

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dietary reference intakes (DRIs) are reference values that guide the planning and assessment of nutrient intake in healthy populations [1]. The progenitor of DRI was the Recommended Dietary Allowances (RDAs) concept for energy, protein, and 8 vitamins and minerals, which was established in 1941 by the US National Research Council at the National Defense Advisory Commission [2]. RDAs were reference values that focused on preventing nutritional deficiencies [3]. According to the Institute of Medicine, RDA is “the average daily dietary nutrient intake level sufficient to meet the nutrient requirement of nearly all (97–98%) healthy individuals in a particular life stage and gender group” [4]. However, as various chronic diseases that were derived from excess or imbalance intake became major issues in public health in the mid-1990s, the need for a comprehensive approach for nutrient intake recommendations became apparent, which resulted in the new paradigm called DRIs [5].
Most countries or regions recommend nutrient intake values that are specific to their populations because there are different dietary cultures and environments, as well as health/disease problems, among different populations. Traditionally, these standards were set at a level that would cover the dietary requirements of practically all healthy persons in a given population. As new knowledge of human nutrient requirements has grown, these standards require reassessment and revision when appropriate. Therefore, most countries examine the status of scientific evidence and update their nutrient intake values periodically (about every 5–10 years) [6].
The initial Korean RDA (KRDA) for 10 nutrients, including energy, was published in 1962 by the Food and Agriculture Organization (FAO) Korean Office and has been periodically revised (the 7th revision was published in 2000) [7]. However, the need for new nutrient reference values has arisen as dietary and lifestyle changes have resulted in an increased prevalence of chronic diseases in the mid-20th century in Korea. Thus, in 2002, the Korean Nutrition Society (KNS) organized a committee to revise the KRDA and subsequently decided to expand the recommendation to the Dietary Reference Intakes for Koreans (KDRIs), in order to address the diverse issues related to nutrition. In 2005, the KNS officially established the KDRIs, which consisted of Estimated Average Requirement (EAR), Recommended Nutrient Intake (RNI), Adequate Intake (AI), Tolerable Upper Intake Level (UL) for nutrients, and Estimated Energy Requirement (EER) for energy and Acceptable Macronutrient Distribution Range (AMDR) of macronutrients [8]. The KDRIs were revised in 2010 by the KNS.
Since the National Nutrition Management Act was announced in 2010, the task for establishing and revising the KDRIs was conducted by the Korean Ministry of Health and Welfare (MOHW). Therefore, the MOHW recommended the task of revising the KDRIs to the KNS, and for the first time published the KDRIs at the national level in 2015 [9]. The 2015 KDRIs are publicly available on the MOHW website (http://www.mohw.go.kr). In particular, the committee for the establishment of the 2015 KDRIs put emphasis on an evidence-based multidisciplinary approach and the promotion of KDRI utilization.
The purpose of this article is to summarize the revision process for the 2015 KDRIs by focusing on the systematic review framework of scientific evidence.
MATERIALS AND METHODS
The development process of the 2015 KDRIs
DRIs should be developed from scientific evidence that includes their role in eliminating nutritional deficiencies and reducing the risk of chronic diseases [10]. Where adequate information is available, each nutrient has a set of DRIs. A nutrient has either an EAR and an RNI, or an AI. EAR and RNI are set when there is adequate information regarding the mean and standard deviation (SD) for the requirements of a given nutrient [9]. RNI is set to 2 SDs above the mean requirement, or a coefficient of variation is used instead of SD when insufficient data is available, such that 97.5% of the population's required intake would be below the recommended intake level [9]. When sufficient scientific evidence to derive the EAR and RNI cannot be obtained, the AI is used, which represents the adequate nutrient level for health [9]. UL is defined as “the highest average daily nutrient intake level that is likely to pose no risk of adverse health effects to almost all individuals in the general population” by the IOM [4]. UL is calculated based on the evidence of No Observed Adverse Effect Level (NOAEL), Lowest Observed Adverse Effect Level (LOAEL), and Uncertainty Factor (UF) [9]. The UL is determined only when there is evidence from the literature regarding adverse or toxic effects, such as NOAEL and LOAEL, from excessive intake of a given nutrient [9]. AMDR indicates appropriate ranges of intakes for energy sources among macronutrients, such as carbohydrates, proteins, and lipids, for the prevention of chronic diseases and nutritional imbalance [79]. EER means the estimated value of total energy intake for individuals, which is calculated by the predictive equation taking into account age, height, weight, physical activity level, and life cycle [79]. Table 1 shows the established components of the 2015 KDRIs by nutrients for individuals aged 1 year and older.
In Korea, an evidence-based research methodology has been applied to KDRIs for developing the appropriate reference values for the Korean population from the initial 2005 version of the KDRIs [8], with the first revision published in 2010 [11]. Evidence from new and relevant scientific reports has accumulated in recent decades, in addition to the systematic review framework for the United States and Canadian DRIs (e.g., Ca and Vitamin D) published in 2011 [12]. Therefore, the committee for developing the 2015 KDRIs applied the systematic review framework for establishing the 2015 KDRIs.
The committee for developing the 2015 KDRIs
The KNS, at the request of the Korean MOHW, assembled a steering committee to establish the KDRIs, based upon a rigorous and comprehensive review of the available scientific data. The KNS established a steering committee and a review board. The steering committee organized 6 subcommittees with a broad range of expertise (Fig. 1). The 6 subcommittees included: (1) age and physical standards; (2) standards for infants; (3) energy and macronutrients; (4) vitamins; (5) minerals; and, (6) applications of the KDRIs. The review board was organized by experts, who participated in establishing or revising previous KDRIs and reviewed both the procedures and results of the 2015 KDRIs development.
Age subgroups and physical standards for the 2015 KDRIs
Age and gender subgroup categories, as well as the physical standards for each subgroup, were revised for the 2015 KDRIs. To categorize age for the 2015 KDRIs, the committee reviewed the age group categories of the 2010 KDRIs and the available national statistics, including Korean statistical information and educational statistics. In addition, the committee considered the age group categories used for the DRIs of other countries for comparison. As a result, age was categorized into 13 subgroups; 0–5 months, 6–11 months, 1–2 years, 3–5 years, 6–8 years, 9–11 years, 12–14 years, 15–18 years, 19–29 years, 30–49 years, 50–64 years, 65–74 years, and 75 years and older.
Physical standards were derived from the data of Korea National Health and Nutrition Examination Survey 2008–2012, the Agency for Technology and Standards survey data (5th, 2003–2004; 6th, 2010), and the 2007 Korean growth chart, according to the age and gender subgroups of the KDRIs.
Nutrients included in the 2015 KDRIs
One of the important roles of the committee is to screen the target nutrients to be included in the KDRIs. Target nutrients are selected by the KDRI committee through an examination of the available scientific evidence and have extended its scope from 34 types of nutrients and energy in the 2005 KDRIs, to 36 types in the 2015 KDRIs [9]. Total sugars in 2010 and chromium in 2015 were newly added to their respective KDRIs. As a result, 2015 KDRIs included energy and 7 macronutrients (carbohydrate, sugars, lipids, protein, amino acids, total fiber, and water), 13 vitamins (vitamin A, D, E, K, C, thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, and biotin), and 15 minerals (calcium, phosphorus, sodium, chloride, potassium, magnesium, iron, zinc, copper, fluoride, manganese, iodine, selenium, molybdenum, and chromium) in the KDRIs (Table 1).
The systematic review process for the development of the 2015 KDRIs
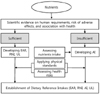
The KDRIs are quantitative nutrient reference values that reflect both adequate and safe upper levels of intake, and comprise the evidentiary base and reference standards that underpin government food and nutrition programs, policies, and regulation. This includes food fortification, nutrition labeling, food expenditure, and guidelines for food and nutrition assistance programs. KDRIs also serve as a basis for developing and revising national dietary and food guidelines. In addition, many other stakeholders use the KDRIs for health delivery, as well as education, research, and other program initiatives. Therefore, KDRIs should be based on scientific evidence of the association between nutrients and health outcomes, including basic requirements and the prevention of adverse effects. Particularly, the application of scientific evidence provides a foundation for establishing KDRIs (Fig. 2) and may improve the validity and reliability of KDRIs by making the best use of the existing scientific literature [9].
The 2015 KDRIs were developed by using systematic evidence review and analysis, based on the systematic review framework used by the Agency for Healthcare Research and Quality (AHRQ) and the Tufts Evidence-based Practice Center (EPC) for updating the 2011 DRIs for calcium and vitamin D [1213]. The systematic review framework for the 2015 KDRIs was adapted by the steering committee using the 3 following steps: (1) development of an analytic framework and refinement of key questions and search terms; (2) literature search and data extraction; and, (3) appraisal of the literature and summarizing the results. After development, the steering committee provided training on the systematic review framework to each subcommittee member at least once to assist them in fully understanding the framework and to be able to conduct the systematic review. Each subcommittee performed a literature search, evaluated the literature selected, and summarized the main findings following the developed framework. Subsequently, the main findings of the systematic review were used for the 2015 revision of the KDRIs. The contents of the systematic review framework for the 2015 KDRIs are described in detail in the following paragraphs.
Development of the analytic framework and refinement of key questions and search terms
An analytic framework is a visual map that shows a complex, connected structure of exposures, health outcomes (or clinical outcomes), biological functions of a given nutrient, modifying factors, and the population of interest, based on the existing scientific knowledge [14]. The analytic framework helps researchers consolidate and translate study results and plays a guiding role in the integration of information from a variety of sources [14]. In addition, it is useful in determining key questions in the next step of the process by summing-up the relationship between exposure and health outcomes in the analytic framework [14]. The analytic framework for DRIs includes 2 aspects of nutrient intake on health outcomes: beneficial effects and adverse effects [1213]. The analytic framework for beneficial effects is used for establishing EAR values, and the analytic framework for adverse effects is used to determine the UL values. For the development of the analytic framework, it is necessary to identify which biomarkers are appropriate to explain the underlying association between exposure and health outcomes through the existing scientific evidence. The analytic framework consists of 4 components: (1) exposures and/or sources (e.g., nutrient intake levels); (2) indicators of exposure reflecting nutritional status (e.g., blood concentration of the nutrient); (3) surrogate outcomes or intermediate outcomes that may predict or substitute for health outcomes (e.g., blood pressure, or blood cholesterol levels); and, (4) health outcomes or clinical outcomes (e.g., cardiovascular disease) [912]. Given that the relationship of these components varies for each nutrient, different analytic frameworks are needed for each nutrient of interest [15]. As an example for the 2015 KDRIs revision, the analytic framework components relevant to establishing the EAR and UL for folate are identified as follows.
Regarding EAR, the exposures (and/or sources) of folate were food, fortified foods, and supplements. The indicators of exposures were serum folate, red blood cell (RBC) folate, and plasma homocysteine. The surrogate or intermediate outcomes were megaloblastic anemia, gastrointestinal dysfunction, and depression. The health or clinical outcomes were pregnancy and childbirth, neural tube defects in the fetus, cardiovascular disease, development of some cancers, and delay of growth. Regarding UL, the exposures (and/or sources) were fortified foods and supplements. The indicators of exposures were serum folate and RBC folate. The surrogate or intermediate outcomes were not identified. The health outcomes or clinical outcomes were the neurological disorder, masking vitamin B12 deficiency, and lowering zinc status.
Based on the analytic frameworks, the next step is to formulate key questions regarding the relationship of the analytic framework components and then determine the key search terms [15]. Key questions define the objective and range that need to be covered prior to the literature search to achieve the objective and also limit the scope of a study at an early stage of research [15]. While key questions should be clearly articulated and specified [1415], these questions must be comprehensive in nature. Therefore, a collaborative process is required for formulating key questions, which embraces stakeholders, targeted users, and both authorities and committee members [14]. Also, the Population, Intervention or exposure, Control or Comparator, and Outcomes (PICO) strategy [16] is commonly used to enhance transparency and reliability in the process of developing key questions [15]. The committee for the 2015 KDRIs carefully determined the key questions that should be answered for setting reference values by considering the relationship between these indicators. For example, several key questions to set the reference values for folate were developed such as: “what effects do dietary folate and folic acid (folate supplements) have on serum folate, RBC folate, and plasma homocysteine level”; and “what effects does folate intake have on surrogate (intermediate) outcomes like megaloblastic anemia and health (clinical) outcomes like neural tube defects in the fetus”.
The committee for the 2015 KDRIs categorized the analytic framework components into 2 parts: the exposures (or sources) of nutrients, and the outcomes of interest. Using folate as an example, the key search terms for exposures were folate and folic acid, and the key search terms for health outcomes were megaloblastic anemia, neural tube defects, hyperhomocy-steinemia, cardiovascular disease, cancer or neoplasms, preterm or low birth weight, and breast milk or lactation. Then, terminology refinements, such as dealing with similar terms, were needed to determine both the final key search terms and the search strategies.
Literature search and data extraction
The literature search should be conducted using a well-structured search strategy with predefined criteria. The 2015 KDRIs committee searched articles using refined key search terms and search strategies through domestic search engines (KISS (Koreanstudies Information Service System), RISS (Research Information Sharing Service), NDSL (National Digital Science Library), DBpia), as well as international search engines (PubMed, Cochrane Library, EMBASE, Science-Direct, Scopus). Eligibility criteria of the target population, language, journal, publication year, and study design are described in detail below. All articles reviewed for the 2015 KDRIs only included articles that guaranteed quality using a peer-review system. The target population of study was healthy individuals, excluding infants under 6 months old. For infants, the subcommittee for infants independently conducted the literature review. There are English and Korean-language restrictions, but an exception was made in case of need for studies published in either Japanese or Chinese.
The availability of new and relevant scientific research was the primary consideration for establishing the 2015 KDRIs. Thus, the availability of relevant research published after 2008 was first examined to cover the period after the 2010 KDRIs. Then, the researches that were examined for the 2010 KDRIs were re-reviewed for establishing the 2015 KDRIs. Considering the strength and quality of scientific evidence according to each type of study [1718], the committee gave a high priority to the results from systematic reviews and meta-analyses and also examined intervention studies, cohort studies, and nested case-control studies. In addition, case-control studies and cross-sectional studies were included in the systematic review if the research was conducted with a Korean or Asian population. Retrieved articles without duplicates were first screened for eligibility through abstract review, and then the full-text of the articles were reviewed for inclusion in the systematic review. General information of the selected studies needed to be extracted and documented clearly, which includes information on the authors, article title, the journal of publication, and study design (Table 2), for assessing study quality and extracting study findings in the next step of the overall systematic review process.
Appraisal of the literature and summarizing the results
The final step in the systematic review framework for the 2015 KDRIs is to evaluate the quality of the selected studies and to summarize the main results of each study, as well as to provide reviewer comments on the study findings. The committee for the 2015 KDRIs considered a broad range of quality assessment tools that were verified internationally, according to each type of study design, for the appraisal of study quality [19]. The quality assessment tools used in the recent DRIs for calcium and vitamin D in the United States and Canada, the tools suggested by the Academy of Nutrition and Dietetics of the United States, and other tools widely used in the similar research field were examined thoroughly. Finally, 4 quality assessment tools were chosen for the systematic review for the 2015 KDRIs, as follows: (1) the Jadad scale [20] for intervention studies; (2) the Newcastle-Ottawa scale [21] for cohort, nested case-control, and case-control studies; (3) the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement [22] for cross-sectional studies; and, (4) A Mea Surement Tool to Assess systematic Reviews (AMSTAR) [23] for review articles. Along with the quality appraisal, study findings were concisely summarized in a specific table to serve as key evidence for the KDRIs. Data regarding the study findings for the 2015 KDRIs included study population, measures of exposure, intervention, outcomes, relative risk, and so on (Table 2).
RESULTS
Results of systematic review for 2015 KDRIs
Out of the total 203,237 retrieved articles for the 2015 KDRIs revision, 2,324 articles were included in the final systematic review (1,183 articles for energy and macronutrients, 619 articles for vitamins, and 522 articles for minerals) (Table 3). General information regarding the selected 2,324 articles such as authors, title, journal, and study design were extracted and documented in spreadsheets (Table 2). The information of excluded articles was also documented along with the reason for exclusion.
The committee made quality appraisals of the selected articles according to the manual of each quality assessment tool. The appraisal results were reported as scores with reviewer comments on the study evaluations, and the scores were converted to the score percentages out of the total scores as 100%. Table 4 shows the results of the quality appraisal according to each type of study design. On average, the score percentages of most studies were higher than a 60% total score percentage. For intervention studies, 799 studies were scored 3.0 (range, 0–5) points out of 5 total points on average. Cohort (n = 381), nested case-control (n = 67), and case-control studies (n = 107) were scored as 6.1 (range, 0–9), 6.0 (range, 3–9), and 5.4 (range, 1–8) points out of 9 total points, respectively. Cross-sectional studies (n = 660) received 14.6 (range, 0–22) points out of 22 total points and reviews (n = 310) were scored 7.0 (range, 0–11) points out of 11 total points (Table 4).
After the appraisal, data pertaining to the study findings were extracted and summarized in a table, along with the general information and appraisal results of the study. The results table concisely presents the study characteristics and findings, so that it assists the committee in translating the study outcomes to address the predetermined key questions [14]. Although the data components related to study findings are slightly different according to each type of study design, the results table for the 2015 KDRIs contained study populations, comparisons, measures of exposure, life stage, interventions, outcomes, relative risk, 95% confidence intervals, reviewer's comments, and the results of the quality appraisal (Table 2). The results tables functioned as the key evidence for setting the reference values of the 2015 KDRIs.
DISCUSSION
This study has comprehensively detailed the systematic review process for the development of the 2015 KDRIs. The 2015 KDRIs provide not only a basic guide for a balanced diet to promote health, but it is also an important standard for the evaluation of nutrient intake levels for Koreans [9]. To establish scientifically sound and reliable KDRIs, the decision making should proceed in a manner that is evidence-based and transparent. Unbiased systematic review plays an essential role in the decision-making process of the KDRI committee and facilitates the revision process of DRIs as additional findings are accumulated in the future [19]. For these reasons, the systematic review framework was developed and applied to the revision process for the 2015 KDRIs.
The incorporation of the systematic review framework into the revision process for the 2015 KDRIs was a complex task. However, considerable efforts on improving the framework should be continually developed to respond to global harmonization and the establishment of more elaborate KDRIs. There are several suggestions that may be considered to improve the systematic review framework for future KDRIs. First, an active discussion will be needed to include a wide range of chronic disease indicators into the analytic framework. The KDRI committee has made an effort to develop reference values for the prevention of chronic diseases and nutrient deficiency. To strengthen this effort, potential indicators related to chronic disease and nutrient exposure should be first identified. The potential indicators that can be incorporated into the analytic framework are the verified indicators that can be identified on the causal pathways between nutrient exposure and chronic disease [1]. However, it is difficult to identify these indicators for most chronic diseases [1]. Consequently, it requires an active discussion on how to select the appropriate chronic disease indicators, including proper surrogate indicators involved in chronic disease development (e.g., low-density lipoprotein-cholesterol for coronary heart disease) [24], and how to incorporate them into the analytic framework [1225]. Second, given the important role of selecting key questions that set the objectives and scope of the systematic review, it is desirable to encourage a broad participation of stakeholders, targeted users, authorities, and systematic review methodologists, as well as committee members, when developing the key questions [19]. Once the multi-sectoral team is organized, careful consideration is necessary to determine which topics should be addressed in setting KDRIs as the key questions [18]. Lastly, nutrition-specific quality assessment tools that reflect the characteristics of nutrition-based research could be introduced during the study quality appraisal stage [19]. The causal relationship between nutrient exposure and health outcome is more complicated than the relationship between pharmacologic treatment and health outcome [19]. In addition, there are unique kinds of covariates, confounders, and sources of error to consider in nutrition research [26]. Therefore, for a critical appraisal of each study regarding the association between nutrient exposure and health outcomes, especially more complex chronic diseases, the nutrition-specific assessment tools could be utilized. For example, a new nutrition-specific assessment tool can be developed by adding evaluation items reflecting the characteristics of nutrition research to the existing evaluation tools [2426].
In the process of revising DRIs, it is clear that the systematic review plays a key role, but the results of this process alone is not a substitute for the decision-making process of the review committee [12]. In other words, the systematic review is not the end of the committee's decision-making process, but is an integral part of the process for transparent and objective decision making [14]. Therefore, the systematic review framework for KDRIs should be constantly improved and developed as a useful tool to help decision making of the committee.
At present, many experts and researchers are still making a commitment to future KDRIs. The endeavors include not only improvements of the systematic review framework, but also the consideration of new approaches to establish reference values related to various chronic diseases, expansion of nutrients in KDRIs, response to population aging and global harmonization, and so on [30]. The effort for promoting the use and application of KDRIs should be made particularly through a close cooperation with professionals in government and fields. On the basis of the cooperation, it might be able to develop the dietary guidelines for Koreans, which is coordinated with KDRIs. Although the 2015 KDRIs were developed using evidence-based approaches, limited research evidence was available on the relationship between diet and health status in the Korean population. Given that the dietary recommendations and guidelines are applied to the dietary habit of the target population, further research about the Korean diet should be conducted for developing the next KDRIs.





 XML Download
XML Download