proportion of high blood pressure compared to Japanese, Chinese, Vietnamese, and Cambodians [13].
Frying food is one of the most common and preferred cooking methods in the Philippines, probably because it is a convenient food preparation and fried food has a savory flavor favored by Filipinos [1415]. During the frying process, the amount of oil absorbed into foods can reach up to 40% of the total weight of the food product [16,17]. Furthermore, during frying, the heated oil undergoes deterioration due to various chemical reactions like thermal oxidation, and thermally-oxidized oil induced oxidative stress [18]. Studies that examined the relationship of oxidative stress and endothelial dysfunction reported that oxidative stress was involved in the pathogenesis of endothelial dysfunction, one of the biological mechanisms responsible for the development of hypertension [19202122].
A cohort study in Spain reported that frequent intake of fried food was associated with a higher risk of hypertension and with the central adiposity and high blood pressure [23,24]. Also, a Spanish cross-sectional study found that high fried food intake was associated with high prevalence of hypertension when these foods were fried with re-used oils [25]. Another cross-sectional study in Korean adults suggested that frequent fried food intake was associated with high prevalence of hypertension among women [26].
Given the evidences that Filipino immigrants are at higher risk for hypertension and intake of fried food among Filipino women is common, this study aimed to examine the association of fried food intake and prehypertension and hypertension combined among Filipino women.
SUBJECTS AND METHODS
Study population
The present study is a cross-sectional study of fried food intake and the prevalence of elevated blood pressure among the Filipino Women's Diet and Health Study (FiLWHEL) participants. Data were collected from 504 Filipino women aged 19 years or above using structured questionnaires, including demographic, health-related behavior, medical history, quality of life, acculturation, anthropometric examination and biospecimen. More information regarding the description of the FiLWHEL study design and methods have previously been published elsewhere [272829].
Out of 504 participants, 76 were excluded because of no 24-hour recalls (n = 7), unusual energy intake (3 standard deviations above or below the log-transformed mean energy intake; n = 7), and only one BP measurement (n = 24) or self-reported physician diagnosis of hypertension or use of antihypertensive medication (n = 38). As a result, 428 participants were included in the analysis. Prior to participation, all study participants gave written informed consent. The Sookmyung Women's University Institutional Review Board (reference number SMWU-1311-BR-012) approved this study.
Dietary intake assessment
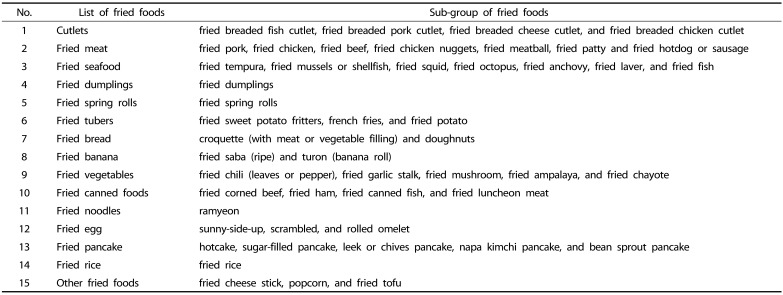
Fried food intake was determined using the one-day 24-hour recall method through an in-person or via telephone interview. Fried food was defined as deep fried, shallow fried, pan fried and stir fried. The list of fried foods is presented in Table 1. The total fried food intake per person was estimated by summing the amount of all fried foods consumed at home or away from home.
Fried food percent energy intake was calculated as total energy intakes from fried food (kcal/day) divided by total energy intakes from all food (kcal/day) multiplied by 100. Fried food (grams/day) per 1,000 kcal of total energy intake was also calculated. Collected data were coded using the Computer Aided Nutritional Analysis Program version 4.0 for professional (CAN-pro 4.0). The nutrition information of some food items that were not available in CAN-pro software were derived from the U.S. Department of Agriculture (USDA) [30], Rural Development Administration (RDA) of Korea [31], Food and Nutrition Research Institute (FNRI) of the Philippines (specifically for Filipino foods) [32] or the manufacturer's product's nutritional label.
Blood pressure measurements
In accordance with the standard principle of blood pressure measurement, mercury sphygmomanometer was used to measure blood pressure with at least 5-minute rest while the participant was seated calmly. Using the same arm, two blood pressure readings with a 5-minute interval after the first measurement were obtained and the average of the two readings was used for the analysis. Elevated blood pressure was categorized into prehypertension with systolic blood pressure (SBP) of 120 - < 140 mmHg or diastolic blood pressure (DBP) of 80 - < 90 mmHg and hypertension with SBP of ≥ 140 or DBP of ≥ 90 mmHg or the used of antihypertensive medication [7].
Anthropometric measurements
Height and waist circumference were measured to the nearest 0.1 cm using a stretch-resistant tape measure with the participant in standing position. Waist circumference was measured at midpoint between the lowest border of the rib cage and the upper most lateral border of the right iliac crest. To measure body weight, bioelectric impedance analysis machine (InBody 620, Biospace Co. Ltd, Seoul, Korea) was used. BMI was calculated as weight in kilograms (kg) divided by square of height in meters (m2). Details of anthropometric measurements have been published elsewhere [27].
Statistical analysis
Participants were classified into blood pressure categories: normotensive and pre-hypertensive and hypertensive combined. For fried food intake, participants were categorized into non-fried food consumers and tertile levels among fried food consumers. Deep and shallow fried food intake and pan and stir fried food intake were also analyzed separately. Non-fried food consumers were considered as the referent category. Analysis of variance (ANOVA) and chi-square test were used to compare the means and proportions of baseline characteristics of the study participants according to fried food intake. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated using multivariate logistic regression models. Tests for linear trend across increasing categories of fried food intake were conducted by assigning medians of the intake of fried food within each category and treating this variable as a continuous variable. The multivariate analysis was adjusted for age (years, continuous), energy intake (kcal/day, continuous), education level (high school or below, college or above-category), length of stay in South Korea (years, continuous), smoking status (ever, never-category), and alcohol intake (ever, never-category). BMI (< 23 and ≥ 23 kg/m2) was adjusted in the additional analysis using the WHO Asia-Pacific cut-off points for overweight [33]. When we further adjusted for vigorous physical activities (hours/day, continuous), sodium intake (grams/day, continuous) and sleeping hours (< 5 hours, 5–6 hours, 7–8 hours, > 8 hours-category), we did not observe appreciable change in the estimates and therefore we did not include those variables in the model. Interactions were examined using the Likelihood Ratio Test (LRT) by including a cross-product term in the model. All P-values presented were two-tailed and P < 0.05 was considered to be statistically significant. All analyses were performed using SAS version 9.4 software package (SAS Institute Inc., Cary, NC, USA).
RESULTS
Characteristics of participants according to fried food intake
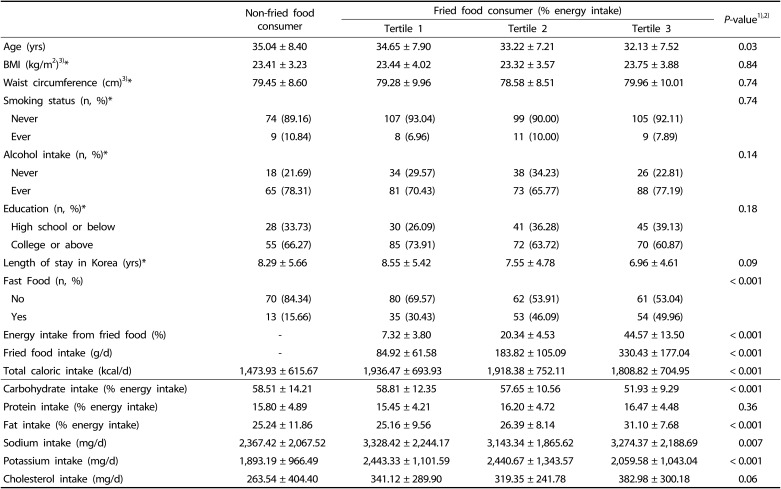
A total of 428 women (mean ± SD age: 33.77 ± 7.78 yrs) were included in the analysis. The prevalence was 28.04% (n = 120) for prehypertension (120 - < 140 mmHg of SBP or 80 - < 90 mmHg of DBP) and 13.32% (n = 57) for hypertension (≥ 140 mmHg of SBP or ≥ 90 mmHg of DBP). Among fried food consumers, their mean intake values were 199.72 g/d for total fried food, 165.92 g/d for deep and shallow fried food and 134.26 g/d for pan and stir fried food. Fried food consumers were younger and tended to consume more fast food compared to non-fried food consumers (Table 2). Intakes of total energy, fat, sodium, potassium, and cholesterol were higher among high fried food consumers but lower in carbohydrate intake as compared to non-fried food consumers.
Association between fried food intake and prehypertension and hypertension combined
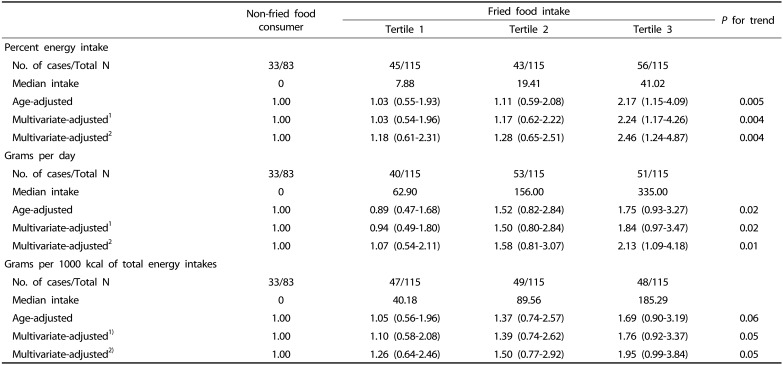
High fried food intake was associated with high prevalence of prehypertension and hypertension combined (Table 3). Compared to non-fried food consumers, the multivariate-adjusted ORs and 95% CIs for having elevated blood pressure among fried food consumers were 1.03 (95% CI: 0.54–1.96) in the 1st tertile, 1.17 (95% CI: 0.62–2.22) in the 2nd tertile, and 2.24 (95% CI: 1.17–4.26) in the 3rd tertile of fried food intake (% energy intake) (P for trend = 0.004). When adjusted for BMI, compared to non-fried food consumers, the ORs and 95% CIs for the 1st, 2nd, and 3rd tertiles were 1.18 (0.61–2.31), 1.28 (0.65–2.51) and 2.46 (1.24–4.87), respectively, (P for trend = 0.004). A similar pattern was observed when fried food intake as grams per day or grams per 1,000 kcal of total energy intake was analyzed. When only hypertension was considered as an endpoint, the prevalence was still higher, albeit not statistically significant (Table 4), comparing the 3rd tertile of fried food consumers with non-fried food consumers.
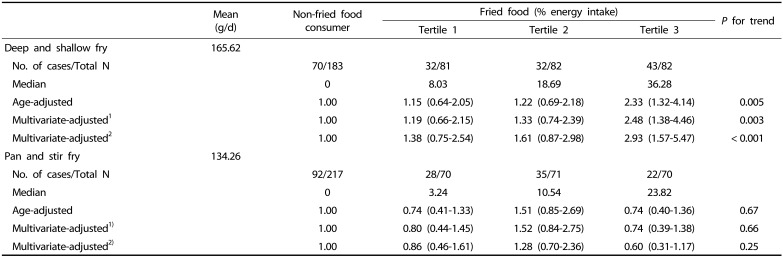
For the separate analyses of deep and shallow fried food intake or pan and stir fried food intake, there was a high prevalence of prehypertension and hypertension combined limited to deep and shallow fried food (Table 5); ORs (95% CIs) for the 1st, 2nd, and 3rd tertiles of fried food intake were 1.19 (0.66–2.15), 1.33 (0.74–2.39) and 2.48 (1.38–4.46), respectively, (P for trend = 0.003). When BMI was added to the multivariate model, compared to non-fried food consumers, the ORs and 95% CIs for the 1st, 2nd, and 3rd tertiles were 1.38 (0.75–2.54), 1.61 (0.87–2.98), and 2.93 (1.57–5.47), respectively, (P for trend = < 0.001). However, the tertiles of pan and stir fried food consumers were compared to non-fried food consumers, there was no significant association.
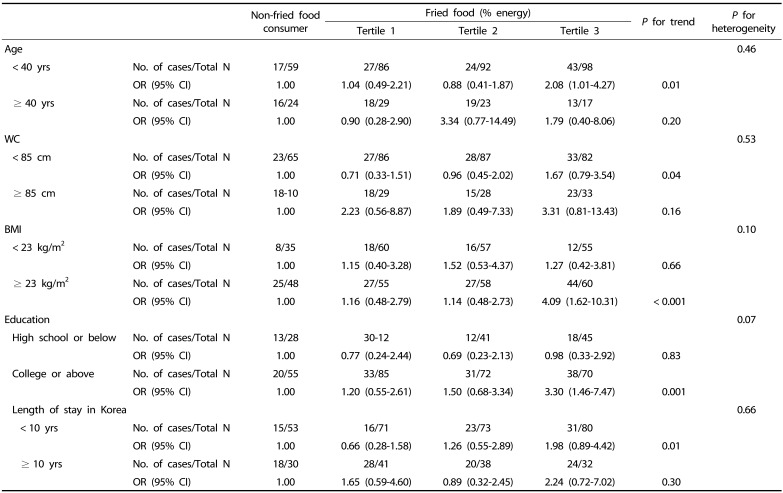
Interaction by age, obesity, education and length of stay
Examination of whether the association of fried food intakes and prehypertension and hypertension combined was modified by age, anthropometric measures, education, and length of stay in South Korea, revealed that there was only a borderline significant interaction with education (P for heterogeneity = 0.07) (Table 6). The association was more pronounced among those who graduated from college or above than those who graduated from high school or below. In addition, those with higher BMI tended to have high prevalence of prehypertension and hypertension combined with high fried food intake, but this pattern was not clear for those with lower BMI.
DISCUSSION
This study found that high fried food intake was associated with high prevalence of prehypertension and hypertension combined among Filipino women married to Korean men. Compared to non-fried food consumers, Filipino women in the highest tertile of fried food intake had a 2-fold higher prevalence of prehypertension and hypertension combined. The association was observed for deep and shallow fried food intake but not for pan and stir fried food intake. In addition, the association between fried food intake and prehypertension and hypertension combined was more apparent for Filipino women with a higher BMI or with higher education compared to those with a lower BMI or lower education, respectively.
Only a few epidemiologic studies examined the association between fried food intake and hypertension. The Seguimiento Universidad de Navarra (SUN) project, a prospective cohort from Spain, previously reported that frequent consumption of fried foods was associated with higher risk of developing hypertension among young adults after 6.3 years of follow-up. In that study, comparing those who consumed fried foods < 2 times/week with those who consumed fried food > 2-4 and > 4 times/week, the relative risk (RR) were 1.18 (95% CI: 1.03, 1.36) and 1.21 (95% CI: 1.04, 1.41), respectively, (P for trend = 0.009) [23]. Furthermore, another SUN study reported that, in comparison to those who consumed fried foods > 4 times/week with ≤ 2 times/week, after 8.3 years of follow-up, the RR for developing high blood pressure was 1.16 (95% CI: 1.02, 1.32; P for trend = 0.011) [24].
The present study showed similar findings to two cross-sectional studies carried out in Spain and in Korea. The Spanish study found that fried food intake was associated with prevalence of hypertension, especially when degraded vegetable oils, such as sunflower oil, were re-used [25]. Also, prolonged intakes of the repeated heated oil has been reported to increase blood pressure [34]. However, in the present study, it was not possible to differentiate between the different type of oils or fats used to fry or if they ever use used oils in frying. In the 5th Korean National Health and Nutrition Survey (KNHANES) 2010–2011 of Korean adults, the prevalence of hypertension increased by 2.4-fold in women with > 2 times/week fried food intake compared with those who rarely consumed it [26].
There are various possible mechanisms behind the blood pressure raising effect of heated oil. During frying, heated oil undergoes deterioration due to the exposure of oil to high temperatures in the presence of air and moisture [35,36]. Thermally-oxidized oil generates free radicals which in turn react with nitric oxide (NO), causing activation of peroxynitrite, which propagates the chain of lipid peroxidation [182137]. Also, it has been reported that hypertensive individuals have high levels of malondialdehyde (MDA), a breakdown product of lipid peroxidation and a known marker of oxidative stress [1838]. Several narrative reviews reported that oxidative stress instigates vascular inflammation by activating the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), promoting endothelial dysfunction which impairs the production of NO, increases vascular reactivity and resistance, as well as raises angiotensin II (Ang II) levels in vascular smooth muscle cells (VSMC), which may predispose risk of hypertension [1822343739].
In this study, we found high prevalence of hypertension with deep and shallow fried food, but not with pan and stir fried food. When oil is exposed to deep-frying temperature, it leads to a series of physicochemical changes such as production of volatile and non-volatile compounds, which affect the properties of oil and fried food [213540]. Also, deep-frying generates toxic compounds such as hydroperoxides, aldehydes, and other free radicals. These toxic products are absorbed into the food, ingested into the gastrointestinal tract, eventually entering the circulatory system [214142]. The frying method might have different effects on the absorption of fats depending on the food, food surface area, moisture content of food, the type of oil used, frying condition (time, temperature, fryer, etc.) and the degree of degradation [254344]. However, we could not assess whether the oil used was fresh or re-used.
This, to our knowledge, is the first study to examine the association of fried food intake and hypertension among Filipino women. Another strength of our study is that we defined prehypertension or hypertension based on blood pressure levels measured by trained physicians. Nonetheless, the study has several limitations. First, the cross-sectional design cannot infer any causal relationship between fried food and elevated blood pressure or hypertension. Although the current evidence is from a cross-sectional study, it is still reasonable within the context of achieving optimum health to recommend reducing or eliminating frying foods as well as avoidance of consuming fried foods among Filipino women. Secondly, the relatively small sample size based on convenience sampling does not represent the general population. Thirdly, the data on fried foods were collected from a one-day 24-hour recall, which does not represent the usual daily intake and might have some non-differential measurement errors. Lastly, we did not investigate in detail the type of fat or oil used for frying from a take away restaurant or away from home.
In conclusion, this study showed the evidence that high fried food intake, especially deep and shallow fried food was significantly associated with high prevalence of prehypertension and hypertension combined among Filipino women. Further prospective studies are warranted on the association of fried food intake and cardiovascular risk factors among Filipino women.

 XML Download
XML Download