

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ovarian cancer is a lethal gynecologic cancer, and its incidence and mortality are increasing in Korea [12]. The vast majority of ovarian cancer patients present with advanced-stage disease. Primary debulking surgery followed by postoperative platinum-based chemotherapy is the cornerstone of management for advanced ovarian cancer. Two randomized controlled phase III trials showed that interval debulking surgery (IDS) produces progression-free survival (PFS) and overall survival (OS) equivalent to those of primary debulking surgery. As a result, there is a trend towards neoadjuvant chemotherapy (NAC) followed by IDS [34] for the treatment of advanced high-grade serous carcinoma (HGSC).
To date, there is no uniform consensus regarding the prognostic value of the histopathological grading system to assess NAC response on tumor tissue obtained during IDS. Recently, Böhm et al. [5] proposed a simple and reproducible scoring system for grading the response of tubo-ovarian HGSC to NAC based on histopathological examination of IDS specimens. They reported that the 3-tiered chemotherapy response score (CRS) of omental tissue sections showed a significant association with PFS and OS in their validation cohort, indicating promise in refining the assessment of NAC response in tubo-ovarian HGSCs [5]. However, it is warranted to test whether the good performance of the CRS system is reproducible in diverse clinical settings such as those exhibiting differences in the selection criteria for NAC, extent of surgery, chemotherapy policies, or experience of pathologists. The aim of this study was to validate the CRS system for assessing treatment response in an external cohort of HGSC patients treated with NAC.
MATERIALS AND METHODS
1. Study population
From 2006 to 2014, electronic medical records of patients with tubo-ovarian or peritoneal HGSC who underwent NAC and subsequent IDS in the Department of Obstetrics and Gynecology, Severance Hospital, Yonsei University College of Medicine were retrospectively analyzed. The same inclusion and exclusion criteria as those reported by Böhm et al. [5] were applied. In brief, the inclusion criteria were 1) histopathologically confirmed International Federation of Gynecology and Obstetrics (FIGO) stage IIIC–IV HGSC patients; 2) ovarian, tubal, or primary peritoneal HGSC; and 3) IDS. This study was reviewed and approved by the Institutional Review Board at Severance Hospital, Yonsei University Health System, Seoul, Korea (IRB No. 4-2015-1158).
Regarding primary treatment strategy, the selection criteria for NAC were not described in the study of Böhm et al. [5]. In this study, we applied 2 gate models for primary treatment strategies in advanced HGSCs. All patients had preoperative computed tomography (CT) and positron emission tomography (PET)/CT. NAC was performed for those who 1) developed pulmonary and/or hepatic parenchymal metastasis in imaging analyses; 2) were medically inoperable; and 3) were judged unsuitable for optimal debulking surgery due to high tumor burden based on the Fagotti's score (scored over 8) [6]. All surgical procedures were performed by a gynecologic oncology team comprising 5 experienced gynecologic surgeons. IDS was performed via long midline laparotomy, hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and pelvic and paraaortic lymphadenectomy, with or without various radical surgeries (e.g., bowel resection, diaphragmatic resection, and peritonectomy). After surgery, patients received 3–6 cycles of postoperative adjuvant chemotherapy (POAC). Both NAC and POAC were routinely given as a combination of carboplatin and taxane. All therapeutic procedures were provided according to the National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology [7].
2. Pathology review
The resected specimens were formalin-fixed and paraffin-embedded according to standard procedures and stained with hematoxylin and eosin (H&E) in the Department of Pathology, Severance Hospital, Yonsei University College of Medicine. All available H&E-stained slides obtained from IDS specimens were reviewed by an experienced gynecologic pathologist (H.S.K.). The slide with the most viable tumor and/or the least chemotherapy response was selected from each of 3 sites: omentum, right adnexa, and left adnexa. Three pathologists (H.S.K., H.M.K., and C.K.P.) independently scored each slide according to the 3-tiered CRS system proposed by Böhm et al. [5]. In brief, CRS 1 indicates no or minimal tumor response; mainly viable tumor with no or minimal regression-associated fibroinflammatory changes, limited to a few foci; and cases in which it is difficult to decide between regression and tumor-associated desmoplasia or inflammatory cell infiltration (Fig. 1A). CRS 2 indicates appreciable tumor response amid viable tumor that is readily identifiable; multifocal or diffuse regression-associated fibroinflammatory changes with viable tumor in sheets, streaks, or nodules; and extensive regression-associated fibroinflammatory changes with multifocal residual tumor, which is easily identifiable (Fig. 1B). CRS 3 indicates complete or near-complete response with no residual tumor; minimal irregularly scattered tumor foci seen as individual cells, cell groups, or nodules up to 2 mm maximum size; mainly regression-associated fibroinflammatory changes; and no or very little residual tumor in the complete absence of any inflammatory response (Fig. 1C).
Fig. 1
Examples of histopathological features of tumor regression after NAC corresponding to CRS 1 to 3. CRS 1: no or minimal tumor response (A). CRS 2: appreciable tumor response amid viable, readily identifiable tumor (B). CRS 3: complete or near-complete response with no or minimally residual tumor (C).
CRS, chemotherapy response score; NAC, neoadjuvant chemotherapy.

Each pathologist was blinded to the results of other pathologists. Following submission of independent scores for reproducibility analysis, all cases in which the score was not unanimous were reviewed jointly using a multi-headed microscope. The agreed upon consensus score was used for outcome analysis.
3. Statistical analysis
Fleiss' kappa statistics and Kendall's coefficient of concordance were used to assess levels of agreement among the pathologists. Survival outcomes according to the CRS were analyzed. The PFS and OS curves were drawn using the Kaplan-Meier method, and the curves were compared using a log-rank test. Adjusted hazard ratios (HRs) for PFS and OS were estimated with a Cox proportional hazards model. In addition, the performance of CRS was evaluated using the concordance index (c-index). A bootstrap method (1,000 repetitions) was used to obtain more unbiased estimates of the c-index. Statistical significance was defined as a p<0.050. All statistical analyses were performed using STATA ver. 12.0 (StataCorp LP, College Station, TX, USA).
RESULTS
1. Baseline characteristics
We found 115 stage IIIC–IV ovarian cancer patients who underwent NAC followed by IDS in our institutional databases. One hundred and ten (95.7%) patients met the inclusion criteria. Three (2.6%) patients with ovarian clear cell carcinoma and 2 (1.7%) with carcinosarcoma were excluded. The baseline characteristics of the patients are summarized in Table 1. The median age of the patients was 57 years (range, 27–80 years). All patients had histopathologically confirmed HGSC and underwent platinum/taxane-based chemotherapy.
Table 1
Baseline characteristics

2. Interobserver reproducibility of 3-tiered CRS system
The interobserver reproducibility of the 3-tiered CRS system was assessed. The omental CRS showed high reproducibility among the 3 independent pathologists (Fleiss' kappa value=0.656; Kendall's coefficient of concordance=0.669; absolute agreement=71.7%). In addition, we observed comparable reproducibility of the adnexal CRS with that of the omental CRS (Table 2). These findings were not consistent with those from previous data showing that the adnexal CRS showed inferior reproducibility to the omental CRS [5].
Table 2
Fleiss' kappa value, Kendall's coefficient of concordance, absolute agreement, and p-value for 3-tiered CRS system in external validation cohort

3. Association of CRS with patient survival
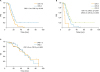
The distribution of CRS in our cohort (CRS 1, 5.5%; CRS 2, 51.8%; CRS 3, 42.7%) was significantly different from that of Böhm et al. [5]'s validation cohort (CRS 1, 0%; CRS 2, 70.0%; CRS 3, 30.0%; p<0.050). In our cohort, the omental CRS displayed a significant prognostic value for PFS between CRS 1–2 and CRS 3; the median PFS of patients with CRS 1–2 and CRS 3 tumors was 14.5 and 18.6 months, respectively (p=0.016; Fig. 2A). There were significant differences in PFS between patients with CRS 1 and CRS 2 tumors (p<0.001) and between those with CRS 2 and CRS 3 tumors (p=0.046), respectively (Fig. 2B). Unlike Böhm et al. [5]'s validation cohort, which exhibited no significant difference in survival between CRS 1 and CRS 2 diseases, we did observe a significant difference between those groups. When adjusted for age, stage, and debulking status, the CRS was an independent prognostic factor for PFS (CRS 1–2 vs. CRS 3; adjusted HR=1.74; 95% confidence interval [CI]=1.05–2.87). A log-rank test revealed no significant difference in OS between CRS 1–2 and CRS 3 (p=0.902; Fig. 2C). With interval validation using the bootstrap method (1,000 runs), the c-index for the Cox model was 0.725 (95% CI=0.650–0.793) for recurrence.
Fig. 2
PFS and OS according to the 3-tiered CRS system in the omentum of tubo-ovarian HGSC patients receiving NAC. PFS according to the omental CRS (CRS 1–2 vs. CRS 3) (A). PFS according to omental CRS (CRS 1 vs. CRS 2 vs. CRS 3) (B). OS according to omental CRS (CRS 1–2 vs. CRS 3) (C).
CRS, chemotherapy response score; HGSC, high-grade serous carcinoma; NAC, neoadjuvant chemotherapy; OS, overall survival; PFS, progression-free survival.
4. Association of CRS with debulking status and platinum resistance
No gross residual disease after IDS was achieved in 23.8% of patients with CRS 1–2, whereas 48.9% of patients with CRS 3 (odd ratio [OR]=3.07; 95% CI=1.36–6.92) had no gross residual disease after IDS. However, there was no significant difference in the rate of optimal cytoreduction (residual tumor <1 cm) between patients with CRS 1–2 and CRS 3 tumors (p=0.785), optimal cytoreduction was achieved in 81.0% of and 83.0% of patients with CRS 1–2 and CRS 3 disease, respectively.
Less than 6 months after last POAC, 83.3%, 26.3%, and 23.4% of patients with CRS 1, 2, and 3 had platinum-resistant diseases, respectively. There was a trend towards an inverse association between CRS and the frequency of platinum resistance (CRS 1–2, 31.8%; CRS 3, 23.4%), although the difference was not statistically significant (p=0.336).
DISCUSSION
The CRS system was successfully used to stratify patients with respect to prognosis. In this study, we performed external validation of the CRS system in an independent cohort of tubo-ovarian HGSC patients, of which the selection criteria for NAC, extent of IDS, surgical skill, and chemotherapy policies are different from those of the original cohort [5]. In our cohort, patients were homogenously selected for NAC and treated with minimization of confounding factors, such as the selection criteria for NAC, chemotherapy policies, and extent of surgery. We demonstrated that the CRS system was highly reproducible and exhibited prognostic significance and predictive value for tumor recurrence in an external cohort.
There is no recommended or agreed system for tumor regression grading for ovarian cancer treated with NAC. Therefore, there is unmet clinical need for a system to assess response to NAC. To date, 4 previous studies have documented tumor regression grading systems after NAC in advanced ovarian cancer [891011]. Although these studies showed a correlation between response to NAC and survival, they did not validate their own criteria in an independent external cohort and did not assess reproducibility. Recently, Böhm et al. [5] proposed a 3-tiered CRS system, validated its prognostic significance, and assessed its reproducibility in 2 independent cohorts. As suggested by Böhm et al. [5], the CRS system is easy to use in practice, cost-free, and reproducible. In this study, we assessed inter-observer reproducibility among 3 independent pathologists in our institution who trained on the 3-tiered CRS system using an electronically available website [12]. The parameters including Fleiss' kappa value, Kendall's coefficient of concordance, and the percentage of absolute agreement indicated high reproducibility of the CRS system.
After the release of the CRS system, concerns were raised that the score is based on omental assessment instead of primary site assessment [131415]. In tubo-ovarian HGSC, multiple intra-abdominal sites including the omentum are involved in addition to the primary site of origin. Considering the intratumor heterogeneity in genomic profiles according to the tumor location in advanced ovarian cancer [16], chemotherapy response is expected to vary between the location of primary and metastatic lesions. Böhm et al. [5] reported a significant correlation between outcome and omental CRS. However, they did not find any significant association between outcome and the adnexal CRS. Similarly, we found that adnexal CRS showed no significant association with outcome (p=0.317; Supplementary Fig. 1).
The CRS system has prognostic significance and can be used to stratify patients after NAC and IDS. In the validation cohort of Böhm et al. [5], there was no significant difference in PFS between CRS 1 and CRS 2. However, a prominent difference in PFS was found between CRS 2 and CRS 3. In this study, we observed a significant trend towards a positive association between CRS and PFS (p<0.001). We also found significant differences in PFS between CRS 1 and CRS 2 (p<0.001) and CRS 2 and CRS 3 (p=0.046), respectively. While the outcomes of patients with CRS 2 tumors were similar to those of patients with CRS 1 in the study of Böhm et al. [5], we observed that outcomes of patients whose tumors exhibiting CRS 2 are similar to those of patients with CRS 3. In other words, the pattern of survival was different between Böhm et al. [5]'s validation cohort and that of ours. The median PFS was 12 months in the CRS 2 group from Böhm et al. [5]'s validation cohort and 15.7 months in the CRS 2 group from our cohort, whereas the median PFS of the CRS 3 group was approximately 18 months in both cohorts. The previous study showed a moderate but insignificant trend toward longer PFS in patients with complete versus incomplete debulking. In this study, residual disease after IDS was the most powerful prognostic factor on multivariate analysis and showed better PFS when complete debulking was achieved (no gross residual vs. any gross residual; adjusted HR=0.49; 95% CI=0.28–0.87). This might suggest that no gross residual disease after IDS overcomes the partial response (CRS 2) after NAC.
In order to determine the discriminatory performance of the CRS system, we calculated the c-index with 1,000 samples after bootstrapping. The c-index is similar to the area under the receiver operating characteristic (ROC) curve for logistic models and is measured on a scale ranging from 0.5 (no better than chance) to 1 (perfect prediction). Given that the c-index for the Cox model was above 0.700, CRS had a good performance in terms of discrimination.
This study has some limitations. First, it was limited by its retrospective nature and by small numbers in some score categories. The characteristics of patients whose tumors display a CRS of 1 and worse prognosis should be clarified to improve outcomes in this disease subset. Second, with increased use of NAC in recent years, our cohort is limited by the short follow-up period. Further studies are necessary to identify outcomes such as OS with long-term follow-up databases.
In conclusion, we demonstrated that the CRS system has prognostic significance in an external cohort of tubo-ovarian HGSC patients. The CRS system is a reproducible prognostic tool for assessing NAC response in patients with HGSC to be externally validated. The addition of treatment response shows promise in improving survival estimates for HGSC patients treated with NAC.
 XML Download
XML Download