

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sentinel lymph node biopsy (SLNB) is a standard procedure in patients with breast cancer who have clinically negative lymph nodes. In comparison with initial axillary lymph node dissection (ALND), performing SLNB confers no significant differences in either disease-free survival (DFS) or overall survival (OS) [123]. However, ALND is performed when axillary lymph node metastasis is confirmed via SLNB. Compared with ALND, SLNB requires less time and a smaller operating field, and SLNB has fewer side effects (e.g., seroma, hematoma, pain, and lymphedema). Potential adverse effects of ALND can considerably worsen the quality of life of the patient [1234].
After the introduction of SLNB, there were some suggestions made about omitting ALND in some patients with positive SLNB results, as there was no difference in survival in early breast cancer regardless of the axillary surgery method [567]. However, the major limitation in these reports is that they were small, single-institutional studies. The American College of Surgeons Oncology Group (ACOSOG) Z0011 trial randomized patients with early breast cancer who had positive SLNB results into groups undergoing SLNB alone and SLNB+ALND; no difference was found in patient survival rates [8]. In a follow-up study in 2016, disease-specific survival (DSS), OS, and local recurrence rates were also similar between the groups, and there were no significant differences in the 10-year DFS and regional recurrence between the two groups [910].
Based on these results, we used data from the Korean Breast Cancer Registry to investigate DSS and OS rates in patients with early breast cancer, who had one or two positive axillary lymph nodes in the final pathology and who did or did not undergo ALND. Furthermore, we investigated the annual number and proportion of patients undergoing breast-conserving surgery (BCS), with SLNB or SLNB+ALND, among patients with one or two positive axillary lymph nodes. Our overall goal was to provide results that would be useful for future axillary surgeries in Korea.
METHODS
Study population
The data in the Korean Breast Cancer Registry were collected by the Korean Breast Cancer Society (KBCS) from 41 university hospitals and 61 training hospitals in Korea. In the present study, we used data for the cause and date of death from this database in connection with the Central Cancer Registry data of the Ministry of Health and Welfare in cooperation with the Korean National Statistical Office, to compile complete death statistics updated through 2014. This study was approved by Catholic Medical Center Daejeon St. Mary's Hospital Institutional Review Board (No. DC17RISE0006) and waived the requirement for obtaining informed consent.
Study design
The study included 131,717 patients diagnosed with breast cancer, who were registered in the KBCS database from 1995 to 2014. The following information was retrieved from the database: age; sex; menopausal status; date of surgery; method of breast surgery; method of axillary surgery; tumor size at the time of diagnosis; presence and number of lymph metastases; histological type; estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) status; use of chemotherapy, radiotherapy, hormone therapy, and targeted therapy; and mortality status. We categorized molecular subtypes as follows: luminal A-like means ER and/or PR positive and HER2 negative; luminal B-like means ER and/or PR positive and HER2 positive; triple-negative means ER and PR negative and HER2 negative; HER2-enriched means ER and PR negative and HER2 positive.
The inclusion criteria were as follows: (1) tumor stage 1 or 2 (tumor size ≤5 cm); (2) clinically negative axillary lymph node metastasis; (3) one or two positive axillary lymph nodes in the final pathology; (4) BCS; and (5) whole breast radiation therapy. Ultimately, 4,442 patients in the KBCS database satisfied these criteria. The 4,442 patients were divided into two groups: those who received SLNB (SLNB group) and those who received ALND after SLNB (SLNB+ALND group) (Figure 1).
The primary endpoint of this study was to determine whether there is any significant difference in DSS and OS between patients who underwent SLNB and those who underwent SLNB+ALND. The secondary endpoint was to describe the independent factors influencing DSS and OS.
Statistical analysis
The Student t-test was used to compare variables between the SLNB and SLNB+ALND groups. Intergroup comparisons of DSS and OS were verified via log-rank test, and prognostic indicators were identified using Cox regression analysis. Survival rates were determined from the date of diagnosis to the date of death due to breast cancer or any cause. The Student t-test was used to compare variables between the SLNB and SLNB+ALND groups. Intergroup comparisons of DSS and OS were verified via log-rank test, and prognostic indicators were identified using Cox regression analysis. Statistical analysis was performed using SAS version 9.3 (SAS Institute, Cary, USA), with a p-value <0.05 as the threshold for statistical significance.
RESULTS
Clinical characteristics
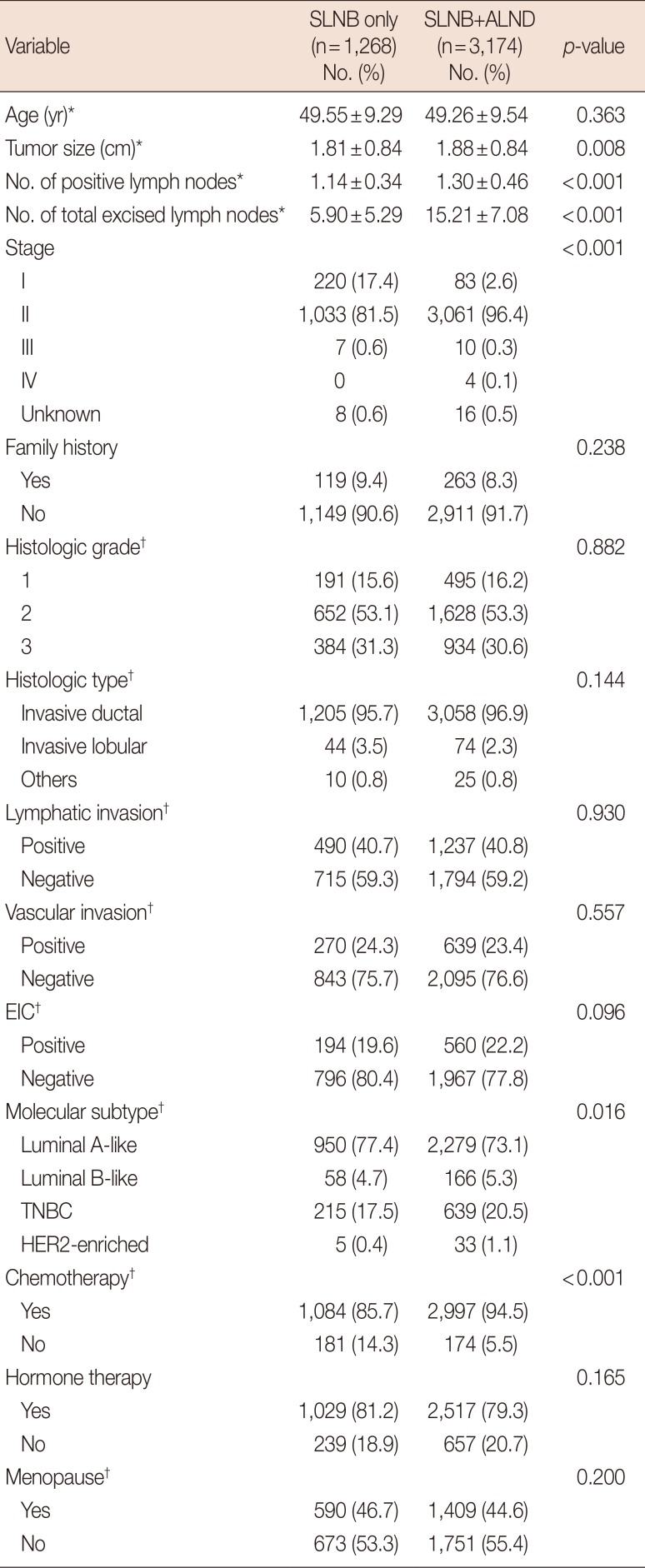
Among the 131,717 patients in the full dataset, 4,442 met the inclusion criteria, with 1,268 in the SLNB group (28.6%) and 3,174 in the SLNB+ALND group (71.4%). The clinical characteristics of the two groups are summarized in Table 1. The two groups differed in the number of positive lymph nodes (1.14±0.34 vs. 1.30±0.46, p<0.001), total number of lymph nodes removed (5.90±5.29 vs. 15.21±7.08, p<0.001), pathological stage (p<0.001), molecular subtype (p=0.016), and use of chemotherapy (p<0.001).
Survival outcomes
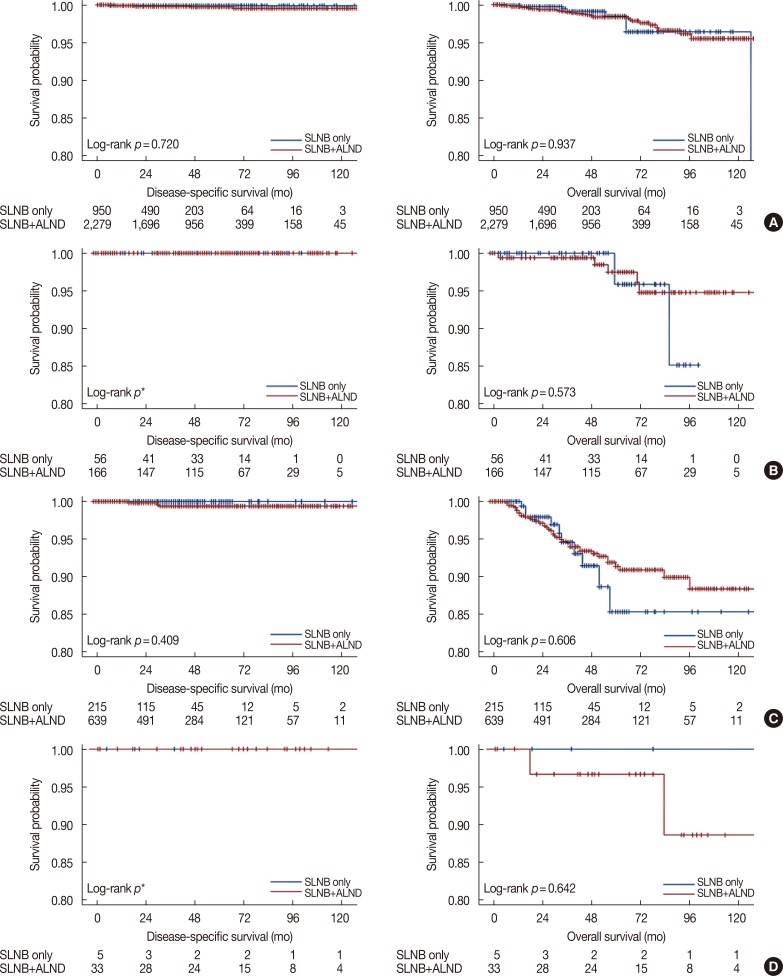
There were no significant differences in either DSS (p=0.378), or OS between the two groups (p=0.925) (Figure 2). The mean follow-up period for the SLNB and SLNB+ALND groups was 30.86±25.21 months and 47.24±30.56 months, respectively.
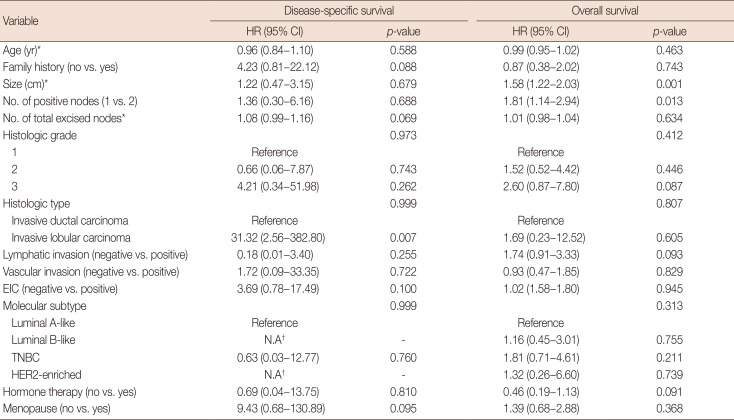
Factors associated with prognosis
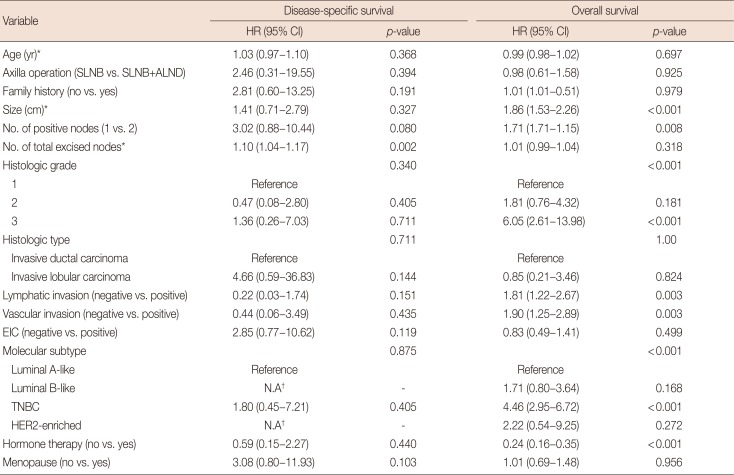
In the univariate analysis, total lymph node count correlated significantly with DSS; OS was correlated with tumor size, positive lymph node status, histologic grade, lymphatic invasion, vascular invasion, molecular subtype, and hormone therapy. In the multivariate analysis, histologic type correlated significantly with DSS; tumor size and positive lymph node status had a correlation with OS. The results for all variables are summarized in Tables 2 and 3.
Subgroup analysis according to molecular subtype
The relationship between the method of axillary surgery, and DSS and OS was assessed in the 4,442 patients. Study participants were categorized into the following subgroups: luminal A-like subtype (n=950), luminal B-like subtype (n=58), triple-negative (n=215), and HER2-enriched (n=5). There was no significant association between method of surgery and survival in any of the subgroups (Figure 3).
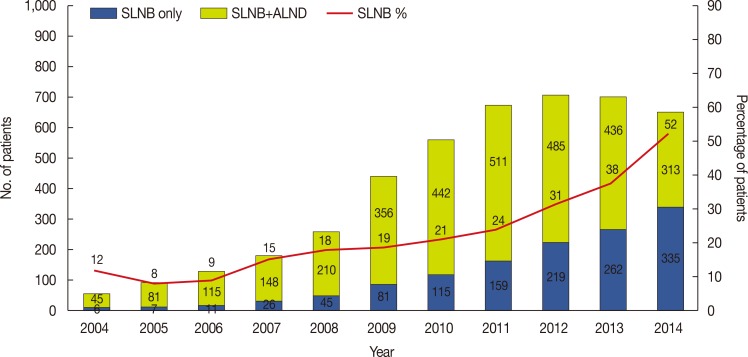
Annual incidence of SLNB alone or SLNB+ALND in patients with one or two positive axillary lymph nodes
The number of patients who underwent SLNB alone for one or two positive lymph nodes has increased gradually since 2004. The proportion of patients who underwent SLNB alone for one or two positive lymph nodes increased continuously from 2005 to 2014 (Figure 4).
DISCUSSION
Sentinel node biopsy could decrease morbidity in early breast cancer, and a previous study has shown that arm edema after axillary surgery occurs less frequently in patients who undergo mastectomy and do not undergo ALND than in patients who undergo ALND [11]. Previous studies have suggested that axillary recurrence is rare in early breast cancer; thus, SLNB without ALND may control axillary recurrence in selected patients [67]. Moreover, in patients with one to two positive lymph nodes on SLNB, DSS is not affected even when ALND is not performed [891213]. Therefore, omitting ALND can be helpful to patients if there is no benefit for survival.
Some studies have shown that performing SLNB under certain conditions may not affect survival [567]. To validate previous studies using a different approach, we retrospectively analyzed the study groups who underwent SLNB or SLNB+ALND. We included patients with only one or two positive lymph nodes in the final pathology, regardless of the type of axillary surgery. We excluded patients who were found to have further nodal metastases on subsequent ALND and were upgraded to N2/3 disease. This differed from the inclusion criteria in the ACOSOG Z0011 trial, in which 27.3% of participants underwent ALND and had additional metastases in the excised lymph nodes; such patients may have worse prognosis. At a median follow-up of 6.3 years in the ACOSOG study, 5-year OS was 92.5% with SLNB and 91.8% with SLNB+ALND [13]. In our study, with a mean of 47 months' follow-up, OS was 98.3% in the SLNB group and 97.3% in the SLNB+ALND group. Despite several differences in study design, the present study showed no significant difference in OS regardless of the method of axillary surgery, in patients with early breast cancer and one or two positive axillary lymph nodes who received BCS.
In a randomized trial conducted in 2010, the decision to perform ALND after SLNB during BCS was made based on the size of the tumor and the number of metastatic lymph nodes [8]. Since then, several studies have been published in which ALND was not performed in patients with early breast cancer who had one to two positive lymph nodes on SLNB, with no adverse effects on DSS rates; the subsequent use of ALND tended to decrease over time [141516171819]. In an analysis of Surveillance, Epidemiology, and End Results Program data, no differences were found in DSS or OS in patients with breast cancer (n=9,521) who did or did not receive ALND, including those with T1–T2 disease and ≥3 positive lymph nodes upon SLNB [20]. With those studies, the recommendations were updated in 2011 the new National Comprehensive Cancer Network (NCCN) guidelines [21]. However, the adoption and implementation of NCCN recommendations have been slow and irregular, and there is still reluctance to adopt this as the new standard for patients undergoing BCS for early breast cancer. We have no data in this regard for Korean patients with breast cancer. As seen in Figure 4, the increase in the number of patients who underwent SLNB alone was similar to previous studies. The decrease in the total number of patients who underwent BCS after 2014 was thought to be owing to an increase in the number of mastectomies and reconstructions. Despite decreasing BCS, the proportion of SLNB alone increased.
Among histologic subtypes, invasive lobular carcinoma is associated with DSS, but its incidence is rare in Korea, with only 3.5% in our study compared with 7.5% in the ACOSOG Z0011 trial. A study examining only invasive lobular breast carcinoma reported no effect of ALND on survival [22]. There are few studies on molecular subtypes, and one study revealed that ER or/and PR positive cases had significantly lower hazard ratios than both negative cases [10]. However, there was no difference in DSS and OS among molecular subtypes in our study. Tumor size, total lymph node number, and positive lymph node number were significantly higher in the SLNB+ALND group than in the SLNB group; because this study was a retrospective study, it was not possible to randomly assign the two groups.
In our study, the number of lymph nodes harvested was very high in the group undergoing SLNB (5.90±5.29). Based on the 7th edition of the American Joint Committee of Cancer (AJCC) staging criteria, six or more nodes removed constitutes axillary clearance [23]. The number of sentinel lymph nodes reported in other studies have not always followed the accepted definition [9242526], as these studies have mostly collected the data from the final pathology report. The disadvantage of such an approach is that even though pathological assessment might have been performed via SLNB during surgery, lymph nodes may have been obtained from the surrounding tissues, including some axillary lymph nodes. The total number of excised nodes was correlated with DSS in univariate analysis but not in multivariate analysis. The exact reason for this is difficult to determine due to the inherent characteristics of large databases. Additionally, the registry does not contain information about harvest methods for SLNB. The number of positive lymph nodes was a significant factor affecting OS in univariate and multivariate analysis; however, we only included patients with one or two positive nodes. We know that the number of positive nodes is a significant risk factor in the prognosis of breast cancer, although all cases with one to three positive axillary lymph nodes are classified as pN1a, according to the AJCC staging manual [21]. Further studies in patients who have several lymph node metastases are mandatory.
This study had some limitations. First, we cannot exclude selection bias owing to the retrospective nature of the study. The tumor stage, hormonal status, and prognosis were more favorable in the SLNB group, and more chemotherapy was administered in the ALND group; these factors could affect the statistical analysis results for the two groups. Secondly, some data might be incomplete or incorrect, with some cases described as stages 3 and 4. Despite these limitations, we consider the results of this study to be meaningful because they were obtained from a large number of patients of a single ethnicity, across multiple centers. Additionally, in patients meeting the inclusion criteria, the surgical methods did not affect survival rates in the subgroups or in the overall group. Our study is a retrospective study, but our findings can serve as basic data for future matched cohorts; a prospective randomized study is necessary to further investigate the need for ALND in this population.
In conclusion, Korean patients with early breast cancer who had one or two positive axillary lymph nodes and received BCS plus SLNB showed no significant differences in DSS and OS, regardless of whether they underwent ALND. The number of patients who underwent SLNB alone for one or two positive lymph nodes increased from 2004 to 2014 in Korea. Although follow-up studies are required, our study indicates that we can consider omitting ALND when treating selected patients with early breast cancer.


 XML Download
XML Download