

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Renal transplantation is one of the renal replacement therapies for patients with end-stage renal disease. There are various advantages of kidney transplantation over dialysis, and the number of patients receiving renal transplantation is increasing. The mean lifespan and survival rate of renal transplant recipients have been increasing, and non-immunological factors, such as hyperlipidemia, hypertension, and diabetes, are important for long-term survival. The use of immunosuppressive drugs requires continuous dietary control and meticulous nutritional intervention to prevent obesity, hyperlipidemia, hypertension, diabetes, and osteoporosis [12].
The nutritional status before transplantation affects the prognosis after transplantation. Therefore, we aim to carry out an appropriate diet therapy according to the chronic kidney disease (CKD) stage and treatment before renal transplantation and maintain good nutritional status of the patient [34].
In the early period after transplantation, sufficient nutrition should be supplied because of the increased metabolic demand due to the stress caused by the use of high-dose immunosuppressive drugs. In the long-term nutritional management after transplantation, nutritional intervention is needed to prevent obesity, hyperlipidemia, hypertension, diabetes, and osteoporosis, which are the adverse effects associated with the use of immunosuppressive drugs [2].
The nutritional intervention process of kidney transplant patients which is performed by clinical dietitians at Samsung Medical Center is as follows.
Initial nutritional assessment is performed within 24 hours of hospitalization. After surgery, patients are kept nil per os for 2–3 days. Once the therapeutic diet starts, the explanation about the therapeutic diet is provided. Post-renal transplantation diet and post-renal transplantation dialysis diet are mainly prescribed, and low-potassium diet is also combined if necessary. Nutrition education is carried out for nutritional management after renal transplantation and before discharge, and the content is as Table 1.
Table 1
Contents of nutrition education

| Content of nutrition education |
|---|
| Maintenance of standard weight |
| Recommended dietary intake after transplantation (see Table 2 for estimation of recommended dietary intake) |
| Regular intake of balanced diet |
| Control of salt intake, reduction of simple sugar and distribution of glucose intake |
| Healthy fat intake methods |
| Increased fiber intake |
| Restriction of herbal products and botanicals |
| Food hygiene |
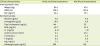
Table 2
Nutrient recommendations for adult KT

KT, kidney transplantation; BEE, basal energy expenditure; PUFA, polyunsaturated fatty acid; MUFA, monounsaturated fatty acid; DRI, dietary reference intake.
This table adapted from [5].
On postoperative day (POD) #15, nutritional re-assessment is performed, and if necessary, considering the nutritional status and calories they have taken, nutritional intervention is performed. After transplantation, patients who need management due to hyperglycemia receive additional nutrition education for blood glucose control before discharge. After discharge, follow-up education is continued according to the outpatient clinic visit day, if necessary.
CASE
A 57-year-old male patient underwent hemodialysis at a dialysis clinic because of CKD due to chronic glomerulonephritis. He underwent emergency hospitalization and deceased donor kidney transplantation (DDKT). On hospital day (HD) #2, the initial nutritional assessment was performed. The patient showed the following results: height of 165 cm, body weight of 63.6 kg (Information of edema status was not available), percent of ideal body weight (PIBW) of 106.2%, body mass index (BMI) of 23.4 kg/m2, albumin of 4.0 g/dL, and usual intake of > 90% of requirement. Thus, the nutritional status was evaluated as relatively good.
On POD #3, fasting was ceased, and the post-renal transplantation diet was started. Then, the explanation of the therapeutic diet, including diet name, necessity of the therapeutic diet, and cautions for the intake, was provided. We educated the patients on their current therapeutic diet. We carried out interviews with patients to identify their intake status and helped increase oral intake through meal adjustments reflecting their dietary preferences.
After POD #14, the patient was educated about renal transplantation nutrition education in groups which was performed every Wednesday. Patients were informed of the recommended intake level at each step, salt intake control, healthy fat intake methods, restriction of herbal products and botanicals, and food hygiene maintenance. After group education of about 30 minutes, a Q & A session was held, and supplementary explanations were provided individually as needed. The patient in this case consumed less than 80% of the recommended calories and loss weight. Thus, we encouraged him to increase his intake levels and take nutritional supplement drinks.
On HD #16, nutritional reassessment was performed. Considering the PIBW value of 100.3%, BMI of 22.1 kg/m2, and serum albumin of 4.0 g/dL, as well as his intake level, his nutritional status was relatively good. The need for sufficient intake of a balanced diet to maintain proper nutritional status after discharge was re-explained. The clinical characteristic of initial nutritional assessment and nutritional reassessment is shown in Table 3.
Table 3
Clinical characteristics
Two months after discharge, follow-up education was conducted at the outpatient clinic visit day. Follow-up education is usually conducted within one to two months after discharge, and the date of visit is scheduled according to the patient's request over the phone. Nutritional counseling for increased blood glucose after transplantation, persistent weight loss or weight gain after discharge, and elevation of blood lipid levels is mainly performed, and secondary follow-up education is conducted according to the degree of post-education correction. The patient in this case increased his dietary intake significantly after discharge, but he continued to ingest one-to-two cans of nutritional supplement drinks, resulting in an overall intake of 1.1 to 1.2 times more calories than the recommended calorie intake. Educational sessions regarding the necessity of proper weight maintenance and the recommended daily intake for long-term complication management after renal transplantation were conducted, and the patient was instructed to reduce nutritional supplement drink intake. The patient was re-educated regarding of after renal transplantation. This process is shown in Table 4.
Table 4
Summary of nutrition management during and after the hospital stay

DISCUSSION
Immediately after renal transplantation, the caloric requirement and proteins are increased due to the stress and catabolism because of the surgery. Since the stress from the surgery and the use of steroids may cause hyperglycemia, it is necessary to pay attention to simple sugar intake and regular intake of balanced diet. The use of immunosuppressive drugs may lead to hyperkalemia; therefore, potassium levels in the blood are carefully monitored, and if necessary, potassium intake is controlled. Hypophosphatemia frequently occurs in the early period after transplantation; thus, the intake of phosphorus-containing foods is increased. Nutritional intervention requires patient management through monitoring [267].
During the stabilization period, the appetite is increased due to steroids, and intake restrictions in terms of dietetic therapy are relaxed; thus, weight gain is likely to occur. Therefore, it is necessary to consume calories for maintaining normal weight. Arterial sclerosis, such as ischemic heart disease and stroke, is the leading cause of death in kidney transplant patients; therefore, kidney transplant patients should follow the dietary guidelines for dyslipidemia. Prolonged use of steroids increases the risk of osteoporosis, and sufficient calcium intake is thus recommended [278].
Since patients take immunosuppressive drugs for their entire lives, they should follow food safety guidelines to prevent food-borne infections [2].
To stabilize the nutritional status of the patients and familiarize them with dietetic therapies for preventing or alleviating the side effects caused by the use of immunosuppressive drugs, continuous patient management is needed not only during the hospital stay but also after discharge. The nutritional intervention of kidney transplant patients should be individualized according to the post-transplantation period and the nutritional status of the patient. It is also necessary to perform patient management according to a planned process for effective management.
 XML Download
XML Download