

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
There is no standard protocol for the assessment of lymph node (LN) involvement in endometrial cancer (EC) [1] although the 2009 International Federation of Obstetricians and Gynecologists (FIGO) staging system is based on the surgical findings including pelvic and para-aortic LN metastases [2]. Performing lymphadenectomy only for patients at high-risk of extra-uterine disease with the aim of preventing over- and under-treatment is an important issue in the surgical management of EC [3].
Mayo Clinic (Rochester, MN, USA) initiated a paradigm for surgical management of EC in 2004. According to this paradigm (widely known as “Mayo algorithm”), lymphadenectomy has been reported to be no longer deemed necessary for the subset of EC patients with low-risk features [3]. These low-risk features have been defined as; “endometrioid type EC, FIGO grade 1 or 2 histology, myometrial invasion (MMI) ≤50%, and primary tumor diameter (PTD) ≤2 cm” [3]. By contrast, all other patients have been defined as high-risk and introduced as candidates for systematic lymphadenectomy up to the renal veins [4].
Although the rate of LN involvement is approximately 15% in endometrioid EC [5], 75% of women with EC require systematic LN dissection (LND) when the Mayo criteria are used [3]. Lefringhouse et al. [6] have recently reported that the Mayo algorithm performed well at identifying EC at high-risk of extra-uterine disease; however, by recommending lymphadenectomy for over two-thirds of their study population. Given that most ECs are categorized as high-risk by the Mayo criteria, Vargas et al. [7] suggested that low-risk group be expanded to include; 1) grade 1 endometrioid tumors with <50% MMI regardless of PTD, 2) grade 2 tumors with tumor size <3 cm, and 3) grade 3 tumors with no MMI. The Mayo criteria modified by Vargas et al. [7] have been reported to have a positive LN rate of 2.3%, 2%, and 0% for grade 1, 2, and 3 tumors, respectively [7].
According to the European Society for Medical Oncology (ESMO) guidelines, the features of low-risk EC have been defined as endometrioid histology, MMI ≤50% and FIGO grade 1 or 2 [8]. The ESMO criteria were modified by Bendifallah et al. [9] who integrated lymphovascular space invasion (LVSI) into the model (ESMO-modified classification) in 2014. Keys et al. [10] have assigned EC patients into risk categories in order to determine the need for adjuvant treatment according to the age of the patients, histologic type, tumor grade, presence of LVSI, and depth of MMI (the Gynecologic Oncology Group-99 [GOG-99] criteria). Although the GOG-99 and ESMO-modified criteria have been introduced to determine the need for adjuvant treatment in EC, we wondered whether these criteria can be used to predict LN metastasis. Given the high rate of patients undergoing LND according to the current Mayo criteria, there seems to be a need for an alternative model that can more accurately identify the patients who do not require lymphadenectomy.
Therefore, we designed this retrospective, dual-institutional study in order to compare the clinical validity of the GOG-99, the Mayo-modified, and the ESMO-modified criteria for predicting LN involvement in women with endometrioid EC clinically confined to the uterus.
MATERIALS AND METHODS
1. Study design and eligibility
Medical records of consecutive women who underwent primary surgical treatment for EC between January 2010 and December 2016 at 2 gynecologic oncology centers in Ankara, Turkey were retrospectively reviewed. The study protocol was approved by the Local Institutional Review Boards. All patients provided an informed consent regarding research use of their medical information.
The study population included women with endometrioid type EC clinically confined to the uterus who underwent comprehensive surgical staging according to the current Mayo criteria depending on intraoperative frozen section analysis. Women with non-endometrioid type EC, those with macroscopic extra uterine tumor (defined as any disease that was evident on visual inspection of the pelvic and abdominal cavity), patients with gross cervical involvement and those with incomplete medical records were excluded from the study. We also excluded patients with less than 15 LNs in the final pathology report as well as those with synchronous malignancies.
2. Clinical information
Patient data were extracted from 2 institutions with maintained EC databases. With the eligible cases, demographic characteristics were abstracted from medical records.
Tumor characteristics were abstracted from original pathology reports, and the following data were recorded: PTD (as a continuous variable or dichotomous [<2 cm or ≥2 cm] and [<3 cm or ≥3 cm]), depth of MMI ([<50% or ≥50%] and [≤66% or >66%]), presence of LVSI, and the status of peritoneal cytology examination (negative, positive, or not performed).
Surgical staging consisted of total hysterectomy, bilateral salpingo-oopherectomy (based on the age of the patient), pelvic and para-aortic lymphadenectomy, and peritoneal washings. All operations were performed by gynecologic oncologists. Data on the extent of surgery included number of total LNs harvested, number of pelvic LNs removed, and number of para-aortic LNs removed.
All surgical specimens were examined and interpreted by gynecologic pathologists. Architectural grading was defined by standard FIGO criteria. Tumor size was macroscopically measured on fresh tissue by gynecologic pathologists who noted size in 3 largest dimensions. The largest of 3 dimensions of the tumor was defined as PTD [3]. LVSI was defined as the presence of adenocarcinoma of any extent, in endothelium lined channels of uterine specimens extracted at the time of surgery [10]. All tumors were staged according to the FIGO staging system [2].
3. Definitions
Lymphadenectomy was defined as the performance of pelvic and para-aortic LND at the same time. We defined pelvic lymphadenectomy as removal of the lymphatic tissue in the external, internal and common iliac and obturator regions. Para-aortic lymphadenectomy was defined as removal of the lymphatic tissue over the inferior vena cava and aorta beginning at the level of aortic bifurcation up to the left renal vessels. A systematic LND was arbitrarily defined as removal of more than 20 nodes [11]. An adequate pelvic lymphadenectomy was defined as the removal of at least 10 pelvic LNs, and an adequate para-aortic lymphadenectomy was defined as the removal of at least 5 para-aortic LNs [312].
All included patients were divided into low- and high-risk groups according to the GOG-99 [10], the Mayo-modified [7], and the ESMO-modified [9] criteria (Table 1). LVSI is the cornerstone of risk stratification according to the ESMO-modified criteria. Regardless of MMI, the ESMO-modified criteria define all FIGO grade 1 or 2 endometrioid type tumors as high-risk if LVSI is positive. These 3 risk stratification models were compared in terms of predicting LN positivity based on the final pathology reports of the patients.
Table 1
Description of the risk-stratification models

4. Statistical analysis
Statistical analyses were performed using Statistics Package for the Social Sciences (SPSS) software (version 17; SPSS Inc., Chicago, IL, USA). The distribution of the data was analyzed using normality tests. When the data were not normally distributed, the Mann-Whitney U test was used for the comparison of 2 groups. The χ2 and Fisher exact test were used for the comparison of categorical variables. The predictive accuracy of each risk-stratification model was assessed according to its discrimination (i.e., ability of the model to differentiate patients with LN metastases from those without). Discrimination was measured using the receiver operating characteristics (ROC) curve and summarized by the area under the curve (AUC). The AUC requires binary outcomes (presence or absence of the event). The AUC of 0.5 represents no discriminating ability, and a value of 1.0 represents perfect accuracy [9]. The diagnostic performance of 3 risk scoring systems was expressed as sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and positive likelihood ratio (LR+) and negative likelihood ratio (LR−), and was stratified according to the level of diagnostic confidence and reported according to the Standards for Reporting of Diagnostic Accuracy [13]. A p-value <0.05 was considered to indicate statistical significance.
RESULTS
Six hundred and twenty-five women of surgically-staged endometrioid type EC were identified according to the inclusion criteria. The median age of patients was 58 (range, 27–87) and the median tumor diameter was 3.5 cm (range, 0.1–9.5). While 14 (2.2%) patients had a tumor limited to the endometrium, 394 (63%) had <50% MMI and 217 (34.8%) had ≥50% MMI. However, there were 134 (21.4%) women with MMI >66%. Three hundred fifty-three patients (56.5%) had grade 1 tumor, 184 (29.4%) had grade 2 tumor and 88 (14.1%) had grade 3 tumor. Presence of LVSI was identified in 162 (25.9%) patients. Table 2 demonstrates the LVSI status of the patients based on the stage of the disease. Positive peritoneal cytology was present in 27 (4.3%) patients. LN involvement was detected in 70 (11.2%) patients with a systematic LND rate of 100%. The comparison of women with and without LN involvement is presented in Table 3.
Table 2
The LVSI status of the patients based on the stage of the disease
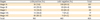
Table 3
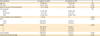
The comparison of women with and without LN involvement with endometrioid EC clinically confined to the uterus
According to the GOG-99 criteria [10], 451 (72.2%) women were classified as low-risk whereas 174 (27.8%) were categorized as high-risk. LN involvement was correctly estimated in 51 of 70 LN-positive patients according to the GOG-99 criteria (sensitivity 72.9%, specificity 77.8%, NPV 95.8%, and PPV 29.3%). When women were classified as low-risk (n=361) and high-risk (n=264) according to the ESMO-modified criteria [9], 64 of 70 LN-positive patients were found to be in the high-risk group (sensitivity 91.4%, specificity 63.9%, NPV 98.3%, and PPV 24.2%). The Mayo-modified criteria [7] identified 303 (48.5%) women as low-risk and 322 (51.5%) women as high-risk. Sixty-nine of the 70 LN-positive patients were found to be classified in the high-risk group when the Mayo-modified criteria were used (sensitivity 98.6%, specificity 54.4%, NPV 99.7%, and PPV 21.4%). The only node positive patient not detected by the Mayo-modified criteria had FIGO grade 2 tumor with MMI <50% and a PTD of 2.5 cm. However, this patient had LVSI. The comparison of the Mayo-modified, GOG-99 and the ESMO-modified criteria in terms of detecting LN involvement is shown in Table 4.
Table 4
The comparison of the Mayo-modified, the ESMO-modified, and the GOG-99 criteria in terms of predicting LN involvement in endometrioid EC clinically confined to the uterus

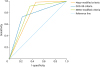
When the ROC analysis of the GOG-99, the Mayo-modified, and the ESMO-modified criteria was performed in order to predict LN metastasis, the AUC was 0.753, 0.763, and 0.780, respectively (p<0.001, Fig. 1).
DISCUSSION
To the best of our knowledge, this is the first study comparing the GOG-99, the Mayo-modified, and the ESMO-modified criteria in terms of predicting LN involvement in endometrioid EC clinically confined to the uterus. We found out that LN involvement in women with endometrioid EC clinically confined to the uterus was most accurately predicted by the ESMO-modified criteria based on the ROC analysis.
However, we should underline some limitations of the current study. First, the retrospective nature of the study cannot exclude any bias. Second, lack of central pathology review seems to be an important limitation. Third, lack of ultrastaging might have been an important issue for underestimating the rate of nodal metastasis in low-risk patients since the rate of nodal involvement increases in this subgroup of patients when ultrastaging is used. Finally, the nature of dual-instutional experience may be interpreted as a limitation.
The most controversial management issue relates to the requirement for, and the extent and therapeutic value of, lymphadenectomy [14]. In order to minimize under-treatment and achieve optimal oncologic outcomes, patients who will derive potential therapeutic value from lymphadenectomy should be identified. On the contrary, patients who will not benefit from lymphadenectomy must be identified in order to minimize over-treatment and prevent lymphadenectomy-associated serious morbidities such as intraoperative bleeding, deep vein thrombosis, lymphocyst formation, lymphedema of lower extremities, and chylous ascites [15]. Since over-treatment is an important issue in the surgical management of endometrioid EC currently [5], a precise balance must be obtained between the desire to prevent over-treatment and the ability to diagnose LN involvement.
However, most of the patients with endometrioid EC fall into the high-risk category and undergo systematic LND when the universally accepted Mayo-criteria are used. Although the Mayo algorithm has been reported to identify a 98.2% NPV for women who would not benefit from a lymphadenectomy [16] and correctly estimates patients who are at low-risk for LN metastasis, Vargas et al. [7] reported that only 21% of patients were classified as low-risk when the Mayo criteria were used. Lefringhouse et al. [6] have recently reported that the low-risk group should be expanded to achieve a better clinical balance of surgical risk and treatment outcomes as two-thirds of early ECs are classified as high-risk by the current Mayo algorithm. The distinctive feature of the Mayo criteria is that it strictly takes PTD into account. For example, a woman with FIGO grade 1 endometrioid EC having ≤50% MMI needs to undergo systematic lymphadenectomy if her PTD is 2.5 cm. Systematic lymphadenectomy becomes indicated at the expense of potential serious morbidities for such a clinical scenario in which PTD exceeds 2 cm, and presents as the sole low-risk feature missing.
However, the ESMO-modified criteria do not take PTD into account while classifying patients into low-risk and high-risk groups. Instead, it integrates LVSI into the model. Currently, LVSI is considered a prerequisite for tumor dissemination to the lymphatic system [17].
There seems to be a correlation between LVSI positivity and depth of MMI. Alexander-Sefre et al. [18] found an association between stage and LVSI incidence: LVSI as detected by hematoxylin and eosin staining was not detected in any patients with stage IA disease but found in 12% and 50% of patients with stages IB and IC disease, respectively. Additionally, dos Reis et al. [17] found that patients with LVSI were more likely to have MMI. A combination of deep MMI and LVSI proved to be superior to LVSI alone in the prediction of pelvic LN metastasis [19].
However, Guntupalli et al. [20] analyzed 757 patients with endometrioid EC stages IA to IVB, and found that LVSI was highly predictive of nodal disease. The authors reported that the absence of LVSI had a NPV of 95% and could therefore be considered as a marker to stratify patients according to the risk of nodal disease [20]. Moreover, the incidence of occult LN metastasis was reported to be 3.6% in a cohort of 438 women with EC and the NPV of LVSI for LN metastasis was found to be 96.4% [21].
Unfortunately, there is currently no surrogate marker of LVSI in a pre- or intra-operative setting. LVSI status is most commonly not available until after hysterectomy, at the time of preparation of the final pathology report. LVSI is very difficult to assess during intraoperative frozen section analysis, and it is often reported only at the final pathology report [20]. Assessment of LVSI is subject to inter-observer variation. Stromal retraction, displacement of tumor cells into vascular channels and coexistent inflammation may all add to difficulty in interpretation [22]. However, it has recently been reported that LVSI may be determined by intraoperative frozen section analysis with 50% sensitivity, 100% specificity, 94.4% of NPV, and 100% of PPV [23]. Based on these data, LVSI may be suggested as a routine pathological parameter to be studied during frozen-section analysis for women undergoing surgery for endometrioid EC in order to decrease the number of patients unnecessarily undergoing LND.
On the other hand, absence of LVSI can be used as a reliable tool for determining patients who do not require para-aortic LND. Kumar et al. [24] reported that surgeons might potentially forgo para-aortic LND in the majority of patients with endometrioid type EC in order to reduce surgical morbidity. The authors emphasized that this cohort can be identified by a combined absence of positive pelvic LNs, >50% MMI, and LVSI [24]. Vaizoglu et al. [25] demonstrated that LVSI should be considered as a valuable pathological parameter for the surgical management of patients with EC. They reported that the incidence of LN metastasis in the para-aortic area was 0.5% among patients without LVSI. A recent study by Sari et al. [26] demonstrated that the rate of para-aortic LN metastasis in patients without LVSI was only 0.8% in a cohort of 641 EC patients that underwent comprehensive surgical staging. In the light of these previous studies and the current one, we think that the combination of absence of LVSI and deep MMI (when safely shown during intraoperative frozen section analysis) may be a reliable tool for determining patients for whom systematic lymphadenectomy can be omitted. We suggest that for prediction LN involvement in endometrioid EC clinically confined to the uterus, one should focus on the trio of tumor grade, depth of MMI and LVSI instead of taking PTD strictly into account.
There are a considerable number of risk scoring systems defined in the literature for predicting recurrence, selecting patients for lymphadenectomy, and identifying indications for adjuvant therapy [378910]. However, the number of studies comparing these risks scoring systems is very limited. Bendifallah et al. [27] have compared Postoperative Radiation Therapy in Endometrial Carcinoma-1 (PORTEC-1) [28], GOG-99 [10], Survival Effect of Para-Aortic Lymphadenectomy (SEPAL) [29], ESMO [8], and ESMO-modified [7] criteria and found out that the ESMO-modified classification is the system that most accurately predicts recurrence risk or LN metastasis. A recent study conducted by Tuomi et al. [30] comparing the Mayo, Helsinki and Milwaukee models for predicting lymphatic dissemination in EC has shown that all 3 models had similar accuracy for detecting LN positivity. In parallel with the results of Bendifallah et al. [27], the present study has also found out that the ESMO-modified classification is the risk-stratification model that most accurately predicts LN involvement in endometrioid EC clinically confined to the uterus.
In the present study, stage IA cases with tumor size >2 cm and grade 1 tumor were included in the low-risk group. Two hundred and sixty-six (46% of our study population) women were found to have the above-mentioned criteria and none of these women had LN involvement. The rate of LN involvement has been reported to be 1.46% (28/1,914) in this subgroup of patients in a Surveillance, Epidemiology, and End Results (SEER) data analysis [31]. In our previous study, LN involvement was not detected in any of the patients (n=120) with stage IA endometrioid type EC having FIGO grade 1 tumor and a PTD >2 cm [32]. Vargas et al. [7] reported the same figure as 1.62% in another SEER data analysis including 3,816 patients. Our finding of 0% rate of LN involvement in this subgroup of patients in the current study may be attributed to the limited number of patients (n=266) compared with those of Mahdi et al. [31] and Vargas et al. [7]. Vargas et al. [7] reported that LN involvement remained below 2% until PTD exceeded 4 cm in this subgroup of patients. Even in tumors greater than 5 cm in size, the rate LN involvement remained below 3%. Given these findings, the authors have concluded that it may be reasonable to defer LND in all grade 1 tumors with less than 50% MMI, irrespective of tumor size [7].
The strengths of the current study lie in the large number of patients with similar demographic characteristics, performance of uniform staging procedures with the same qualified gynecologic oncologists, and a 100% rate of systematic LND. Our study is one of the largest retrospective cohorts associated with the prediction of LN metastasis in women with endometrioid EC clinically confined to the uterus.
In conclusion, the ESMO-modified classification seems to be the risk-stratification model that most accurately predicts LN involvement in endometrioid EC clinically confined to the uterus. When compared with the current Mayo criteria, the ESMO-modified risk stratification model prevents 57% of patients from unnecessary lymphadenectomy at the expense of missing 8.6% of node positive patients. Given the high rate of patients undergoing LND according to the current Mayo criteria, there seems to be a need for an alternative model which safely expands the low-risk group to achieve a precise balance between the desire to prevent over-treatment and the ability to diagnose LN involvement.
 XML Download
XML Download