

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The second most common cancer in Korean women is breast cancer, and there were 19,219 newly diagnosed breast cancer cases in Korea in 2015. Although there have been advancements in the understanding of the disease and its treatments, the incidence and mortality of breast cancer has increased constantly throughout the past 15 years in Korea [1].
Adjuvant radiotherapy (RT) is a well-established component of standard care for the management of patients with invasive breast cancer and ductal carcinoma in situ (DCIS) of the breast [23]. RT for breast cancer has changed dramatically in the recent two decades after multiple randomized trials. These trials have not only established new standards of care but have also raised additional questions about appropriate management [4]. Surveys on patterns of practice show variations in clinical practice amongst practitioners, and these results can assist in creating guidelines and identifying areas of controversy that drive future clinical trials [5]. Research groups from the United States, European countries, Australia, and China have reported a large degree of variation in practice patterns and there is controversy regarding the appropriate dose-fractionation schedule, application of regional nodal irradiation (RNI) and its coverage, and RT omission in patients at low risk of recurrence [456789]. The first Korean study on patterns of care for breast cancer was published in 2007, but its interest was limited to the evaluation and treatment in patients treated with mastectomy and postmastectomy RT (PMRT) [10]. No Korean group has conducted surveys on patterns of practice so far, although breast cancer is one of the most common diseases treated with RT [11].
The purpose of this study was therefore to report the patterns of national practice in RT for breast cancer in Korea, and to support the need for new evidence-based guidelines and future research.
Go to : 
METHODS
A nationwide survey on the patterns of practice in RT for breast cancer was designed by the Division for Breast Cancer of the Korean Radiation Oncology Group (KROG). The questionnaire-based survey comprised 39 questions on six domains: (1) hypofractionated whole breast RT (WBRT), (2) accelerated partial breast RT, (3) PMRT, (4) RNI, (5) RT for DCIS, and (6) RT toxicity. The questionnaire was piloted amongst the members of the Division for Breast Cancer of KROG, and minor modifications were made before starting the study. This study was conducted under the authorization and cooperation of the KROG.
All board-certified members of the Korean Society for Radiation Oncology were invited to participate in the study via e-mail in June 2017, and participation was voluntary. Study data collected was analyzed for each question to evaluate variations of practice in RT.
Go to :
RESULTS
Sixty-four radiation oncologists from 54 out of 86 (62.8%) hospitals responded in June 2017. Of the respondents, 53 (82.8%) worked for academic-affiliated hospitals and 37 (57.8%) worked for hospitals with more than two radiation oncologists, which qualifies a hospital as a radiation oncology training center. The respondents were divided based on the number of breast cancer patients they treated per month, with nine (14.1%) treating more than 30 breast cancer patients, 13 (20.3%) treating 21 to 30, 23 (35.9%) treating 11 to 20, and 19 (29.7%) treating fewer than 10. The respondents were also divided based on the number of years they had been practicing as radiation oncologists, with 24 (37.5%) practicing for more than 15 years, 11 (17.2%) practicing for 10 to 14, 14 (21.9%) practicing for 5 to 9, and 15 (23.4%) practicing for less than 5.
Hypofractionated whole breast radiotherapy for invasive breast cancer
Twenty-three radiation oncologists (35.9%) stated that they used hypofractionated WBRT in the management of early-stage breast cancer. Among the respondents who used hypofractionation, 12 (52.2%) stated that the use of hypofractionation was at the physician's discretion, and 11 (47.8%) stated that it was decided through a shared decision-making process. Seventeen respondents applied hypofractionation in WBRT only, and six applied it in both WBRT and RNI. Respondents stated that a younger age, left-sided breast cancers, triple-negative breast cancers, a history of chemotherapy, and other adverse pathologic features were contraindications for hypofractionation.
Most radiation oncologists applied more than 40 Gy mainly in 16 fractions, and used boost RT as well. The most common hypofractionation schedule prescribed was 43.2 Gy in 16 fractions, followed by 42.4 Gy in 16 fractions and 39 Gy in 13 fractions. Regarding RT technique, field-in-field technique (91.3%) was the most preferred, and intensity-modulated RT (39.1%) or three dimensional-conformal RT (39.1%) was often applied as well (Table 1).
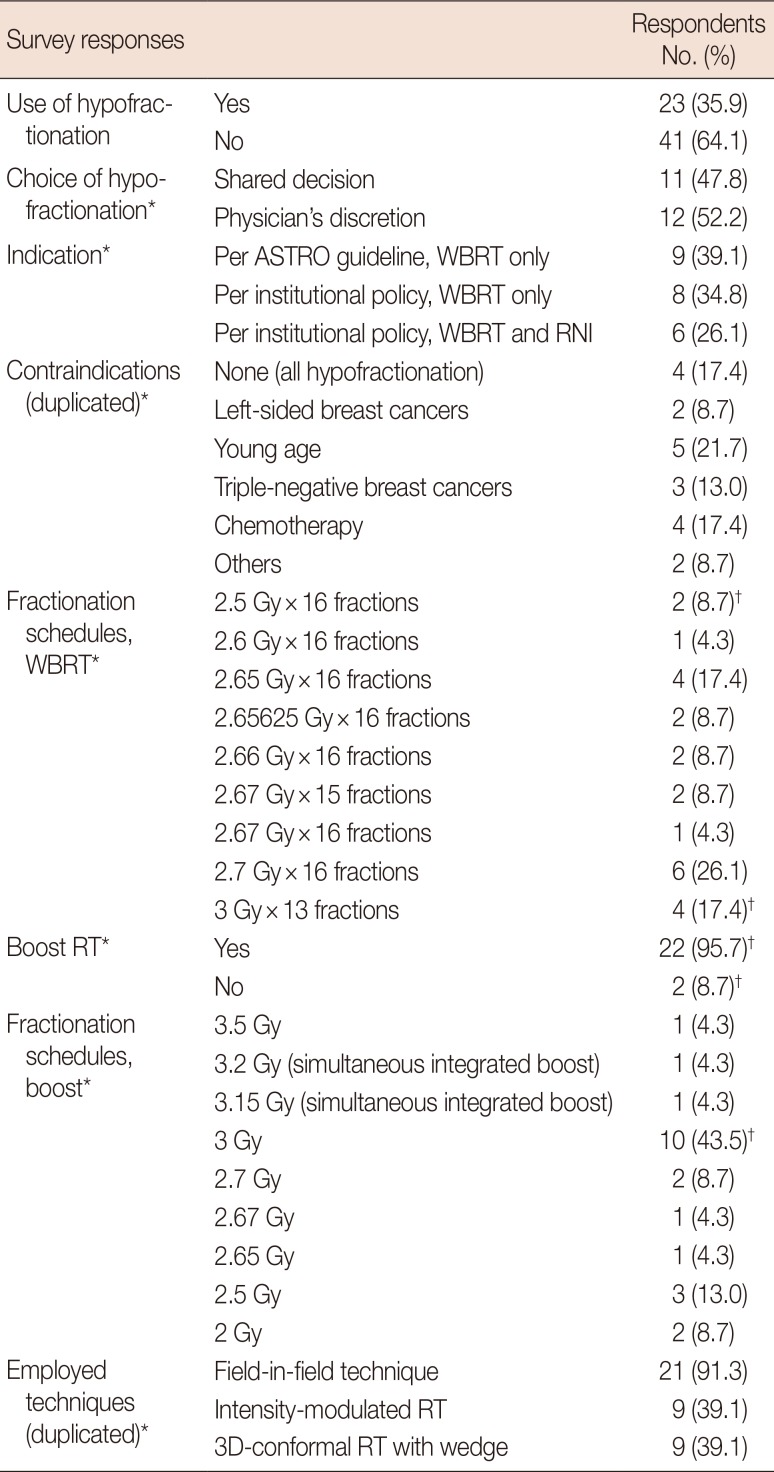
Table 1
Hypofractionated whole breast RT
RT=radiotherapy; ASTRO=American Society for Radiation Oncology; WBRT=whole breast radiotherapy; RNI=regional nodal irradiation; 3D=three dimensional.
*Percentage of respondents who responded “Yes” to use of hypofractionation; †A respondent used different fractionation schedules; 40 Gy in 16 fractions without boost RT or 39 Gy in 13 fractions with boost RT.
![]()
The reasons that 41 of the surveyed radiation oncologists did not use hypofractionation were as follows: they thought that it was not necessarily required in Korea, because of easy access to medical facilities, low medical costs for cancer patients, and widespread additional private insurance (43.8%); they were concerned about reimbursement, because the Korean healthcare service payment is on a fee-for-service basis (35.9%); and, they felt that the long-term data of hypofractionated WBRT was still insufficient (34.4%).
Accelerated partial breast radiotherapy
Only three radiation oncologists (4.7%) used accelerated partial breast RT. They all applied intensity-modulated RT, and one of them applied CyberKnife® (Accuray Inc., Sunnyvale, USA) as well. Different guidelines were followed for accelerated partial breast RT; one responder followed the American Society for Radiation Oncology (ASTRO) guidelines, one followed the ASTRO and Groupe Européen de Curiethérapie-European Society for Radiation Oncology guidelines, and one followed institutional policy.
Postmastectomy radiotherapy
Five radiation oncologists (7.8%) used hypofractionated PMRT. Fractionation schedules were 43.2 Gy in 16 fractions (n=2), 45.9 Gy in 17 fractions (n=2), and 40.05 Gy in 15 fractions (n=1).
Forty respondents (62.5%) had never used boost RT, but eight (12.5%) always used boost RT after chest wall irradiation. Sixteen respondents (25.0%) used boost RT selectively for close resection margins (n=14), pT4 (n=7), pT3 (n=2), and the presence of lympho-vascular space invasion (n=2). Forty respondents (62.5%) used bolus on either the entire chest wall or scar only. Twenty-eight (43.8%) and 46 (71.9%) did not use boost RT and bolus after breast reconstruction, respectively.
For RT techniques, standard or partial wide tangents were the most preferred (82.8%). Intensity-modulated RT, reverse hockey stick technique, and mixed photon and electron technique were applied as well (Table 2).
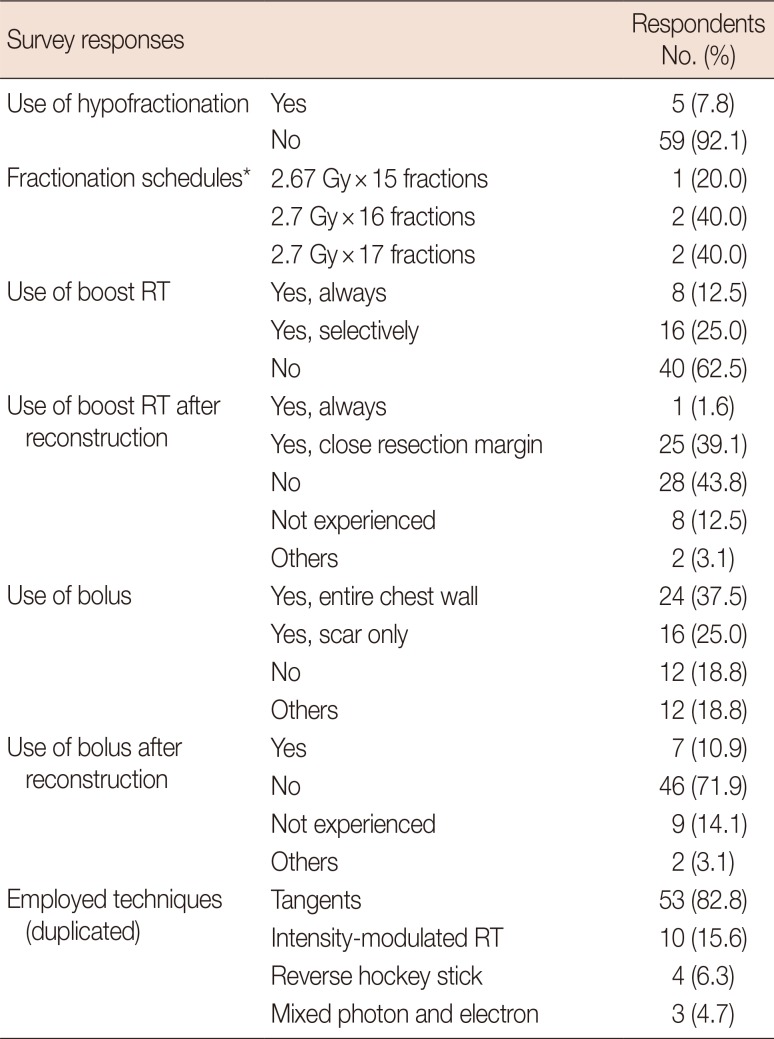
Table 2
Postmastectomy RT
![]()
Regional nodal irradiation
Seven radiation oncologists (10.9%) applied RNI only for patients with 4 or more axillary lymph nodes (LNs) involvement. Seventeen (26.6%) always applied RNI for patients with 1–3 axillary LNs involvement. However, the majority of the respondents (62.4%) additionally considered pathologic risk factors, such as LN-related parameters (number, axillar level, nodal ratio, and extracapsular extension), lympho-vascular space invasion, molecular subtype, and tumor size, along with axillary LN involvement.
The questionnaire provided a clinical case scenario of an early-stage breast cancer patient with 1–2 positive sentinel LN undergoing breast-conserving surgery (BCS) without further axillary dissection, simulating the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial. Eight respondents (12.5%) used standard tangents, and 32 (50.0%) used high tangents with or without supraclavicular LN (SCN) irradiation. Twenty (31.3%) included SCN and only two (3.1%) included internal mammary LN (IMN) in the RT field.
With regard to IMN irradiation when applying RNI, only four respondents (6.3%) always treated IMN, and 30 (46.9%) treated IMN only if IMN involvement was identified through imaging. Nine (14.1%) treated IMN for all patients with 4 or more axillary LNs involvement, but 25 (39.1%) additionally considered tumor location for decision making. Most of the respondents covered up to the third or fourth intercostal space for IMN irradiation. The most preferred RT technique for RNI was intensity-modulated RT for both WBRT (67.2%) and PMRT (54.7%).
Regarding posterior axillary boost (PAB) RT, 26 respondents (40.6%) did not apply PAB at all. Eleven (17.2%) applied PAB for all cases, and 24 (37.5%) considered PAB in cases of insufficient dose delivery to axilla (Table 3).
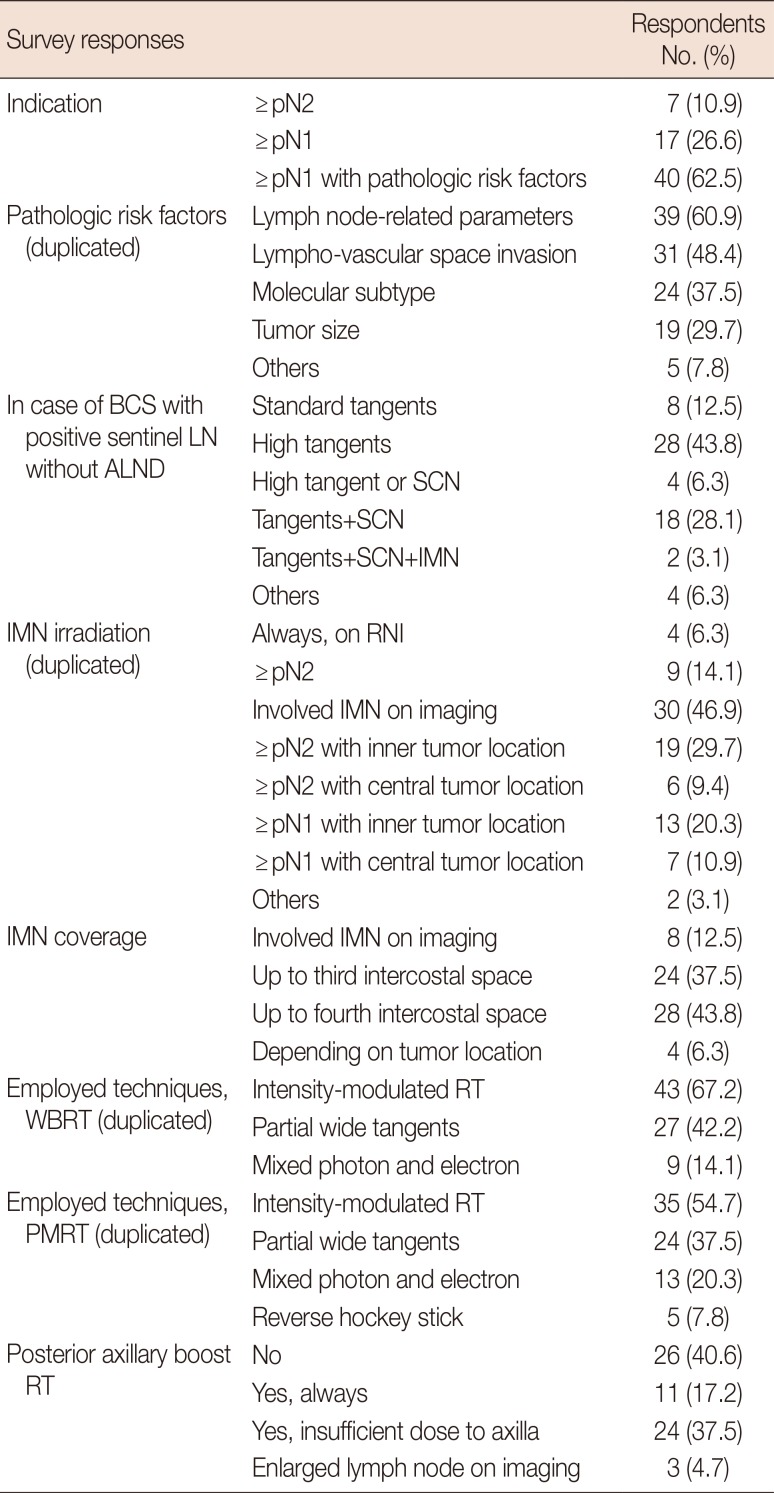
Table 3
Regional nodal irradiation
![]()
Radiotherapy for ductal carcinoma in situ
The majority (87.5%) of radiation oncologists did not consider hypofractionated RT for DCIS treatment. The most common fractionation schedule was 50.4 Gy in 28 fractions (45.3%). Ten respondents (15.6%) had never used boost RT for the tumor bed, but 25 (39.1%) always used boost RT. About half of the respondents (45.3%) considered boost RT depending on clinical and pathological risk factors, including close resection margin (n=28), young age (n=9), and large tumor (n=3).
Thirty-one radiation oncologists (48.4%) considered omission of WBRT after BCS for DCIS. They identified low-risk patients based on risk factors such as age, tumor size, patient's preference, status of estrogen receptor, comorbidities, resection margin, and nuclear grade. Only one respondent considered Van Nuys Prognostic Index (Table 4).
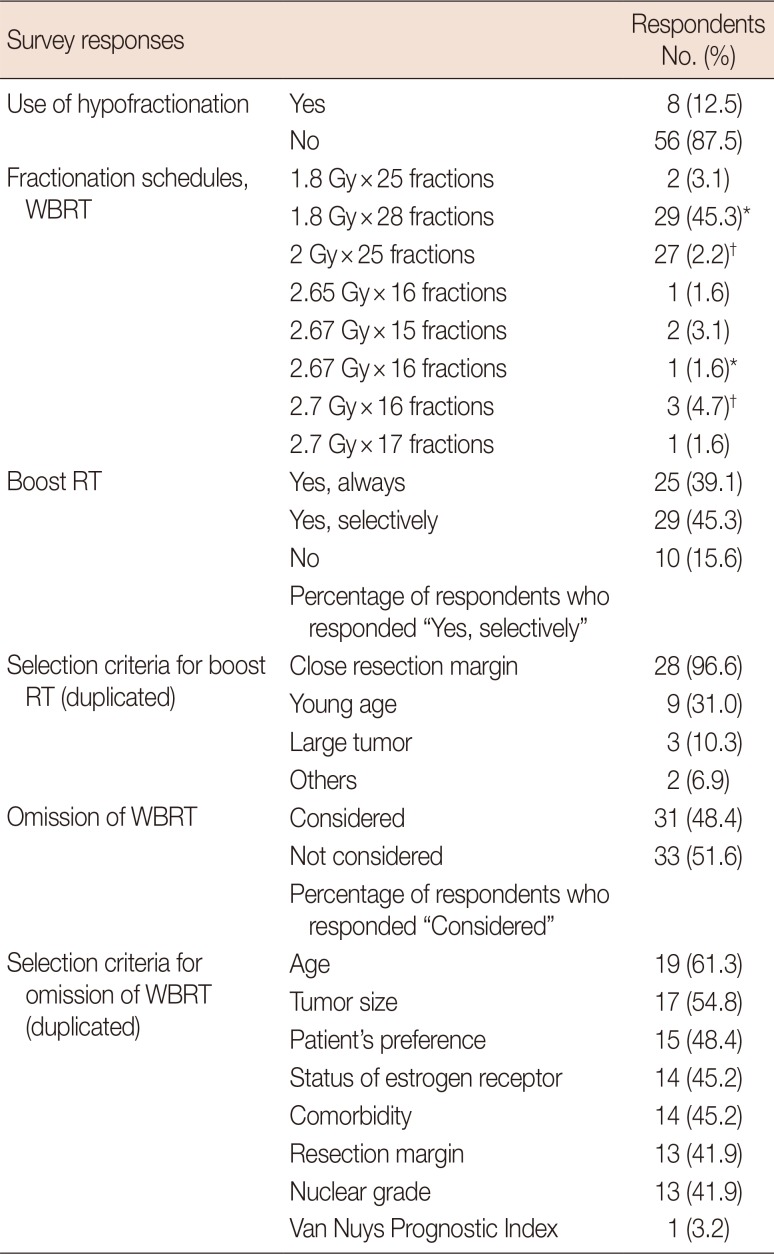
Table 4
RT for ductal carcinoma in situ
![]()
Radiotherapy toxicity
The Radiation Therapy Oncology Group (RTOG) criteria was used to evaluate radiation dermatitis (RD) [12]. For RD prophylaxis, the most commonly used topical agent was EasyDew®/Easyef® (Daewoong Pharmaceutical, Seoul, Korea), which contains a small amount of epidermal growth factor (n=25), followed by gentle soap (n=20), and topical corticosteroids (n=10). Seven respondents did not recommend RD prophylaxis during RT. Regarding RD treatment, the preferred treatment differed according to the severity of RD. Respondents used Silvadene® cream (Pfizer Inc., New York, USA)/dressing and antibiotics more frequently for grades 2–3 RD with moist desquamation than grade 1 RD with dry desquamation. Three respondents stated that they referred patients to a dermatologist for the management of grades 2–3 RD.
To reduce cardiotoxicity, 52 (81.2%) surveyed radiation oncologists employed heart-sparing techniques: intensity-modulated RT (n=33), heart block (n=31), deep inspiration breath hold technique (n=9), and prone position (n=6).
Go to :
DISCUSSION
This is the first nationwide survey for breast RT designed by the Division for Breast Cancer of the KROG and endorsed by the KROG, although a number of similar questionnaire-based surveys have been conducted worldwide.
Delaney et al. [13] pointed out variations in practice would probably always exist and there were many reasons; prior education and training of the radiation oncologist, institutional history, treatment biases of individuals, different philosophies on the way that cancer recurs and spreads, different interpretations of the literature and different resources available. As expected with these reasons, our study revealed marked variations in current practices of breast RT in Korea.
For hypofractionated WBRT for DCIS and PMRT, high-quality data are still scarce. Retrospective studies by Ciervide et al. [14] and Lalani et al. [15] reported similar local recurrences in DCIS patients whether treated with hypofractionation or conventional regimen after BCS. A prospective trial by Koukourakis et al. [16] reported encouraging local control rates in high-risk subgroups and tolerable toxicity with hypofractionated PMRT with amifostine cytoprotection. Another prospective trial by Ali and Abd AlMageed [17] reported equivalent disease control and cosmesis between conventional PMRT (50 Gy in 25 fractions) and hypofractionated PMRT (42 Gy in 16 fractions). This lack of high-level evidence could partially explain the very low use of hypofractionation in RT for DCIS and PMRT.
For hypofractionated WBRT for early-stage breast cancer, on the other hand, two trials provided high-quality evidence; the UK Standardisation of Breast Radiotherapy (START) Trial B compared 50 Gy in 25 fractions to 40 Gy in 15 fractions [18], while a Canadian study compared 50 Gy in 25 fractions to 42.5 Gy in 16 fractions [19]. No significant difference in tumor control and breast cosmesis was reported. Despite the high-quality evidence, one-third (35.9%) of the surveyed radiation oncologists in Korea adopted hypofractionation due to the reasons described in the Results.
Hypofractionated RT has several advantages over conventionally fractionated RT: shorter treatment period, increased patient convenience, and lower costs (both direct health care expenditures and opportunity costs to the patient and society due to time away from home and work) [2021]. However, easily accessible medical facilities and low medical costs for cancer patients because of National Health Insurance along with widespread private insurance in Korea attenuates the necessity of hypofractionated RT. It is noteworthy that one-third (34.4%) of the surveyed radiation oncologists still consider the long-term data of hypofractionated RT insufficient despite evidence-based guidelines [2122].
Regarding RNI, there is a consensus that it should be given to patients with 4 or more axillary LNs involvement (pN2). However, there remains controversy in how patients with 1–3 axillary LNs involvement (pN1) or patients with high-risk node-negative disease should be treated.
Our study demonstrated significant variability in practice patterns regarding not only the indication for RNI but also the extent of RNI. Two-thirds (62.5%) of the surveyed radiation oncologists considered RNI in pN1 and pathologic risk factors. It is possible that results of the National Cancer Institute of Canada (NCIC) MA.20 trial and the Early Breast Cancer Trialists' Collaborative Group (EBCTCG) meta-analysis influenced the current practice of RNI. Both the NCIC MA.20 trial and EBCTCG meta-analysis concluded that the addition of RNI could reduce recurrences and mortality for patients treated with BCS and mastectomy, respectively.
The MA.20 trial randomized patients with pN1 or high-risk pN0 after BCS and adjuvant systemic therapy to undergo either WBRT or WBRT plus RNI (including SCN, IMN, and axilla), and patients were stratified according to the number of axillary LNs removed and involved. The MA.20 trial concluded that the addition of RNI reduced breast cancer recurrences but did not improve overall survival [23]. The EBCTCG meta-analysis analyzed 8,135 patients from 22 trials that randomly assigned patients to treatment groups of either no PMRT or PMRT (including SCN, IMN, and axilla), and showed PMRT reduced both recurrence and breast cancer mortality in pN1 as well as pN2 [24]. However, these two studies with high-level evidence did not influence current Korean practitioners regarding the extent of RNI. Approximately half (46.9%) of the respondents treated IMN only if involved IMN was identified on imaging, and only four (6.3%) routinely treated IMN when RNI was applied.
In the setting of ACOSOG Z0011 [25], which is of an early-stage breast cancer patient with 1–2 positive sentinel LNs undergoing BCS without further axillary dissection, 12.5% and 50.0% of the respondents used standard and high tangents, respectively. These results were consistent with those of an Australian study; 20.4% and 48.9% of practitioners used standard and high tangents, respectively.
Although the literature has demonstrated that RT halves ipsilateral breast tumor recurrence after BCS for DCIS, patients show a favorable survival outcome with a 10-year survival rate >98%, regardless of the intensity of locoregional therapy [2627]. Given the favorable prognosis of DCIS, efforts to identify patients who are suitable for less-intensive treatment have been made [2829].
In a recent survey from the United States (using the Georgia and Los Angeles County Surveillance, Epidemiology, and End Results registries), one quarter of the patients omitted RT after BCS in DCIS, and the most common reason for omitting RT was due to advice from a clinician. A total of 74% of radiation oncologists would discuss RT omission as an option, but 70% would still recommend WBRT in a clinical scenario of a healthy, 65-year-old woman with favorable prognosis DCIS who had undergone BCS [30]. In our study, 48.4% of radiation oncologists considered omission of WBRT after BCS for DCIS in low-risk patients based on clinical and pathologic factors. However, because our questionnaire did not give a specific scenario, it was difficult to compare the results between the two studies.
A number of trials have evaluated the omission of RT after BCS for patients with favorable factors in DCIS. The Eastern Cooperative Oncology Group selected patients with low-risk clinical and pathologic characteristics and observed them without WBRT; the number of invasive ipsilateral breast events increased through 12 years of follow-up, without plateau [28]. The RTOG 9804 trial selected patients with low-risk DCIS and randomized them to either observation or WBRT. The results were promising, contrary to those of the former study, with a 6.7% local failure occurrence at 7 years without WBRT. However, even within this low-risk group, the addition of WBRT reduced the risk of local failure to 0.8%, and longer follow-up data is needed [29].
The aim of the present study was to provide baseline information to physicians about patterns of practice for breast RT in Korea. The results showed a high-degree of variation on issues of breast RT, such as hypofractionation, RNI, and RT omission in DCIS. These issues are also covered by the most recent Korean Clinical Practice Guideline for Breast Cancer, but definite conclusions cannot be reached because additional evidence is needed.
Although the findings of this study are valuable, some aspects of this study require further consideration. A questionnaire-based survey is a very useful method of study to reveal practice variations or controversy on treatments in the medical field. However, the results of the survey are based on self-reported data from respondents and might not reflect actual physicians' practices. Moreover, we could assume that there is a wide range in the number of patients treated by each surveyed radiation oncologists. In other words, the response that 50% of the respondents consider hypofractionation does not mean that 50% of patients are treated with hypofractionation. Population-based studies utilizing data from cancer registries or data on insurance claims are needed to figure out the actual state of practice.
Go to :
 XML Download
XML Download