

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Tea is the most widely consumed beverage worldwide after water [1]. The tea plant, a species of evergreen (Camellia sinensis), is valued for its young leaves and leaf buds, which are used to produce the beverage. Tea types can be differentiated based on their manufacturing process, for example, ‘nonfermented’ green tea, ‘semi-fermented’ oolong tea, and ‘fermented’ black tea [2].
The association of tea and coronary heart disease (CHD) prevention has been the subject of controversy [3]. Most studies have found that tea consumption reduces the risk of cardiovascular morbidity and mortality [456]. By contrast, some studies have shown weak or no effect of tea consumption on the risk of cardiovascular diseases [78]. Meta-analyses have also obtained conflicting results. Hartley reported that green and black tea consumption could prevent the morbidity of cardiovascular disease [9]. However, another meta-analysis of tea consumption in relation to stroke, myocardial infarction, and all coronary heart disease (CHD) showed that there was an increased risk of CHD and stroke in populations with increased tea consumption [10]. A large prospective study showed that regular green tea consumption was associated with a significantly reduced risk of death from all causes, cardiovascular disease, and cancer among Chinese adults [11]. Unanswered questions from these studies include whether sex, age, type of tea, or the amount of tea consumed can produce these different results.
In the present study, we enrolled CHD and non-CHD patients to determine the association of tea consumption with CHD risk in the study population.
SUBJECTS AND METHODS
Patient and public involvement statement
This study was approved by the Ethics Committee of Sun Yat-sen Memorial Hospital (Approval reference: 2015 No.51) and complied with the Declaration of Helsinki. Informed consent was obtained from all subjects. This study was carried out on 267 CHD patients and 235 non-CHD controls at Sun Yat-sen Memorial Hospital between 2013 and 2014. CHD patients were diagnosed according to the international diagnostic criteria: (1) acute chest pain; (2) ischemic changes in exercise electrocardiography (ECG); and (3) ≥ 50% lumen diameter reduction in at least one major coronary artery on coronary angiography (ICA). The exclusion criteria were as follows: malignant tumor, hepatic and renal insufficiency, severe heart failure, and more than three complications. Non-CHD patients who had been hospitalized during the same period were recruited, and their exclusion criteria were similar to those for the CHD patient group.
Assessment of baseline characteristics
A pre-tested questionnaire was used to collect data for the name, place of birth, age, and sex of each participant. Hypertension, hyperlipidemia, and diabetes histories were recorded. Weight was measured to the nearest 0.01 kg using a bathroom scale (Hana, model BR9011; 120 × 0.01 kg, China). Height was measured in meters to the nearest 0.01 m using a height meter (Seca, model 206, Germany). Body mass index (BMI) was calculated for each subject. After a 10-min rest in the sitting position, blood pressure was measured. All of the indices were recorded by a trained interviewer.
Tea consumption assessment
Tea consumption was also examined by using a questionnaire. Beverage consumption was assessed by asking: “Did you regularly consume tea, including black tea, oolong tea, or green tea, during the last year?” Participants were also asked to select how often they consumed tea. Tea consumers were asked about the type of tea consumed, the amount of tea consumed per consumption period, frequency of tea consumption per week, and duration of tea consumption.
Statistical analysis
The baseline characteristics of the study participants were examined using t-tests for continuous variables and chi-squared tests for categorical variables. We included the various biomarkers individually into logistic regressions to assess p values after adjusting for sex, age, blood pressure, BMI, history of hypertension, history of hyperlipidemia, history of diabetes, as well as smoking, exercise, and nap behaviors, and wine consumption. An unconditional logistic regression was used to measure the association between tea and CHD. Odds ratios (ORs) were adjusted for BMI, age, blood pressure, history of hypertension, history of hyperlipidemia, history of diabetes, smoking, exercise, naps, and wine consumption. SAS software (Version 9.2, SAS Institute Inc.) was used for data analysis. A P < 0.05 indicated a significant difference.
RESULTS
Baseline characteristics of the study population
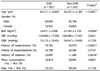
Out of 502 eligible participants, 267 were CHD patients and 235 were non-CHD patients (Table 1). Mean BMI was higher in CHD patients than in non-CHD patients. Moreover, the two groups' age distributions were different and compared to non-CHD patients, more CHD patients had histories of hypertension, hyperlipidemia, and diabetes.
CHD-related biomarkers in CHD and non-CHD patients
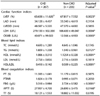
Regarding the cardiac function indices, left ventricular ejection fraction (LVEF) was worse in CHD patients than in non-CHD patients. Levels of lactate dehydrogenase (LDH) and creatine kinase of the muscle or brain type (CKMB) were higher in the CHD group than in the non-CHD group. Regarding the blood lipid index, the level of high-density lipoprotein cholesterol (HDL) was lower in CHD patients than in non-CHD patients. With regard to the blood coagulation indices, fibrinogen (FBG) and activated partial thromboplastin time (ATPP) were notably higher in CHD patients than in non-CHD patients (Table 2).
Tea consumption did not reduce the CHD risk in male participants
Tea consumption (seldom or regular tea consumption), type of tea consumed (none, partially fermented tea, or fully fermented tea), amount of tea consumed per unit time (none, 1–2 cups/time, or > 3 cups/time), frequency of tea consumed per week (none, 1–3 days/week, 4–5 days/week, or > 6 days/week), and duration of tea consumption (none, 0–10 years, 10–20 years, or > 20 years) were recorded and analyzed.
The results showed that men who drank tea did not have a reduced risk of CHD (adjusted OR = 1.672, 95% CI: 0.909–3.074, P = 0.0982). Different types of tea, specifically, partially fermented tea (adjusted OR = 1.592, 95% CI: 0.840–3.018, P = 0.1544) or fully fermented tea (adjusted OR = 1.926, 95% CI: 0.829–4.475, P = 0.1275), did not reduce the CHD risk. A tea consumption level of > 3 cups/time (adjusted OR = 1.477, 95% CI: 0.714–3.054, P = 0.2928) did not influence the CHD risk. A tea consumption frequency of 4–5 days/week (adjusted OR = 1.198, 95% CI: 0.563–2.549, P = 0.6395) or > 6 days/week (adjusted OR = 1.609, 95% CI: 0.772–3.351, P = 0.2041) also did not influence the CHD risk. Male participants with a green tea consumption history of 0–10 years (adjusted OR = 1.767, 95% CI: 0.676–4.617, P = 0.2453), 10–20 years (adjusted OR = 2.049, 95% CI: 1.000–4.196, P = 0.0500) or > 20 years (adjusted OR = 1.249, 95% CI: 0.584–2.668, P = 0.5665) also did not have a reduced risk of CHD (Table 3).
Tea consumption reduced the CHD risk in female participants
In contrast to the male results, the risk of CHD was reduced in women who drank tea (adjusted OR = 0.484, 95% CI: 0.242–0.968, P = 0.0403). The risk of CHD was also reduced in women who drank partially fermented tea (adjusted OR = 0.210, 95% CI: 0.084–0.522, P = 0.0008). Moreover, female participants who consumed 1–2 cups/day of tea had a reduced CHD risk (adjusted OR = 0.291, 95% CI: 0.131–0.643, P = 0.0023). A tea consumption frequency of > 6 days/week was also beneficial for CHD prevention (adjusted OR = 0.183, 95% CI: 0.049–0.679, P = 0.0112). In addition, female participants who had been drinking tea for 10–20 years (adjusted OR = 0.360, 95% CI: 0.137–0.946, P = 0.0382) had a reduced risk of CHD (Table 4).
DISCUSSION
Tea consumption has been shown to be useful for the prevention of many debilitating human diseases. Several published studies have reported similar results to those reported herein, showing that tea consumption can reduce CHD risk [1112]. In our study, we observed that tea consumption was associated with a reduced risk of CHD in female participants, but not in male participants, in Guangzhou, China. The protective association was related to the type of tea, the amount of tea consumed per unit time, the frequency of tea consumption per week, and the duration of tea consumption, as shown by the reduced CHD risks for partially fermented tea, 1–2 cups/time, > 6 days/week, and 10–20 years of tea consumption, respectively.
There is evidence indicating that catechins, which are the main polyphenolic compounds in tea, are responsible for the inverse association between tea consumption and CHD in women. Previously, tea catechins were shown to be associated with a reduced risk of CHD [13]. It was also shown that a tea catechin extract significantly reduced the circulating total cholesterol (TC) and LDL-cholesterol concentrations in women [1415]. Higher catechin antioxidant activities have been observed in female animals compared to that in male animals [16]. Catechins have conferred cardio-protection in the case of ischemia/reperfusion injury [17] and have provided vascular benefits that influence both CHD and cerebrovascular diseases. In our study, we found that tea consumption was associated with a reduced risk of CHD in female participants but not in male participants in Guangzhou, which was consistent with a previous canonical study [18].
Furthermore, in this study, the inverse association between tea consumption in women and CHD risk was related to the type, amount, frequency, and duration of tea consumed, which were partially fermented tea, 1–2 cups/time, > 6 days/week, and 10–20 years of tea consumption, respectively. Fully fermented tea (black tea) contains fewer antioxidant compounds, such as caffeine or catechins, than those in partially fermented and nonfermented teas (green tea and oolong tea). In addition, most catechins are oxidized by fermentation to thearubigins and theaflavins, which have reduced antioxidant properties, and black tea (fully fermented) has lower antioxidant properties than green tea or oolong tea (partially fermented) [19]. Our results show that 1–2 cups/time and > 6 days/week consumption of partially fermented tea has a lowering effect on CHD risk in women.
The results suggest that drinking tea is a good habit for CHD prevention. However, drinking too much tea might cause insomnia, which is a risk hazard for CHD [20]. In our study, consumption of > 3 cups/time contributed to the absence of an inverse association between tea consumption and CHD. However, we did observe that only 10–20 years of tea consumption could reduce CHD risk.
The underlying reason for the differences between our results for men and women might be the presence of a “critical time window” for the prevention of CHD in women. In our study, we observed a similar temporal phenomenon. Women who had been drinking tea for 10–20 years but not those who had been drinking tea for more than 20 years had a reduced risk of CHD. The mechanisms involved in this “critical time window” need to be clarified in the future.
We also observed that CHD-related biomarkers, namely, cardiac function indices (LVEF, LDH, and CKMB), blood lipid index (HDL), and blood coagulation indices (FBG and APTT), were worse in the CHD group than in the non-CHD control group. When analyzing the reasons behind these differences, we first detected that the cardiac function indices (LVEF, LDH, and CKMB) were worse in the CHD group than in the non-CHD control group. Studies have shown that tea polyphenols promote cardiac function and energy metabolism in ex vivo rat heart with ischemic/reperfusion injury. Second, tea consumption could decrease triglyceride and cholesterol levels to reduce serum lipid concentrations. Third, the blood coagulation indices (FBG and APTT) were worse in the CHD group than in the non-CHD control group. Studies have shown that the green tea polyphenol epigallocatechin has notable dose-dependent antiplatelet activity and blood anticoagulation effects. The above reasons might indicate some aspects of the mechanisms behind the beneficial effects of tea consumption.
There are a few limitations associated with this study. First, the number of patients in our study was limited; thus, larger scale studies are needed. Second, the proportion of the Guangzhou population that consumes tea may not be representative of that of the average population across China. Third, our study had a retrospective design. Prospective studies could better illustrate the association between tea consumption and CHD incidence. Moreover, we did not consider other potential confounding factors that may affect the outcome of CHD, such as consumption of wine and coffee, daily calorie intake, and CHD family history. Therefore, prospective studies are needed, and we suggest that future studies include an extended follow-up period for individuals who consume tea (because tea consumption pertains to CHD incidence) to ascertain long-term outcomes.
In summary, found that tea consumption was associated with a reduced risk of CHD in women (but in not men) in Guangzhou, China. The association was related to the type of tea consumed (partially fermented tea), the amount of tea consumed per unit time (1–2 cups/time), the frequency of tea consumed per week (> 6 days/week), and the duration of tea consumption (10–20 years of tea consumption).


 XML Download
XML Download