

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hospitalized patients are at high risk of malnutrition during hospitalization, and malnutrition in these patients are significantly associated with increased morbidity, mortality, hospital stay, and hospital costs [1]. In particular, pediatric patients are highly susceptible to nutritional deficiencies, and the impact of malnutrition can be greater in this population than in adult patients. Poor nutritional status of hospitalized children is directly related to poor short-term disease outcomes. This can also affect long-term outcomes by delaying physical growth and neurocognitive development in these patients [2]. The estimated prevalence of malnutrition among hospitalized children ranges between 12% and 24%, even in developed countries; however, the risk of malnutrition is often under-recognized and overlooked in hospitals [3]. For these reasons, the necessity of a systematic nutritional support for hospitalized children has been emphasized for decades [2].
According to a report from the Council of Europe in 2002, practices related to nutritional care and support of hospitalized patients, such as the use of nutritional risk screening and assessment, the assignment of responsibilities in nutritional support, and educational programs regarding clinical nutrition, were limited and insufficient, even in European countries [4]. South Korea is one of the developed countries in Asia. While medical resources and medical standards are rapidly improving, conditions for nutritional support among hospitalized children seem to be generally insufficient, although this has yet to be evaluated.
Therefore, the aim of the present study was to investigate the nutritional support status of hospitalized children in South Korea by conducting a nationwide hospital-based survey, in order to assist physicians in the recognition of malnourished pediatric patients.
Go to : 
SUBJECTS AND METHODS
Study design and data collection
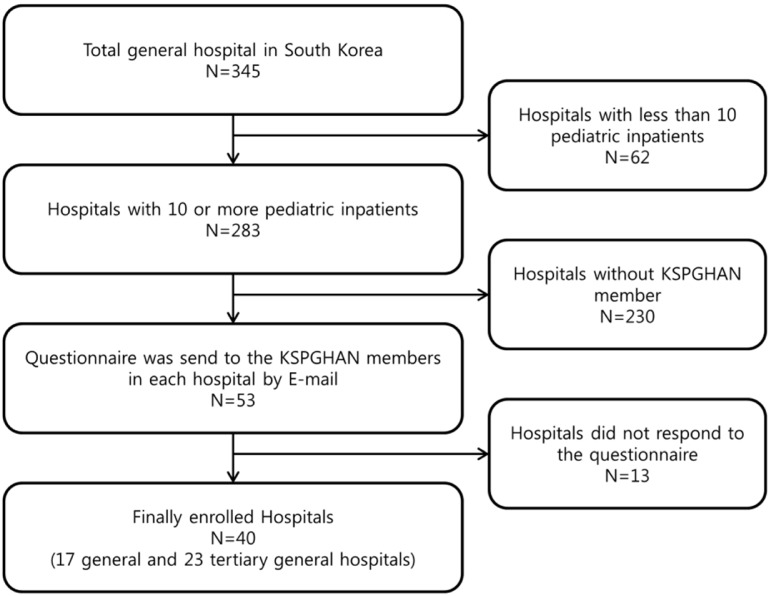
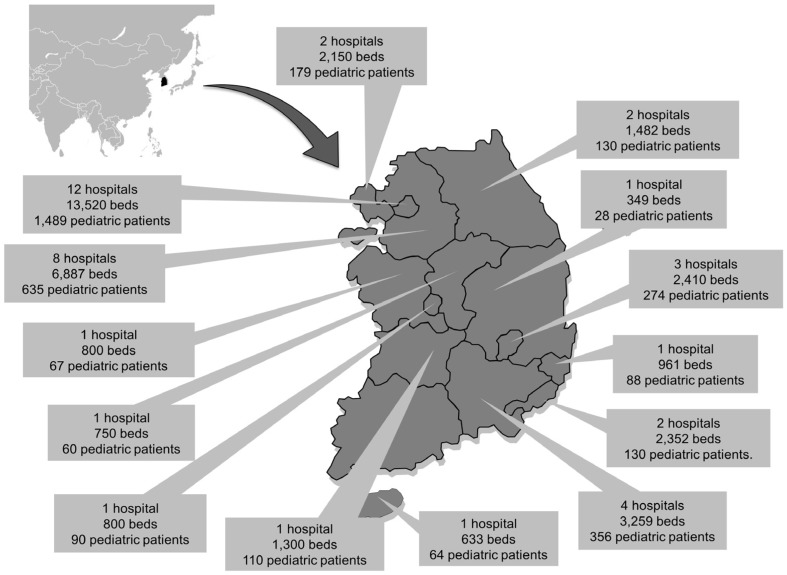
A systematized nationwide hospital-based survey to identify the current status of nutritional support for hospitalized children was officially designed by the Nutrition Committee of the Korean Society of Pediatric Gastroenterology, Hepatology, and Nutrition (KSPGHAN). A general hospital was defined as a hospital with more than 100 beds for inpatients and 7 or more departments, including internal medicine, general surgery, pediatrics, obstetrics and gynecology, radiology, anesthetics, and laboratory medicine. Among general hospitals, a total of 43 hospitals with more than 500 inpatient beds were designated as tertiary hospitals, as qualified by the Ministry of Health and Welfare in South Korea. Of the total 345 general and tertiary hospitals in South Korea, 283 hospitals in which more than 10 pediatric patients were admitted were initially selected. Of these, 53 hospitals in which pediatric gastroenterologists are regular members of KSPGHAN were finally selected to increase the response rate. The questionnaires were emailed to the pediatric gastroenterologist in each hospital. A total of 40 hospitals, including 17 general hospitals and 23 tertiary hospitals, responded to the questionnaire and finally enrolled in the present study (Fig. 1). The overall response rate was 75.5%. Incomplete answers were completed following confirmation by e-mail and direct telephone interviews. These hospitals were distributed nationwide in South Korea, and more than one hospital from each province was included in this study (Fig. 2). Although hospitals were concentrated in the metropolitan area, their distribution was proportional to the number of hospitals and population in each province. This nationwide hospital-based survey was conducted in July 2017. The study was approved by the Institutional Review Board of the Seoul National University Bundang Hospital (IRB no. N-1707-411-601).
Development of questionnaires
The questionnaire was developed and revised by the nutrition committee of KSPGHAN. Through eight times of focused group discussions, questions were developed. After conducting a pilot survey with the questionnaire draft in 10 hospitals, the questionnaire was finalized through direct feedback from 10 committee members. The final questionnaire consisted of 48 items including hospital size (12 items), manpower for nutrition care (4 items), working process of nutrition support (14 items), and hospital resources related to nutritional care (18 items)
Statistical analysis
All statistical analyses were performed using the SPSS software (version 18.0, SPSS Inc., Chicago, IL). Descriptive statistics were used in this study. All data are expressed as median and interquartile range.
Go to :
RESULTS
Basic characteristics of participating hospitals
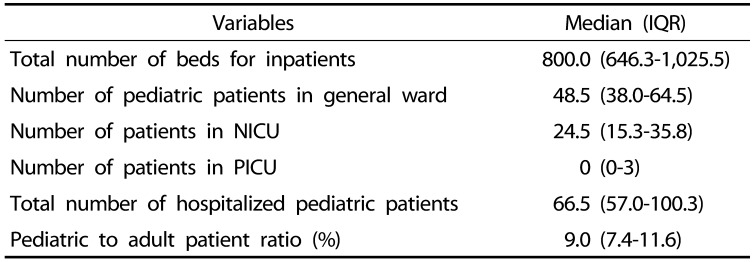
A total of 40 hospitals were finally enrolled in the present study. The size of participating hospitals and the composition of pediatric wards and intensive care units are listed in Table 1.
Composition for nutritional support personnel
Of the 40 hospitals, 37 (92.5%) had physicians who were responsible for nutritional care of pediatric patients. Nutritionists, nurses, and pharmacists who were in charge of clinical nutrition for pediatric patients were available in 30 (75.0%), 26 (65.0%), and 27 (67.5%) hospitals, respectively. However, only 21 (52.5%) hospitals provided a complete team of nutritional support personnel (physician, nutritionist, nurse, and pharmacist) for the nutritional care of pediatric patients (Table 2). In 8 (20.0%) hospitals, nutritionists, nurses, and pharmacists were not assigned for pediatric nutrition, although the median number of pediatric patients was 55 in these hospitals. Nutritionists assigned for pediatric nutrition support were also responsible for adult patients in 21 (52.5%) hospitals. Only 9 (22.5%) hospitals had nutritionists assigned exclusively for pediatric nutritional support, while only 3 (7.5%) hospitals provided nurses and pharmacists exclusively working for children.
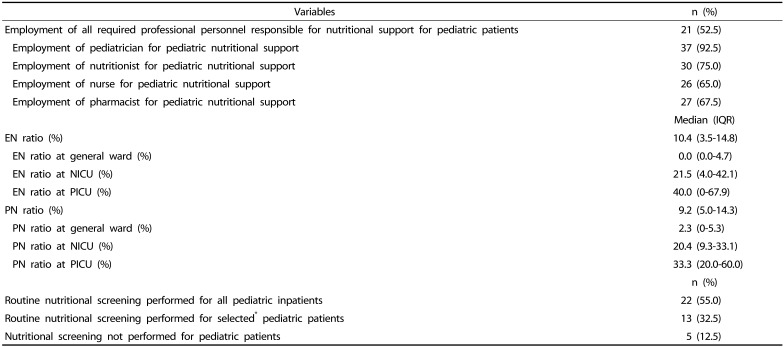
Table 2
Status of nutritional support for pediatric patients in enrolled hospitals (n = 40)
* “Selected” refers to patients classified as high-risk patients with malnutrition according to the policy of each hospital (for example, patients in intensive care unit).
IQR, interquartile range; EN, enteral nutrition; PN, parenteral nutrition; NICU, neonatal intensive care unit; PICU, pediatric intensive care unit.
![]()
Provision of enteral and parenteral formulas for nutritional support in hospital
The proportion of hospitalized pediatric patients who receive enteral nutrition (EN) or parenteral nutrition (PN) was investigated in all participating hospitals on the same day during this nationwide survey. Although the proportion of those receiving EN or PN varied according to the hospitals and ward type, the prescription rates of both EN and PN were the highest in the pediatric intensive care unit and lowest in general wards (Table 2).
The use of nasogastric tube for short-term nutrition support was available in all hospitals. EN with gastrostomy tube was also available in many hospitals for prolonged nutritional support; however, gastrostomy tube feeding was not applied for pediatric patients in 8 (20%) hospitals. The type of EN formula available for nutrition care of pediatric patients did not vary in most hospitals. In 9 (22.5%) hospitals, 2 or 3 EN formulas were used for hospitalized pediatric patients. In 21 (52.5%) hospitals, only 1 formula was used for children. In the remaining 10 (25%) hospitals, EN formulas specifically for children are not supplied at all. On the other hand, between 4 and 25 (median 13) types of EN formulas were available for adult patients in all hospitals; these formulas are initiated according to the medical condition and underlying disease of the patients (Table 3).
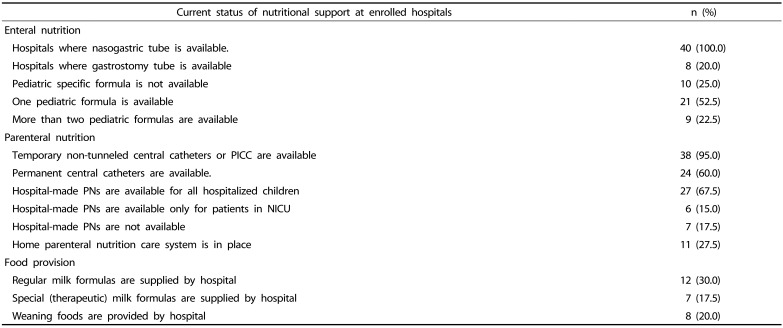
Temporary non-tunneled central catheters such as subclavian catheters and peripherally-inserted center catheters were primarily used for central PN supply in most hospitals. In 16 (40%) hospitals, permanent central catheters such as chemo-ports, Hickman catheters®, and Broviac catheters® were not available for long-term central PN support in pediatric patients. Home PN care for patients with intestinal failure was available in only 11 (27.5%) hospitals. The remaining 29 (62.5%) hospitals did not have any home PN care programs for pediatric patients. In 27 (67.5%) hospitals, hospital-made PNs were available for all hospitalized children. In 6 (15%) hospitals, commercialized PN products were prescribed only to neonatal intensive care unit patients. In the remaining 7 (17.5%) hospitals, individualized hospital-made PN products were not available (Table 3).
Other than EN or PN, the method of providing feeding formula varied between the hospitals. In many hospitals, infant formula was brought from home by the parents. Milk formula and special milk formula were supplied in only 12 (30%) and 7 (17.5%) hospitals, respectively. Weaning food was provided in only 8 (20%) hospitals (Table 3).
Nutritional screening and assessment for hospitalized children
In adult patients, 25/38 (65.8%) of the surveyed hospitals were performing nutritional screening for all hospitalized patients at the time of admission. On the other hand, nutritional screening was performed for every hospitalized children at the time of admission, in 22/40 (55.0%) of hospitals. In 13 (32.5%) hospitals, nutritional screening was performed only for selected high-risk pediatric patients. Even in 5 (12.5%) hospitals, nutritional screening was not performed for pediatric patients (Table 2).
Among 35 hospitals where nutritional screening was performed, screening methods for patients at risk of malnutrition varied from hospital to hospital. One hospital (2.5%) applied the pediatric nutritional risk score, while another hospital (2.5%) used the STRONGkids (screening tool risk on nutritional status and growth) as a nutritional screening tool. Other 33 hospitals (82.5%) used their own methods of nutritional screening.
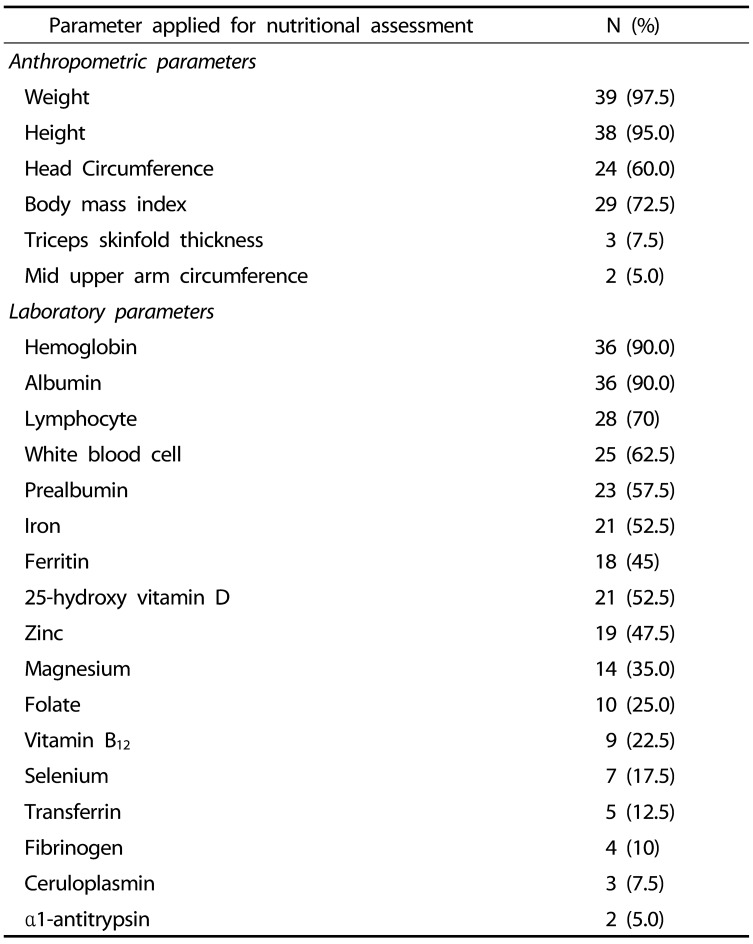
Anthropometric and laboratory parameters frequently used for nutritional assessment of hospitalized pediatric patients are listed in Table 4. Weight, height, and body mass index were most commonly used for anthropometric assessment, while hemoglobin, serum albumin, and lymphocyte levels were most frequently used for laboratory assessment.
In this nationwide hospital-based survey in South Korea, lack of manpower, time, knowledge, and experience, as well as low medical fee for nutritional care and insufficient medical equipment and nutritional formulas, were the main barriers to proper nutritional support for children admitted to hospitals (Table 5).

Go to :
DISCUSSION
Hospitals in South Korea are known for their qualified doctors, fast service, and well-equipped large-scaled facilities [5]. According to data from the Ministry of Health and Welfare in South Korea, 364,189 foreign patients visited South Korea annually for medical services, and the number is increasing by approximately 30% every year. Although hospitals in South Korea are gradually evolving to global standards, nutritional care and attention to clinical nutrition among hospitalized patients is relatively insufficient, and even associated studies are scarce. In the present study, a total of 40 general hospitals were investigated through a nationwide hospital-based survey. The results of our study may represent approximately 12% of the total general hospitals (345 hospitals) in South Korea. This is the first study to investigate the status of nutritional support for hospitalized pediatric patients in South Korea. We aimed to determine the current status of nutritional support for hospitalized children through this nationwide hospital-based survey.
As reported by the ESPGHAN committee on nutrition, experienced physicians, nutritionists, nurses, and pharmacists encompass the ideal members of nutritional support [2]. However, according to our study, only half of general and tertiary hospitals in South Korea met this condition. Even when various medical conditions in each hospital were taken into account, this is still low, considering the size of the hospitals. In 8 hospitals, no personnel was assigned for nutritional care other than physicians. These findings suggest the future direction of the nutritional support system in Korean hospitals. Even if members of nutritional support team are able to care for adult patients, all possible professional health care providers should be assigned to pediatric nutrition, as manpower is the cornerstone of nutritional support. Consultation on nutritional support is available only when human resources and nutritional consultation system are in place and satisfactory clinical outcomes from nutritional support may result in additional consultations. Through this virtuous cycle, experience and knowledge can be accumulated and linked to high-quality nutritional support. In our nationwide hospital-based study, the most frequently encountered barrier to in-hospital nutritional support was the lack of manpower and time. Similarly, Ladas et al. [6] reported that the biggest obstacle to nutritional care was the limited availability of registered dieticians.
EN and PN are essential parts of nutritional support [7]. Since the characteristics of patients differed, the proportion of EN and PN prescriptions varied from hospital to hospital in the present study. In all hospitals, it was possible to use short-term nasogastric tubes for enteral feeding. Although gastrostomy feeding should be used for prolonged enteral feeding [8], gastrostomy tube was not available for pediatric patients in approximately 20% of hospitals. In addition, compared to adult EN formulas, few varieties of EN formulas were available for children. Furthermore, as EN formulas specified for childhood diseases were not available in many hospitals, disease-specified adult EN formulas were inevitably initiated on children.
In terms of PN supply, not every hospital used permanent central catheters. Customized hospital PN preparations for pediatric patients were available in 67.5% of hospitals. Since manufactured PN products are generally made for adult patients, the amount of calories and electrolytes contained is suitable for patients with larger physique. Therefore, for small pediatric patients, personalized hospital-made PN formula for each patient is required for ideal PN support. However, the provision of individualized, hospital-made PN was limited in several hospitals. Although the absolute number of pediatric patients is much less than that of adult patients and the profitability may be much less accordingly, manufacturers should make an effort to produce more variety of products for children. Hospitals should also attempt to provide optimal nutritional formula for each patient. The government may play a role in mediating any potential economic and ethical conflicts.
Experts agree that early interventions ensure the effectiveness of nutritional therapy [9]. Furthermore, according to a nationwide study in Asia, whether or not to perform nutritional screening as a routine has a major impact on nutritional work processes and the methods of nutritional support [10]. That is why guidelines emphasize on routine nutritional screening on admission [11]. In the present study, routine nutritional screening for all hospitalized children was performed in approximately half of the hospitals, which was relatively lower than that in adult patients (55.3% vs. 65.8%). According to a European study, nutritional screening on admission was performed routinely in 21–73% of hospitals [12]. Although these rates were similar to ours, it should be highlighted that this European study was conducted approximately a decade before our survey. Nutritional screening process for pediatric patients should therefore be improved for proper nutritional support during hospitalization in Korea.
Several nutritional screening tools for adult patients are widely used in clinical practice. However, no widely-used nutritional screening tools are available for children, even though this population is vulnerable to malnutrition [13]. While pediatric nutritional risk score, subjective global nutrition assessment, STAMP, PYMS, and STRONGkids have been developed as pediatric nutrition screening tools for children, there are no standardized approaches [14]. According to our study, screening tools also varied between hospitals in Korea. Most hospitals used their own screening methods instead of the above-mentioned tools. In order to provide well-organized nutritional support, guidelines for standardized nutritional screening should be developed for hospitalized Korean children. Furthermore, this should not only be applied to newly-hospitalized patients, but also patients who have been hospitalized for longer periods, who may require screening on a regular basis.
Reluctance to change, lack of knowledge, lack of defined responsibility, lack of defined protocols, and overload of daily work were listed as the main barriers to an effective in-hospital nutritional support, according to the Italian study [15]. Similarly, in our nationwide hospital-based survey, lack of manpower, time, as well as financial and medical resources, were reported as major barriers. These barriers cannot be solved without the multifaceted involvement of the hospitals or government, as manpower and medical resources are mainly concentrated in adult patients rather than in children, who make up a relatively smaller sized population in many countries.
There are several limitations to our study. First, because the questionnaires were sent to pediatric gastroenterologists, who are KSPGHAN members and also already invested in pediatric nutrition, the results of this survey may have overestimated the actual status of nutritional support for pediatric inpatients. Second, since some hospitals did not respond to the survey, our results may not reflect the overall condition of in-hospital nutritional support. Third, although the questionnaire was made through several intensive discussions and pilot surveys, the reliability and validity of the questionnaire could not be analyzed statistically, as the number of relevant subjects and existing data were limited. Additional communications between the enrolled subjects and the nutritional committee was carried out to complement this limitation.
In conclusion, nutritional support systems varied among hospitals and were often inadequate to provide sufficient nutritional care to hospitalized pediatric patients. Educational, financial, and administrative support is required for optimal nutritional management of hospitalized pediatric patients.
Go to :
 XML Download
XML Download