

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Although the incidence rate of gastric cancer has been steadily decreasing worldwide, some Asian countries including South Korea (hereafter “Korea”), Latin American countries, and some former Soviet European countries still exhibit high incidence and mortality rates of gastric cancer [1]. Gastric cancer is the most common cancer in Korea, and the third most common cause of cancer-related mortalities [2].
Risk factors of gastric cancer include behavioral and genetic factors and Helicobacter pylori infection [3]. In an analysis using cohorts of 45,000 twins, gastric cancer was found to be caused by behavioral factors (72%) rather than genetic factors (28%) [4]. Among behavioral factors, dietary habits, alcohol drinking, and smoking are associated with gastric cancer risk [3]. The International Agency for Research on Cancer, an affiliated organization of the World Health Organization (WHO), classifies alcohol as a Group 1 carcinogen [5]. Alcohol is broken down into acetaldehyde and acetate in the human body, and reactive oxygen species formed during this process damage the DNA and proteins, which promote carcinogenesis. Furthermore, alcohol acts as a solvent to increase intracellular infiltration of carcinogens, thereby contributing to the cancer development [6]. In gastric cancer, alcohol consumption is also categorized as a probable risk factor with strong evidence [7]. A previous meta-analysis on the association between alcohol consumption and gastric cancer has reported that heavy drinkers exhibited significantly higher gastric cancer risk compared to non-drinkers [8]. However, alcohol consumption was not associated with gastric cancer in case-control studies in Korea [910], and controversial results were found in cohort studies [11121314]. Moreover, studies have been reporting controversial outcomes globally [151617181920]. The annual alcohol consumption in Korea is 10.2 L per person, which is higher than that in America, Japan, and China and the second highest in Asian countries, after Laos [21]. Since Koreans exhibit high incidence and mortality rates of gastric cancer, alcohol consumption studies in Korean population are necessary to identify the association between alcohol consumption and gastric cancer risk. Moreover, the frequency and amount of alcohol consumption differs with sex. Women are more vulnerable to the effects of alcohol due to the lower water content in the body as compared to men, even if the amount of alcohol consumed is the same as in men [22]. Therefore, the association between alcohol consumption and gastric cancer risk may differ with sex.
This study examined the association between gastric cancer risk and the status, frequency, and amount of alcohol consumption in Korean population using a case-control study. In addition, potential differences in the association between gastric cancer risk and alcohol consumption were assessed according to sex.
SUBJECTS AND METHODS
Cases and controls
This study included 440 cases (aged ≥ 20 years) newly diagnosed with gastric cancer via gastroscopy and biopsy at Chungnam University Hospital and Hanyang University Guri Hospital between January 2003 and August 2006. Patients aged ≥ 80 years were excluded from the study due to the possibility of practical difficulties in interview and recall of previous experiences. In total, 485 controls who were admitted to the hospital for non-gastric diseases, were selected within the same study period (± 1 year) from the same hospitals with cases. The absence of gastric cancer in controls was confirmed via gastroscopy. Cases and controls were matched based on their admission period (± 1 year), age (± 5 year), sex, and hospital. Finally, 316 case-control matched pairs (126 pairs in Chungnam University Hospital and 190 pairs in Hanyang University Guri Hospital) were included in this analysis.
All study participants received relevant information regarding the study and voluntarily provided written consent to participate in the study. All study contents and procedures were approved by Hanyang University Hospital Institutional Review Board (IRB) (IRB no. 2003-4).
Data collection
To minimize information bias, trained interviewers conducted face-to-face interviews with patients suspected to have gastric cancer, prior to the final diagnosis based on biopsy results. Questionnaires used consisted of questions regarding sociodemographic characteristics (sex, age, education level, etc.), lifestyle habits (alcohol drinking and smoking habit), family history of gastric cancer (first-degree relatives), and dietary factors (dietary habits and food frequency questionnaire).
Questions regarding alcohol consumption included the current status on alcohol drinking (non-drinker, past-drinker, and current drinker), the age at which one started and stopped alcohol consumption, and the total period (years) of alcohol consumption. Furthermore, the frequency and one-time amount of alcohol consumption for 1 year in the last 3 years before the interview were investigated for each type of alcoholic beverage (i.e. soju, beer, western liquor, makgeolli, rice wine, and others). The reason for setting the reference period of alcohol drinking for 1 year in the 3 years before the interview is that cases may have changed their alcohol drinking habits owing to signs of poor health status before the gastric cancer diagnosis. Participants were asked to provide an appropriate answer for alcohol consumption frequency from 9 options (“none/less than once per month”; “once a month”; “2–3 times per month”; “once a week”; “2–3 times per week”; “4–6 times per week”; “once every day”; or “≥ 2 times per day”). To assess the amount of alcohol consumption, the most commonly used units for each type of alcoholic beverage were used (i.e., soju, soju shot glass; beer, beer glass; western liquor, liquor glass; makgeolli, bowl; and rice wine or others, 200 mL cup).
The alcohol amount (g) per unit for each type of alcoholic beverage was calculated based on the alcohol content in the early 2000s when this survey was conducted (soju, 22%; beer, 4.5%; western liquor, 40%; makgeolli, 6%; and rice wine or others, 13%) [23]. The total daily alcohol amount was calculated by multiplying the daily consumption frequency with the alcohol amount (g) in each type of alcoholic beverage and adding the multiplication results. Based on the alcohol consumption criteria according to sex as suggested by the WHO [24], daily alcohol amounts were categorized into 4 groups (non-drinkers, past drinkers, < 20 g/day for women or < 40/day for men, and ≥ 20 g/day for women or ≥ 40 g/day for men).
Medical records were accessed to identify the height (cm) and weight (kg) of cases and controls. Body mass index (BMI, weight [kg]/height [m2]) has been categorized into 4 groups (underweight, ≤ 18.49 kg/m2; normal weight, 18.5–22.9 kg/m2; overweight, 23.0–24.9 kg/m2; or obese, ≥ 25.0 kg/m2) based on the standard for Asian population suggested by the WHO [25].
Statistical analysis
To compare the general characteristics of case and control groups, chi-square test and t-test were used. Odds ratio (OR) and 95% confidence interval (95% CI) were calculated using unconditional logistic regression, to compare the gastric cancer risk, according to the current status, frequency, and amount of alcohol consumption. The multivariate logistic regression model was adjusted for education level (≤ elementary school, middle school, ≥ high school, or missing), family history of gastric cancer (yes, no, or unknown), current smoking status (non-smokers, past smokers, or current smokers), and BMI (≤ 18.49, 18.5–22.9, 23.0–24.99, or ≥ 25 kg/m2). Dietary factors have been considered as a risk factor for gastric cancer, but dietary factors, such as energy, fruits, vegetable, vitamin C, and folate, did not show any significant association with gastric cancer risk in this study. In addition, these dietary factors were not related to alcohol consumption. Therefore, dietary factors were not considered as confounding variables in the multivariate analysis. To analyze the P-value for trend, median values of the frequency and amount of alcohol consumption were assigned to each category and used as continuous variables in the logistic regression model. All statistical tests were two-sided with α-error of 0.05 and performed using SPSS Statistics ver. 23.0 (IBM Corp., NY, USA).
RESULTS
General characteristics of cases and controls
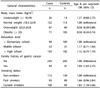
The general characteristics of the case and control groups are presented in Table 1. The number of men (208 cases, 65.8%) was higher than that of women (108 cases, 34.2%), and gastric cancer was most commonly observed in patients aged 60–69 years. No difference in education level was observed between the two groups (P-value = 0.758). However, the prevalence of obesity was lower in the case group (22.5%) than that in the control (33.2%) (P-value < 0.001). Cases had more family history of gastric cancer (15.5%) than did the controls (9.8%), but the difference was not statistically significant (P-value = 0.098).
General risk factors related to gastric cancer
As shown in Table 2, after adjusting for sex and age, educational level was not significantly associated with gastric cancer risk (OR = 1.15; 95% CI = 0.74–1.79). However, gastric cancer risk was significantly lower in overweight (OR = 0.58; 95% CI = 0.39–0.88) and obese (OR = 0.50; 95% CI = 0.34–0.74) groups than that in the normal weight group. In addition, patients with family history of gastric cancer had a significantly higher gastric cancer risk than those without history (OR = 1.69; 95% CI = 1.04–2.74). Meanwhile, gastric cancer risk was significantly higher in current smokers than that in non-smokers (OR = 1.83; 95% CI = 1.10–3.06).
Alcohol consumption status and gastric cancer risk
In the multivariate analysis to examine the association between the current status of alcohol consumption and gastric cancer risk, past-drinkers exhibited higher tendency of gastric cancer risk than did non-drinkers, although this association was not statistically significant (OR = 1.69; 95% CI = 0.95–3.00). Meanwhile, current drinkers showed no association with gastric cancer risk (OR = 0.96; 95% CI = 0.63–1.45). Stratified results according to sex showed a similar tendency with the association between the gastric cancer risk and past or current drinking status in all participants (Table 3).
Alcohol consumption frequency and gastric cancer risk
Table 4 shows the gastric cancer risk according to the frequency of alcohol drinking per week. Drinkers of ≥ 5 times per week had an increased gastric cancer risk, but was not statistically significant (OR = 1.56; 95% CI = 0.92–2.64). Women who drank ≥ 1 time per week had an increased gastric cancer risk, but this association was also not statistically significant (OR = 2.18; 95% CI = 0.79–6.02).
Alcohol consumption amount and gastric cancer risk
Table 5 shows the association between alcohol amount (alcoholic g/day) and gastric cancer risk. Among all participants, higher alcohol consumption (≥ 20 g/day for women or ≥ 40 g/day for men) was significantly associated with gastric cancer risk (multivariate OR = 1.73; 95% CI = 1.05–2.85). In the stratified analysis by sex, men showed an increased tendency of gastric cancer risk in participants who drink ≥ 40 g/day of alcohol compared to non-drinkers, but this was not statistically significant (OR = 1.65; 95% CI = 0.90–3.03). Meanwhile, women who consumed ≥ 20 g/day of alcohol exhibited a significantly higher gastric cancer risk than did non-drinkers (OR = 5.62; 95% CI = 1.32–23.81), which was higher than the effect size in men.
Soju consumption and gastric cancer risk
Table 6 shows the association between consumption (shot glass/day) of soju, the most favorite type of alcoholic beverage, and gastric cancer risk. Participants who drank soju of > 3 shot glasses per day showed increased gastric cancer risk, although this was not statistically significant (OR = 1.52; 95% CI = 0.94–2.47). In a stratified analysis by sex, the gastric cancer risk was slightly higher in men with > 3 shot glasses of soju per day (OR = 1.54; 95% CI = 0.91–2.59) and women with > 1 shot glass of soju per day (OR = 2.55; 95% CI = 0.75–8.67), although it was not significant.
DISCUSSION
In this study, alcohol consumption status and frequency were not associated with gastric cancer risk. However, participants with higher alcohol consumption (≥ 20 g/day for women or ≥ 40 g/day for men) had a significantly higher gastric cancer risk than did non-drinkers. Especially in women, alcohol consumption of ≥ 20 g/day was associated with a greater increase in gastric cancer risk.
Alcohol consumption is an evident risk factor for certain cancer types, and a previous study has described that excessive long-term alcohol consumption contributed to further increase in cancer risk [26]. Excessive alcohol consumption reduces food intake and intake of essential nutrients, and alcohol and its metabolites inhibit appropriate absorption, digestion, and usage of nutrients [2728]. This leads to reduced bioavailability of nutrients preventing cancer, which increases cancer risk [29]. Furthermore, excessive alcohol consumption inhibits the absorption and metabolism of folic acid, thereby increasing the demand for folic acid intake [30]. Low folic acid intake has been reported to induce DNA hypomethylation and damage DNA synthesis, eventually increasing cancer risk [3132]. Certain types of alcoholic beverages contain additives (i.e., flavoring agents and preservatives) and natural products (i.e., acrolein, phenol, and ketones), which may contribute to the carcinogenic process [29]. Owing to these reasons, excessive alcohol consumption has been reported to increase the risk of upper digestive organ cancers [33].
In this study, the current status of alcohol consumption was not significantly associated with gastric cancer. However, past-drinkers showed an increased tendency of gastric cancer risk when compared with non-drinkers (OR = 1.69; 95% CI = 0.95–3.00). This observation is probably due to the discontinuation of alcohol consumption in patients in the case group after experiencing a sign of poor health status, although they did not know their disease condition. A Korean Multi-center Cancer Cohort study [12] and a Chinese case-control study [34] demonstrated that the current status of alcohol consumption was not significantly associated with gastric cancer, but pastdrinkers were significantly associated with gastric cancer risk or cancer-related mortality. Another previous case-control study in Venezuelan men indicated that both current and past drinkers were significantly positively associated with gastric cancer risk - more specifically, past drinkers had higher effect size on gastric cancer risk [35]. On the contrary, other studies have demonstrated no significant association between gastric cancer and either current drinking or past drinking [193637]. In addition, lifetime duration of alcohol consumption was not associated with gastric cancer risk (OR = 0.98; 95% CI = 0.61–1.56 for alcohol consumption during ≥ 31 years vs. non-drinkers, data not shown).
A Korean Multi-center Cancer Cohort study assessing the association between alcohol consumption frequency and gastric cancer has shown that drinking ≥ 7 times per week was positively associated with the risk of gastric cancer mortality, although drinking 4–6 times per week showed no significant association [38]. In addition, another cohort study on Western European men, during the 15- and 30-year follow-up, reported that drinking ≥ 2 times per week was associated with increased gastric cancer risk [39]. However, alcohol consumption frequency was not significantly associated with gastric cancer in a Japanese cohort study [19]. In our study, although participants drinking ≥ 5 times per week demonstrated a tendency of increased gastric cancer risk, it was not significant (OR = 1.56; 95% CI = 0.92–2.64). Even if the alcohol consumption frequency is high, small amounts of alcohol consumption may allow the body to completely dissolve the alcohol and prevent the induction of toxicity. Therefore, the amount of alcohol consumption may be more important than frequency.
In this study, higher alcohol consumption (≥ 20 g/day for women or ≥ 40 g/day for men) significantly increased the gastric cancer risk (OR = 1.73; 95% CI = 1.05–2.85). A Korean Multi-center Cancer Cohort study showed that drinkers who consumed ≥ 72.01 g/day (≥ 504.01 g/week) of alcohol had 2.93-fold higher risk of gastric cancer mortality than did those who consumed 0.01–9.9 g/day of alcohol [12]. Another European cohort study demonstrated that alcohol drinkers who consumed ≥ 60 g/day exhibited 1.65-fold higher gastric cancer risk than did those who consumed 0.1–4.9 g/day [40]. A meta-analysis of relationship between alcohol consumption and gastric cancer showed that alcohol consumption of ≥ 30 g/day exhibited 1.58-fold increased gastric cancer risk [41]. Meanwhile, other case-control [910163536] and cohort studies [151942] did not show a significant association between alcohol consumption and gastric cancer.
When the association between alcohol consumption and gastric cancer was stratified by sex, alcohol consumption of ≥ 40 g/day was positively associated with gastric cancer risk in men, although not statistically significant (OR = 1.65; 95% CI = 0.90–3.03). Meanwhile, alcohol consumption of ≥ 20 g/day in women remarkably increased the gastric cancer risk (OR = 5.62; 95% CI = 1.32–23.81). A National Health Insurance Corporation cohort study on Korean men demonstrated that alcohol consumption of ≥ 25 g/day significantly increased the gastric cancer risk by 1.2-fold [11]. Another cohort study on Western European men (30-year follow-up) reported that participants with alcohol consumption of ≥ 100 g/week showed 1.9-fold higher association with gastric cancer than did those with alcohol consumption of 0.1–9.9 g/week. Moreover, their 15-year follow-up outcomes showed that both groups with alcohol consumption of ≥ 25 g or ≥ 100 g/week exhibited 2.06-fold and 2.74-fold increased association with gastric cancer, respectively, as compared to participants with alcohol consumption of 0.1–9.9 g/week [39]. Meanwhile, other studies have shown that the amount of alcohol consumption was not associated with gastric cancer risk in men [183435]. A Kangwha cohort study on the Korean population reported that alcohol consumption was not associated with gastric cancer risk in men, whereas alcohol consumption of ≥ 12.0 g/week significantly increased the gastric cancer risk (2.59-fold) in women [13]. Meanwhile, another Swedish women cohort study also concluded that alcohol amount was not associated with gastric cancer risk [17]. Women have greater body fat and less body water as compared to men. Therefore, when men and women of the same weight drink the same amount of alcohol, the blood alcohol level is higher in women than in men [22]. Moreover, the concentration of alcohol dehydrogenase in the stomach was lower in women than that in men, which leads to low metabolic rate of alcohol in gastric tissues. Consequently, the blood alcohol level is higher in women [43], which may the reason for the higher gastric cancer risk, despite lower alcohol consumption, in women than that in men. Therefore, the effects of alcohol amount in gastric cancer risk may differ according to sex. Our study suggests that the amount of alcohol consumed shows greater association with gastric cancer risk compared with the current status and frequency of alcohol consumption.
In Korea, the most favorite type of alcoholic beverage is soju (58.2%), followed by beer (35.6%), as reported in 2001 [44]. In our participants, soju accounted for 80% of the entire alcohol consumption, and thus, the association between alcohol consumption from soju and gastric cancer risk was assessed. The result showed that those who drank soju of > 3 shot glasses per day showed increased tendency of gastric cancer risk, although not statistically significant.
Despite intriguing findings, a few limitations and bias were observed from the study design and sample size in this study. Cancer patients with a long latent period may have changed their alcohol consumption habits due to signs of poor health status, despite not knowing their disease condition. To consider this possibility, the 1-year frequency and amount of alcohol consumption were assessed in the last 3 years before the interview, which may induce a high recall bias. However, according to Liu et al. [45] study, excessive drinkers showed a tendency to under-report the amount of alcohol consumption for current status. Therefore, the assessment of previous alcohol consumption based on recall is evaluated as a good prognostic factor. In this study, the sample size to analyze the association between alcohol consumption and gastric cancer risk was calculated as 414 pairs of gastric cancer cases and controls, according to Schlesselman's equation for a matched case-control study (α-error = 0.05, β-error = 0.10, P0 = 0.36 [the rate of heavy episodic drinking] [46], and OR = 1.58 for heavy alcohol drinking vs. non-drinking [41]) [47]. However, the sample size included in the final analysis was smaller than the aimed samples because some cases and controls could not be matched by age, sex, or hospital where they were diagnosed. Moreover, gastric cancer risk was found to be decreased in overweight and obese participants in this study. However, this is likely due to the weight loss commonly observed in patients with gastric cancer rather than obesity as a preventive factor for gastric cancer. H. pylori infection was examined using a rapid urease test (Product no: 60480, Kimberly-Clark, Ballard Medical Products, USA), known as Campylobacter-like organisms (CLO) test. However, the H. pylori infection test had a loss of approximately 32% due to failure of biopsy and the loss rate was very different in two hospitals. Therefore, H. pylori infection was not included as a confounding factor in the multivariate model. Because women who consumed ≥ 20 g of alcohol per day accounted for only 7.5% in this study and relatively small portions of women were current drinkers, further study with larger sample size of women is warranted. Lastly, since alcohol drinking rate in women has been recently increasing, additional studies should be performed using more recent data.
In conclusion, gastric cancer risk was not associated with the current status and frequency of alcohol consumption. However, excessive alcohol consumption (≥ 20 g/day for women or ≥ 40 g/day for men) significantly increased the gastric cancer risk. Alcohol consumption of ≥ 20 g/day can sufficiently increase the gastric cancer risk, especially in women. Since the Korean population has a high incidence rate of gastric cancer and high alcohol consumption, controlled alcohol consumption is needed to prevent gastric cancer.





 XML Download
XML Download