

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Assessing dietary sodium intake is very important in public health care. Sodium intake, a modifiable risk factor, is associated with hypertension and kidney disease, and is ultimately related to cardiovascular deaths [1]. Limiting dietary salt consumption is known to be beneficial for preventing the progression of cardiovascular and kidney disease [23]. Currently, even healthy adults are encouraged to reduce dietary sodium [45].
Twenty-four-hour (hr) urinary sodium (Na; 24UNa) is the gold standard for estimating daily sodium intake [6] and is a reliable method for monitoring and assessing sodium intake for salt restriction in population studies [78]. It can also be used for objectively evaluating diuretic response, dietary compliance, blood pressure control and risk of cardiovascular disease among patients with edematous or hypertensive diseases such as liver cirrhosis [910], heart failure [11] and chronic kidney disease [1213]. However, obtaining 24-hr urine from outpatients is difficult and time-consuming, and the results are often imprecise due to inadequate urine collection. Therefore, it would be desirable to establish a simple and reliable test for estimating 24UNa excretion.
Dietary recall is known to under-report nutrient intake, and so gives less accurate estimates than those based on urinary data [1415]. Several techniques have been proposed to replace the 24-hr urine test. Trials based on casual urine samples, also known as spot urine, have been carried out. Tanaka's equation and the Korean formula have been suggested for estimating 24UNa [1617]. These two formulas identify patients who consume > 100 mEq of Na per day with sensitivities > 80% [17]. Urinary Na/creatinine (Na/Cr) and Na/potassium (Na/K) ratios have also been suggested for estimating daily sodium intake or salt loading, although the former needs correction for urinary Cr excretion [1018].
The spot urine test suffers disadvantages because the results vary depending on diet and inspection time. Mann et al. [18] reported that the Na/Cr ratio of late afternoon/early evening urine samples obtained near the midpoint of the 24-hr collection period was strongly correlated with actual 24UNa excretion. However, 57% of the participants examined were taking diuretics, which could have confounded the results [18]. No consensus has yet been reached on the best method for estimating daily sodium intake. In this study, urine samples were collected at every episode of urination for 24 hours. We measured Na and other electrolytes in each urine sample and examined any correlations that could represent 24UNa.
Go to : 
SUBJECTS AND METHODS
Subjects
Fifteen healthy men between 20 and 60 years old were enrolled in 3 teaching hospitals: Inje University Ilsan-Paik Hospital, Hanyang University Guri Hospital, and Yonsei University Gangnam Severance Hospital. None of the participants was taking any medication or had any chronic medical diseases such as hypertension, diabetes, hepatitis, inflammatory diseases, and malignancy. The study protocol was approved by the institutional review boards of Inje University, Ilsan-Paik Hospital (IB-0911-048), Hanyang University Guri Hospital (GURI 2009-11-005), and Yonsei University Gangnam Severance Hospital (3-2009-0178) and written informed consent was obtained before the screening procedure.
Processing and measurement of urinary parameters
On the first day, the fifteen men were offered 3 meals containing a total of 9–10 g of salt, prepared under the supervision of nutritionists working for each hospital. Ten of them consumed all the 10 g salt on the first day completely. The other 5 participants did not eat the full meals completely and their total intake was evaluated by the hospital nutritionist and the amount of salt consumed was calculated. All the participants had only 3 meals and drank as much water as they wanted over the 24-hr period. Twenty-four-hr urine was collected from the second-void urine of the first day to the first-void urine of the second day. The urine samples were collected by the participants, who were provided with graduated cylinders to measure the volume of each sample on site. All the samples were transported in conical centrifuge tubes and kept in a −70 degree refrigerator for further analysis.
24UNa excretion was estimated using Tanaka's equations and the Korean formulas for predicting 24-hr urinary Cr in Koreans: Tanaka's equations are: 1) Estimated 24UNa_Tanaka (mEq/day) = 21.98 × ({spot urine Na (mEq/L) / [10 × spot urine Cr (mg/dL)]} × predicted value of 24-hr urinary Cr (PRCr)_Tanaka)0.392 [16], 2) PRCr_Tanaka (mg/day) = −2.04 × age (yr) + 14.89 × weight (kg) + 16.14 × height (cm) − 2244.45 [16]. The Korean formulas are: 1) Estimated 24UNa_Korea (mEq/day) = 28.985 × ({spot urine Na (mEq/L) / [10 × spot urine Cr (mg/dL)]} × PRCr_Korea)0.346 [17], 2) PRCr_Korea (mg/day) = −7.428 × age (yr) + 10.372 × weight (kg) + 15.631 × height (cm) − 1,234.785 [17].
Urinary Na, K, chloride (Cl), urea nitrogen (UN), Cr, specific gravity (SG) and osmolality (Osm) were measured from each spot urine sample. All biochemical measurements were performed in a central laboratory (Green Cross Laboratories, Republic of Korea). Urinary Na, K and Cl were measured with ion selective electrodes using an automatic analyzer (ADVIA 1650, Siemens, USA). Urinary UN and Cr were measured with the same automatic analyzer by the kinetic UV assay and the Jaffe method, respectively. Urinary SG was measured by reflection refractometry using a URISYS 2400 (Roche, Japan). Urinary Osm was measured with a freezing point osmometer (Fiske one-ten, Fiske, USA).
Relationship between 24UNa and spot urine Na
We calculated the ratios of urinary Na to other urinary parameters, and identified any correlations with total measured 24UNa. Three sets of urine samples were compared: the first-void morning urine of the second day, the second-void urine of the first day, and all random urine samples from each participant. Urinary Na was adjusted for urinary K, Cr, Cl, UN, SG and Osm: urinary Na/K, urinary Na/Cr, urinary Na/Cl, urinary Na/UN, urinary Na/SG and urinary Na/Osm. The 24UNa level was estimated using Tanaka's equation and the Korean formula based on the results for all spot urine samples. Adjusted and estimated values were compared to the measured 24UNa, and their correlations were analyzed. The coefficients of intra-personal variation for each modified variable were also calculated to determine the variability of the methods.
Data analysis
Data are presented as means ± standard deviations (SD). Associations between measured 24UNa and demographic factors, spot urine Na and other urinary parameters were analyzed by the Pearson's correlation method. Intra-personal coefficients of variation were calculated as the ratio of the SD to the mean of each value and expressed as a percentage. Data were analyzed with the SPSS 15.0 program (SPSS Inc, Chicago, IL, USA).
Go to :
RESULTS
Clinical characteristics of the subjects
The basic characteristics of the fifteen men (mean 32.7 ± 6.5 years) are summarized in Table 1. Average dietary salt intake was 9.2 ± 1.2 g/day (range, 6.3–10 g/day) and average voiding frequency was 5.9 ± 1.9 voids/day. The total number of random urine samples was 88 (Table 2). The average voiding times of the second-void urine of the first day and the first-void urine of the second day were 11:54 ± 1:42 AM (median, 11:30 AM; range, 10:15 AM–16:10 PM) and 7:09 ± 1:00 AM (median, 7:17 AM; range, 5:55 AM–10:00 AM), respectively. The mean 24-hr urinary creatinine per kilogram of body weight was 21.7 ± 4.9 mg/kg. The average 24-hr urine volume was 1,403 ± 475 mL and the mean measured 24UNa was 143.9 ± 42.1 mEq (range, 87.1–239.4 mEq). The measured 24UNa of 13 of the participants was > 100 mEq. The mean urinary Na/K in all collected urine samples was 3.0 ± 0.89 (range, 1.29–4.64). Measured 24UNa was significantly correlated with estimated 24UNa using Tanaka's equation (r = 0.673, P < 0.01) and the Korean formula (r = 0.612, P < 0.05) in all collected urine samples.
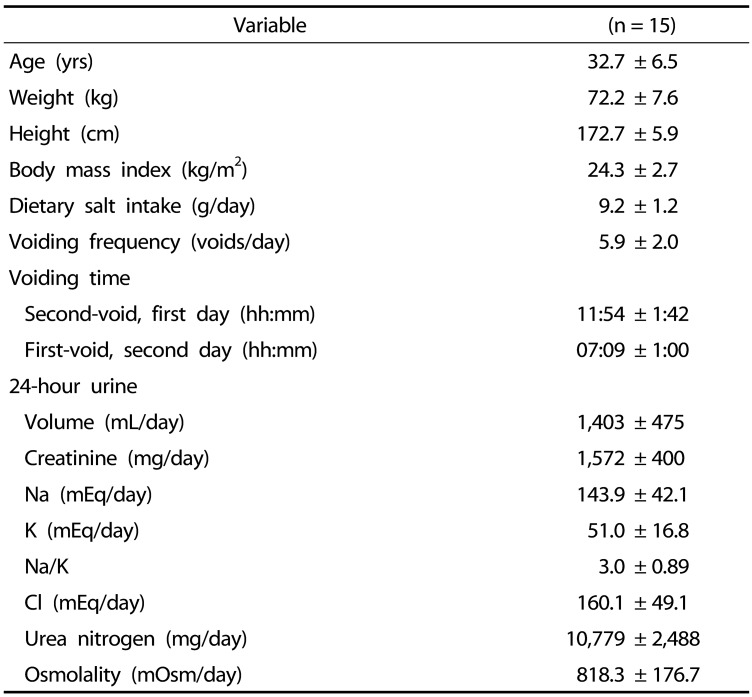

Table 1
Clinical characteristics of the subjects.
![]()
Table 2
Pearson's correlation coefficients (r) between measured 24UNa and demographic factors and urinary parameters according to time of urine sampling
![]()
Correlations between measured 24UNa, and demographic factors, urinary parameters, and estimated 24UNa in all spot urine samples
The mean urinary Na/K in all spot urine samples was 2.95 ± 1.29 (range, 0.43–6.04). Measured 24UNa was significantly correlated with urinary Na/UN (r = 0.560, P < 0.01), urinary Na/Osm (r = 0.510, P < 0.01), urinary Na/Cr (r = 0.392, P < 0.01), urinary Na/K (r = 0.290, P < 0.01), estimated 24UNa using Tanaka's equation (r = 0.452, P < 0.01) and the Korean formula (r = 0.414, P < 0.01), age (r = 0.548, P < 0.01), weight (r = 0.497, P < 0.01), and height (r = 0.393, P < 0.01) for all random urine samples (Table 2).
Correlations between measured 24UNa, and demographic factors, urinary parameters, and estimated 24UNa in the 2nd urine of the 1st day
The mean urinary Na/K in the second-void urine of the first day was 3.08 ± 1.35 (range, 1.45–5.91). Estimated 24UNa from the second-void spot urine of the first day tended to be more tightly correlated with measured 24UNa than the corresponding values from the other two spot urine samples, i.e., the first-void urine of the second day and all random urines. The following most significant correlations were seen for the second-void urine of the first day: urinary Na/K (r = 0.647, P < 0.01), urinary Na/Cr (r = 0.558, P < 0.05), and estimated 24UNa using Tanaka's equation (r = 0.616, P < 0.05) and Korean formula (r = 0.588, P < 0.05) (Table 2, Fig. 1, Fig. 2).
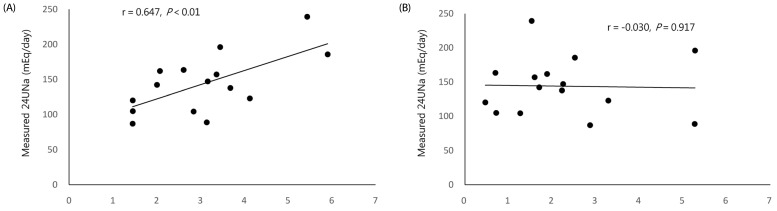 | Fig. 1Correlations between measured 24UNa, and urinary Na/K in the second-void spot urine samples taken on the first day (A) and in the first-void spot urine samples taken on the second day (B).Pearson's correlation coefficients and P-values are shown for each plot. Each line represents the linear regression for the plotted plot. 24UNa, 24-hour urinary sodium; Na, sodium; K, potassium.
|
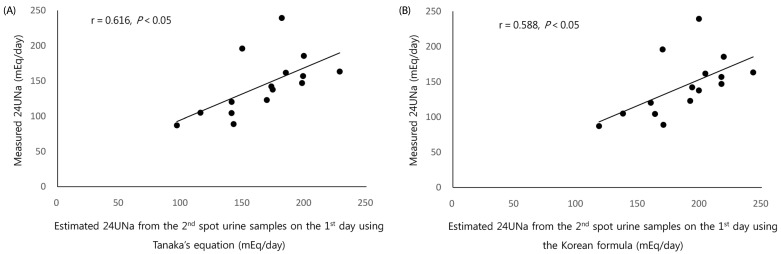 | Fig. 2Correlations between measured 24UNa and 24UNa estimated from Tanaka's equation (A) and the Korean formula (B) in the second-void spot urine samples taken on the first dayPearson's correlation coefficients and P-values are shown for each plot. Each line represents the linear regression for the plotted data. 24UNa: 24-hour urinary sodium.
|
Correlations between measured 24UNa, and demographic factors, urinary parameters, and estimated 24UNa in the 1st urine of the 2nd day
The mean urinary Na/K in the first-void urine of the second day was 2.24 ± 1.47 (range, 0.47–5.28). The first-void morning urine of the second day gave unexpectedly poor correlations compared with all collected urine, all random urine and the second-void spot urine of the first day. Only urinary Na/SG (r = 0.596, P < 0.05) was correlated with measured 24UNa (Table 2, Fig. 1, Fig. 3).
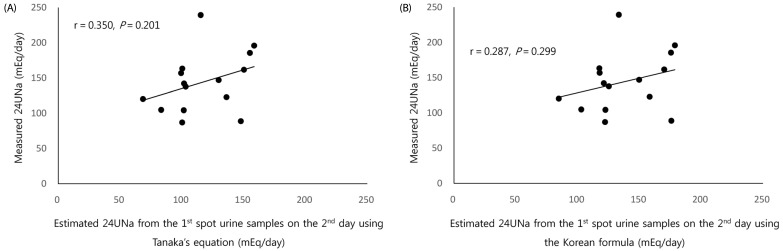 | Fig. 3Correlations between measured 24UNa and 24UNa estimated from Tanaka's equation (A) and the Korean formula (B) in the first-void spot urine samples taken on the second day.Pearson's correlation coefficients and P-values are shown for each plot. Each line represents the linear regression for the plotted plot. 24UNa: 24-hour urinary sodium.
|
Intra-personal variability of urinary parameters and estimated 24UNa
The percent coefficients of intra-personal variation (CV%) of all urinary parameters except Na/Cl were large compared to those of estimated 24UNa. The CV percentages for urinary Na/K, urinary Na/Cr and urinary Na/UN were 34.6 ± 10.1%, 39.9 ± 15.2% and 33.0 ± 10.3%, respectively, and those for estimated 24UNa using Tanaka's equation and the Korean formula were relatively small: 17.8 ± 7.5% and 15.9 ± 6.8%, respectively (Table 3).

Table 3
Coefficients of intra-personal variation for urinary parameters and estimated 24UNa in all random urine samples (n = 88) from the 15 participants
†Tanaka's equations [16]:
1) Estimated 24UNa_Tanaka (mEq/day) = 21.98 × ({spot urine Na (mEq/L) / [10 × spot urine Cr (mg/dL)]} × PRCr_Tanaka)0.392
2) PRCr_Tanaka (mg/day) = −2.04 × age (yr) + 14.89 × weight (kg) + 16.14 × height (cm) − 2,244.45
‡Korean formulas [17]:
1) Estimated 24UNa_Korea (mEq/day) = 28.985 × ({spot urine Na (mEq/L) / [10 × spot urine Cr (mg/dL)]} × PRCr_Korea)0.346
2) PRCr_Korea (mg/day) = −7.428 × age (yr) + 10.372 × weight (kg) + 15.631 × height (cm) − 1,234.785
Abbreviations: 24UNa, 24-hour urinary sodium; CV%, percent coefficient of intrapersonal variation; Na, sodium; K, potassium; Cr, creatinine; Cl, chloride; UN, urea nitrogen; SG, specific gravity; Osm, osmolality; predicted value of 24-hour urinary Cr, PRCr.
![]()
Go to :
DISCUSSION
The urinary Na/K ratio of the second-void urine taken around midday of the first day displayed the most significant correlation with measured 24UNa in fifteen adults that consumed an average of 9.2 g salt in one 24-hr session. Urinary Na/Cr, and estimated 24UNa by Tanaka's equation and the Korean formula were also significantly correlated with measured 24UNa. However, first-void morning urine did not yield good correlations except with urinary Na/SG.
The spot urine Na/K ratio is a useful estimate of the 24-hr urine Na/K ratio and has been suggested as an alternative method for assessing salt loading [1920], in both hypertensive patients and healthy individuals [2122]. Recent epidemiological studies have reported that the Na/K ratios in first-void morning urine and 24-hr urine are correlated with blood pressure [232425]. Observational studies have also shown that the urinary Na/K ratio is more strongly associated with increased blood pressure and subsequent cardiovascular disease than either Na or K alone [2627]. The correlation between the Na/K ratios for casual urine and 7-day 24-hr urine reached 0.80 for mean 4-day values and 0.87 for mean 7-day values [22]. In the current study, the urinary Na/K ratio of the second-void urine was also strongly correlated with measured 24UNa (r = 0.647, P < 0.01).
A further advantage of the urinary Na/K ratio was to determine whether patients consumed a low salt diet or not. If the urinary Na/K ratio was equal to or higher than 1 in patients with liver cirrhosis with ascites, the probability that random spot urine Na concentration was over 78 mEq was 90 to 95 percent [28]. In our study, the minimum 24UNa was 87.1 mEq and the minimum urinary Na/K of the second-void urine of the first day was 1.45. Although we performed this trial with healthy people, the result corresponded with a previous report on hypertensive patients [28]. Based on their own studies for hypertensive and healthy normotensive subjects, Iwahori et al. [212229] have suggested that the urinary Na/K ratio could be a robust monitoring tool for Na reduction and K increase in the normal population, as well as for patients during treatment.
Although first-void morning urine is widely used for measuring microalbuminuria and proteinuria, its accuracy for estimating urinary Na remains unconfirmed. Collecting first-void morning urine is also impractical due to difficulties associated with having just woken up. Mann et al. [18] reported that the urinary Na/Cr ratio in the late afternoon was strongly correlated with measured 24UNa. In another study, however, evening urine samples showed larger within-person variation in urinary Na and K excretion, along with day-to-day and diurnal variation [30]. Katama et al. [31] also reported that night-time urinary Na reflected 24UNa with a correlation of 78%. In our own present study, the intra-personal variability of each parameter was relatively high due to the great variability of first-void morning urine compared to those of other times. Because of this high variability and the difficulty in collecting first-void morning urine, second-void urine may be better for estimating 24UNa. Authors could not explain why estimating 24-UNa from the first-void urine samples did not show good correlation with measured 24UNa. It could be hypothesized that the second-void urine samples are likely to be a better estimation for the pulsatile circadian excretion of urine Na after dietary Na intake than the first morning fasting urine samples.
The strength of our study is that urinary Na and other urinary parameters were measured in every void of urine over 24 hours, along with 24-hr urine obtained by summing all voids. Furthermore, according to the Korea National Health and Nutrition Examination Survey (KNHANES VII-1) results for 2016, the average daily salt intake of Korean adults aged 19 years or older was 9.8 g [32]. The Korean population has high dietary salt consumption, and the participants in the present study consumed 9.2 ± 1.2 g of salt a day, which indicates that our results could be applicable to the entire adult population of Korea.
This study has the following four limitations. First is the very small sample size. Second, only healthy individuals were enrolled, so it is uncertain whether the results can be applied to patients with chronic diseases such as chronic kidney disease and congestive heart failure [33]. Since renal excretion and reabsorption of sodium can be affected by chronic diseases and medication [3334] the challenge to clarify the scope of application remains. Third, there were large variations in 24UNa, even though a comparable amount of salt was provided to all participants for this data. Among fifteen participants, ten consumed 10 g salt a day and the other five consumed 6–9 g salt a day. Twenty-four-hour (hr) urinary sodium may be affected by the sodium intake over the previous several days, which could induce the variation of the 24UNa in this study. Fourth, two formulas using a spot urine sample test for estimating 24UNa did not identify high Na consumption in 14% of cases [17]. However, this problem is not specific to our present study, although all previous studies using spot urine may have the same flaw.
In conclusion, despite these limitations, the strong correlation between urinary Na/K in the second-void urine around midday and 24UNa suggests that this test could be useful as a substitute for 24UNa, and for assessing compliance with dietary salt restrictions in population surveillance and in outpatient settings.
Go to :

 XML Download
XML Download