

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endometrial cancer (EC) is the most common gynecologic malignancy in the United States [1]. It most commonly presents in early stage, and adjuvant radiation therapy is often prescribed following surgery. The Post-Operative Radiation Therapy in Endometrial Cancer (PORTEC)-2 trial showed that vaginal brachytherapy (VBT) was non-inferior to traditional external beam radiation therapy (EBRT) in reducing vaginal recurrence in patients with high-intermediate risk early stage EC [2], and was also better tolerated with regard to long-term gastrointestinal (GI) toxicity [3]. Due to its efficacy and favorable toxicity profile, VBT is generally well-accepted by patients and physicians alike [4].
The most common applicator used to deliver VBT is a single-channel vaginal cylinder. These cylinders are available in various sizes, and per the American Brachytherapy Society (ABS) guidelines, for each patient the largest diameter cylinder that can comfortably and snugly fit into the vaginal apex should be selected [5]. This recommendation owes largely to the known dosimetric advantages conferred by larger cylinders. In particular, larger cylinders decrease air gaps and improve contact with the vaginal mucosa, which can reduce potential areas of underdosage [67], and when prescribing dose to 5 mm depth, larger cylinders result in decreased dose to the vaginal surface while increasing dose to deeper structures [8].
Although we always strive to place the largest possible cylinder at our institution, some patients nevertheless require smaller cylinders because of unusually narrow vaginal anatomy. In this study, we examined the outcomes (tolerability, toxicity, and recurrence) among patients treated with smaller cylinder size compared to those who were treated with larger cylinders.
MATERIALS AND METHODS
From a prospective departmental database of 375 patients approved by the institutional review board, we identified 304 patients who received adjuvant iridium-192 high-dose-rate (HDR) VBT without external beam radiotherapy for International Federation of Gynecology and Obstetrics (FIGO) stage I–II EC at our institution between September 2011 and December 2015. Patients who were treated for advanced stage or recurrent disease were excluded.
All patients underwent staging surgery consisting of total hysterectomy, bilateral salpingo-oopherectomy, and pelvic/para-aortic lymph node evaluation as indicated, with or without peritoneal cytology. Patients with early stage disease meeting criteria for adjuvant therapy were referred for radiation oncology evaluation. Based on risk factors including age, stage, depth of myometrial invasion, tumor grade, histology, presence of lymph-vascular space involvement, lower uterine segment location, and tumor size, patients were recommended VBT.
All patients were examined and triaged to start VBT in a manner previously described [9]. At the time of consultation, each patient was fitted with a vaginal cylinder, selected from custom-fabricated diameter sizes of 2.0, 2.3, 2.6, and 3.0 cm. Cylinder size was chosen iteratively, starting from the largest size and adjusting based on examination and patient feedback. Patients were coached using relaxation techniques and reassured that they should feel pressure but no pain, with the goal of selecting the largest possible cylinder. For patients who expressed discomfort or anxiety during vaginal cylinder placement, prescription for oral benzodiazepine (BZD) was written explicitly for the purpose of improving tolerance of the upcoming VBT procedure. BZD was then taken by these patients 30 minutes prior to each fraction of VBT.
VBT was delivered using a HDR 192Ir source (Varian GammaMedplus iX; Varian Medical Systems Inc., Milpitas, CA, USA). Patients were treated with a single-channel vaginal cylinder, matched in diameter to the cylinder they were sized with at the time of consultation. Most patients were prescribed a dose of 21 Gy in 3 fractions every 1–2 weeks when using 3.0 cm cylinders, but a lower dose of 18 Gy in 3 fractions was used for patients with smaller cylinders in order to achieve a similar surface dose of 10–10.5 Gy [10]. For certain patients with serous or clear cell histology receiving chemotherapy, the dose was adjusted to 14 Gy in 2 fractions [11]. Treatment was prescribed to a 5-mm depth from the cylinder surface. The active treatment length (i.e., distance from most proximal to most distal activated dwell positions in the cylinder's central canal) was chosen based on the patient's post-hysterectomy vaginal length and recurrence risk, as previously reported [10]. Active treatment length was tailored to 3-4 cm for the lowest risk patients, 4–5 cm for the intermediate-risk patients (>50% myometrial invasion or stage II or higher disease), and 5–6 cm for the highest risk patients (grade 3, or serous/clear cell histologies). All patients were treated from a library of template plans, with each source dwell position separated by 1 cm. Additional optimization was not done. Planning was performed in Eclipse version 13.6 (Varian Medical Systems Inc.). All plans were 2-dimensional and dose calculations used a water phantom. Three-dimensional imaging was not performed and dose to normal tissues was not calculated. All patients were instructed to use vaginal dilators, beginning 2 weeks post-treatment, for >1 year duration for the prevention of vaginal stenosis.
Patient, tumor, and treatment characteristics were recorded in the database and included age, body mass index (BMI), race, gravidity, sexual activity, FIGO stage, tumor grade, histology, receipt of chemotherapy, cylinder size, post-hysterectomy vaginal length, proportion of vagina treated, number of fractions, and dilator use. Post-hysterectomy vaginal length was measured systematically for each patient using a custom rigid cylinder. Small cylinder size was defined as size 2.0 or 2.3 cm. Measures of treatment tolerability and toxicity were also recorded and included discontinuation of VBT, need for BZDs, on-treatment GI, genitourinary (GU), or vaginal symptoms; late vaginal stenosis was evaluated at each radiation oncology follow-up visit, graded by the Common Terminology Criteria for Adverse Events (CTCAE) v4.0 (National Cancer Institute, Rockville, MA, USA). Disease recurrence was recorded from radiation oncology as well as gynecologic oncology notes in the hospital electronic medical record. Chi-square tests (for categorical variables) and the Wilcoxon rank sum test (for continuous variables) were used to evaluate if any patient, tumor, or treatment characteristics were associated with need for small cylinders. We also used χ2 tests to examine if any factors, including cylinder size, correlated with treatment discontinuation, need for BZDs, or any early and late toxicities. Of note, fraction size was not included in these analyses given that this was determined by cylinder size. A multivariate analysis for factors associated with vaginal stenosis was performed with logistic regression. Two-sided p-values were considered significant if p<0.05. Statistical analyses were performed using STATA (version 13.0; StataCorp, College Station, TX, USA).
RESULTS
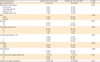
Patient, tumor, and treatment characteristics are shown in Table 1. Of 304 patients with early stage EC, the median age was 65 years (range, 43 to 94). The majority were Caucasian (84%) and overweight/obese (82%). Most had stage IA cancer (72%), with the remainder being stage IB (23%) and stage II (5%). Fifty-five (18%) were nulligravid, 81 (27%) had type II histology, and 100 (33%) received chemotherapy. Cylinder size was 3.0 cm in 157 (52%), 2.6 cm in 96 (31%), 2.3 cm in 49 (16%), and 2.0 cm in 2 patients (1%). In total, 51 patients (17%) required small cylinder sizes (2.0 or 2.3 cm). The median post-hysterectomy vaginal length was 8 cm (range, 5–12).
Table 1
Baseline patient and treatment characteristics

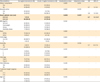
On univariate analysis, normal weight (BMI <25; p<0.001), nulligravidity (p<0.001), and shorter post-hysterectomy vaginal length (p<0.001) were associated with placement of small cylinders (Table 2). Other characteristics were similar when comparing small cylinder patients to larger cylinder patients.
Table 2
Baseline patient characteristics by cylinder size
Overall, treatment was very well tolerated. All but 6 patients (98%) completed treatment as prescribed. Two patients were hospitalized during their brachytherapy course for reasons unrelated to treatment, and subsequently were unable to complete VBT. Four patients chose to discontinue treatment early because of poor tolerance, for reasons including back pain (1 patient), concern over side effects (1 patient), and other (2 patients). Rates of discontinuation were not different between small and larger cylinder cohorts (p=0.27). Eighteen patients in total (6%) required prescription BZDs. On univariate analysis, small cylinder size (p<0.001; odds ratio [OR]=5.81 [2.18–15.5]) and nulligravidity (p=0.003; OR=3.97 [1.49–10.6]) were associated with need for prescription BZDs.
In terms of side effects, acute GI side effects were reported by 31 patients in total (10%). Symptoms noted included grade 1–2 diarrhea, abdominal cramping, bloating, and nausea. On univariate analysis, only small cylinder size was significantly associated with acute GI symptoms (p=0.018; OR=2.69 [1.18–6.14]). By first follow-up at 3 months these symptoms had resolved in 24/27 (89%) of patients (4 patients did not have follow-up).
Acute GU side effects were reported in 34 patients (11%). Symptoms noted included grade 1–2 urinary incontinence, frequency, urgency, pressure, pelvic spasms, nocturia, and urinary tract infection. Small cylinder size was not associated with increased acute GU symptoms on univariate analysis (p=0.270).
Acute vaginal symptoms were reported in 59 patients (19%), which included grade 1–2 vaginal irritation, dryness, discharge, soreness, swelling, and fungal infection. There were no variables associated with increased likelihood of acute vaginal side effects, including small cylinder size (p=0.730).
Analysis of post-treatment vaginal stenosis was performed in 144 patients out of the total 304 (47%) who had at least 2 consecutive follow-up visits in a radiation oncology clinic. Among these patients, the median radiation oncology follow-up time was 17.7 months (range, 7.6–38.6 months). Twenty-eight percent were sexually active, and 69% were compliant with vaginal dilator use as instructed for the prevention of vaginal stenosis. On univariate analysis, factors associated with increased risk for vaginal stenosis included nullgravid status and small cylinder size; factors associated with reduced likelihood of stenosis included being sexually active and/or compliant with vaginal dilators (Table 3). On multivariate analysis, small cylinder size remained an independent risk factor for grade 1 or higher vaginal stenosis (Table 3).
Table 3
Association of treatment characteristics including small cylinder size with vaginal stenosis: univariate and multivariate analyses
Recurrences occurred in 21 patients (7%); 2 of these recurrences were vaginal only (both distal vagina/sub-urethral location), both in patients treated using larger cylinders. Overall, there was no difference in recurrence rate with regard to cylinder size (p=0.55).
DISCUSSION
While most patients in our study were fitted with standard cylinder sizes ≥2.6 cm, a small but significant proportion (17%) required smaller cylinders of 2.3 or 2.0 cm in diameter. Factors that were associated with small cylinder placement included lower BMI, nulligravidity, and shorter post-hysterectomy vaginal length. As expected, treatment was generally well-tolerated by the entire cohort, with acute and low grade GI, GU, and vaginal symptoms in just 10%, 11%, and 19%, respectively. Nonetheless, our data suggest there may be an association between the need for small cylinder size and slightly poorer VBT tolerance, as measured by an increased need for BZDs and an increased rate of acute (but transient) GI symptoms. Furthermore, there was a significant increased risk of post-treatment vaginal stenosis among those who were treated with smaller cylinders, even after accounting for sexual activity and dilator compliance. Reassuringly, recurrence rates were very low, and not different from those treated with larger cylinder size.
Little data exist in the literature regarding the prevalence of smaller cylinder sizes among EC patients receiving adjuvant VBT. A few prior studies indicated a relatively low rate of use of cylinder sizes ≤2.5 cm, ranging from 4% to 8% of patients [1213], while other studies reported range of cylinder sizes used but not the actual distribution of sizes [141516]. A recently published modern series noted a significantly increased proportion of patients requiring smaller cylinders, with 194/381 (51%) fitted with cylinder sizes ≤2.5 cm; however, about a third of the patients in this study also received EBRT, and the main finding was that the addition of EBRT, low BMI, and low weight was associated with need for smaller cylinders [17]. Although prior studies have noted dosimetric disadvantages associated with smaller cylinder size [818], there are no prior studies to our knowledge which have examined the demographics and clinical outcomes of patients treated with small cylinders.
This study highlights that this population may have a slightly increased risk of treatment associated acute GI side effects and late vaginal toxicity. There is prior literature supporting a correlation between lower BMI and higher bowel dose [19]. Conversely, prior studies have correlated larger cylinder size with larger rectal and bowel D2cc dose [20]. Therefore, whether the increased GI symptoms in this group are attributed to a dosimetric versus other explanation might warrant further study, with 3-dimensional dose information available. Vaginal stenosis is a well-described sub-acute to late effect following vaginal or pelvic radiation. The higher risk found in patients treated with small cylinders in this study may reflect the higher surface dose related to the geometry of the smaller cylinder [8]. There may also, however, be baseline differences in tissue quality and vaginal atrophy in this group which were not measured. For this population, it may be worthwhile to consider a more fractionated regimen which decreases late effects [21], preventative treatments to reduce the likelihood of this late effect [22], or novel applicators which may improve the comfort of cylinder placement while allowing for improved geometry.
Our finding that narrow vaginal diameter was associated with an increased need for prescription BZDs (18% vs. 4%) may agree with a qualitative study reported by Kamer et al. [23], which found that women who were unmarried or had low parity were more likely to feel anxious during intra-cavitary brachytherapy than someone who had borne several children. Indeed, our data showed an association both between nulligravidity and need for small cylinders, as well as nulligravidity and need for prescription BZDs. As reported among prior retrospective series, there is a wide range in how providers historically employed anxiolytics and sedation during administration of VBT, with some using these medications in many if not all patients [1324], while others rarely offered them [1416]. Nevertheless, studies have shown that these types of medications do improve the patient experience [25]. Simple non-pharmacologic interventions could also improve patient experience, including dedicated nursing care, warm blankets, comfortable leg positioning, careful music selection, privacy screens, emotional support, limiting number of personnel in the brachytherapy suite, clearly explaining everyone's role, and promptness as well as cognizance of time with applicator between legs [2627].
We recognize some of the limitations of our study. Due to its retrospective nature, importantly, cause and effect cannot be established from this data. We did not examine if there were other issues that could have contributed to a patient's treatment tolerance, such as an underlying psychological disorder, back pain, or history of irritable bowel syndrome (IBS). In particular, a history of sexual abuse or trauma could contribute significantly to tolerance of VBT but is often underreported and can be difficult to assess. In addition, our analysis of post-treatment vaginal stenosis was limited by the short follow-up available for many patients; just over half of the patients in this study had only one early follow-up (n=99) or no follow-up visits (n=61). Patients with only one follow-up (<6 months from treatment) were excluded so as not to dilute the late incidence of vaginal stenosis, which increases over time, and may not manifest until 7–9 months post-treatment [1228]. Maturation of the database would allow inclusion of more patients, as follow-up time increases. Both a larger patient population as well as longer follow-up time would be important to validate our findings, particularly regarding the association between smaller cylinder size and vaginal stenosis. Finally, these findings represent a single institutional experience and may reflect the experience only of a certain geographic population. Thus, multi-institutional validation would be worthwhile.
In conclusion, in this study we show that patients with narrow vaginal anatomy requiring small diameter vaginal cylinders make up a small but significant part of our patient population. Low BMI, nulligravidity, and shorter post-hysterectomy vaginal length were associated with the need for small cylinders. Our patient cohort overall tolerated treatment very well; however, our data suggest there may be an association between need for small cylinders and both need for BZD prescription as well as acute on-treatment GI symptoms. Additionally, this population has a higher rate of post-treatment vaginal stenosis, even after accounting for sexual activity and dilator use. Considerations to potentially improve experience and outcomes in this unique population might include incorporating lower dose-per-fraction VBT regimens to reduce late effects, increasing supportive/preventative on-treatment interventions, and consideration of novel applicator design.
 XML Download
XML Download