

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ultrasonography is an established method for evaluation of tissue echogenicity in cases of suspected thyroid diseases such as Hashimoto's thyroiditis or Graves' disease and an effective tool for detection of focal lesions (1234). On ultrasound (US), decreased echogenicity of thyroid parenchyma is commonly detected; in fact, it has been reported in cases of autoimmune thyroid diseases such as Hashimoto's thyroiditis or Graves' disease (2567). Many studies have correlated sonographic echogenicity of thyroid in patients with Hashimoto's thyroiditis or Graves's disease with thyroid function test results and thyroid autoimmune activity (2389). However, the relationship between decreased thyroid echogenicity and thyroid function test or autoimmune activity in the general population has rarely been studied (7101112). Vejbjerg et al. (11) reported the association between hypoechogenicity or irregular echo pattern on thyroid US and thyroid function in the general population. Likewise, Dvoráková et al. (12), reported a correlation between echogenicity of the thyroid and autoimmune antibodies in a randomly selected population; however, their subject group did not include a large number of patients with decreased echogenicity, and the thyroid parenchyma size was not considered. To our knowledge, the associations of decreased echogenicity, heterogeneous echotexture and thyroid size with thyroid function and autoimmune activity, especially in an asymptomatic population, has not previously been reported.
The purpose of this study was to evaluate the relationships between the degree of decreased thyroid echogenicity, heterogeneity or size with function and autoimmune activity, in an asymptomatic population.
MATERIALS AND METHODS
This retrospective study was approved by our Institutional Review Board, and individual patient consent was waived.
From January 2009 to December 2011, 5611 thyroid US examinations were performed in our institution. The radiologic reports and Picture Archiving and Communication System images of thyroid US were retrospectively reviewed. The patients with images showing decreased parenchymal echogenicity were selected (n = 1457). Decreased echogenicity was defined when more than two-thirds of whole thyroid parenchyma showed lower echogenicity than that of the individual patient's submandibular gland by visual assessment (7). When the echogenicity of submandibular gland was abnormal due to sialoadenitis or connective tissue disease, the echogenicity of parotid gland was considered as a standard. Patients with any focal solid nodule on their thyroid US (n = 459), previous treatment with medication related to thyroid (n = 195), or symptoms related to thyroid (n = 126) were excluded. Our study only included asymptomatic patients. Cases without serum triiodiothyronyne (T3), free-thyroxine (fT4), and thyrotropin (TSH) results (n = 134) were also excluded. Finally, a total of 543 asymptomatic patients with decreased parenchymal echogenicity were included in the study.
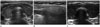
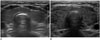
Thyroid US was performed using the HDI 5000 or IU 22 (Philips medical system, Best, the Netherlands) with a 7.5 MHz linear probe. Two radiologists with 5 and 15 years of experience in thyroid US interpreted the US results in consensus. The patients were classified into two groups based on the degree of hypoechogenicity i.e., group A: patients who were hypoechoic relative to the submandibular gland, but hyperechoic relative to strap muscle (Fig. 1A, B); and group B: patients who were isoechoic or hypoechoic relative to strap muscle (Fig. 1C) (7). We also divided the patients with decreased echogenicity into homogeneous (group Ho) and heterogeneous groups (group He) (Fig. 2). Group He was defined when the US showed multiple scattered small hypoechoic nodules in whole thyroid parenchyma. We then classified the patients into three groups based on thyroid size i.e., group 1: patients who had a decreased thyroid size (< 1.2 cm at the thickest anteroposterior diameter); group 2: patients whose thyroid was within normal size range (1.3–1.8 cm anteroposterior diameter); and group 3: patients who had an increased thyroid size (> 1.9 cm at the thickest anteroposterior diameter) (Fig. 3). Normal thyroid dimension were reported as 13–18 mm anteroposterior diameter in adult population (1314). Additionally, we reviewed the serum levels of T3 (reference value: 0.89–1.68 ng/mL), fT4 (reference value: 0.88–1.44 ng/dL), TSH (reference value: 0.35–5.50 uIU/mL), anti-thyroglobulin antibody (TgAb) (reference value: ~40 IU/mL), thyroid peroxidase antibody (TPOAb) (reference value: ~35 IU/mL), and anti-TSH receptor antibody (TSH-rAb) (reference value: ~1.75 IU/L). T3, fT4, and TSH levels within the reference value were classified as normal, higher than upper limit of reference value were classified as elevated level, and lower than lower limit of reference value were classified as low. TgAb, TPOAb, TSH-rAb levels within the reference value were defined as negative, and higher than reference were defined as positive.
The comparisons of the thyroid function test and anti-thyroid antibody levels among the groups were analyzed using the Pearson chi-square test. The statistical significance threshold value was considered as p < 0.05.
RESULTS
The 543 patients included 133 men and 410 women with a median age of 42 years (range: 9–82 years). The number of patients in group A was 448 (82.5%) and in group B, 95 (17.5%). Homogeneous decreased echotexture (group Ho) was observed in 109 patients (20.1%) and heterogeneous echotexture (group He), in 434 patients (79.9%). Nineteen patients (3.5%) had a decreased thyroid size (group 1), 184 patients (33.9%) had size within the normal range (group 2), and 340 patients (62.6%) had an enlarged thyroid (group 3).
T3, fT4, and TSH levels differed significantly between groups A and B (p < 0.001, p = 0.001, p < 0.001). In group B, T3 was low in 14.7%, elevated in 32.6% of the patients and fT4 was low in 17.9%, elevated in 36.8%; while TSH was low in 37.9%, and elevated in 26.3% of the patients. In group A, T3 was low in 23.7% and elevated in 15.8% of the patients; fT4 was low in 10.9% and elevated in 23.0%; while TSH was low in 23.7% and elevated in 15.2% of the patients. TSH-rAb levels did not differ between groups A and B (p = 0.65). TgAb and TPOAb levels in group B showed significant positivity, as compared with those in group A (p = 0.006, p < 0.001). Fifty-nine percent of group B showed a positive TgAb, and 67.6% showed positive TPOAb. On the other hand, 34.8% and 34.9% of group A showed positive TgAb and TPOAb (Table 3).
T3, fT4, TSH, TgAb, and TSH-rAb levels were not significantly different between groups He and Ho, though TPOAb level was significantly positive in group He (p < 0.001). 48.5 % of group He and 19.4% of group Ho showed positive TPOAb (Table 4).
Among groups 1, 2, and 3, the T3, fT4, and TSH levels were significantly different (p < 0.001), especially between groups 2 and 3. T3, fT4, and TSH levels were normal in 60.9%, 73.9%, and 70.7% of group 2, respectively; and in 58.2%, 56.2%, and 49.4% of group 3, respectively. In group 2, T3 was low in 33.2% and elevated in 6.0%; by contrast, in group 3, T3 was low in 15.3% and elevated in as many as 26.5%. In group 2, fT4 was elevated in 14.7%, but in group 3, it was elevated in 32.4%. In group 2, TSH was low in 12.0% of patients, but in group 3, it was low in 34.1%. TSH-rAb and TPOAb showed significant positivity in group 3 relative to group 2 (p < 0.001, p = 0.017); whereas, the TgAb level was not significantly different among groups 1, 2, and 3 (p = 0.084) (Table 5).
DISCUSSION
Diffusely decreased echogenicity of the thyroid parenchyma is a well known sonographic finding in autoimmune thyroid disease such as Hashimoto's thyroiditis and Graves' disease (45815). Hypoechogenicity is caused by reduction of colloid content, increased intrathyroidal blood flow or lymphocytic tissue infiltration (8). Many studies have focused on the relationship of laboratory parameters to thyroid echogenicity in patients with Hashimoto's thyroiditis or Graves' disease (2389). Schiemann et al. (3) noted that decreased echogenicity was correlated with TSH and TSH-rAb levels in patients with Graves' disease; and Schiemann et al. (8) reported that high-grade hypoechogenicity was associated with increased TSH levels and highly elevated TPOAb in patients with Hashimoto's thyroiditis. However, these findings pertain only to specific conditions such as Hashimoto's thyroiditis or Graves' disease. More notably, Vejbjerg et al. (11) demonstrated an association between reduced echogenicity and/or irregular echo pattern and high values of TSH and TgAb/TPOAb positivity in the general population. Moreover, in a randomly selected population, Dvoráková et al. (12), reported highly significant relationship between decreased echogenicity and TgAb/TPOAb. In the present study on asymptomatic population, cases with decreased thyroid echogenicity showed significantly positive TgAb and TPOAb; and significant TPOAb positivity was observed in patients with heterogeneous decreased echogenicity. The patients with enlarged thyroid showed significantly elevated levels of TSH-rAb and TPOAb. Additionally, T3, fT4, and TSH levels in the group with more severe decreased echogenicity were significantly abnormal (either decrease or increase) relative to those with mild decreased echogenicity. T3 were abnormal in 47.4% of the more decreased echogenicity group and in 39.5% of mild decreased echogenicity group. The fT4 and TSH levels were abnormal in 54.7% and 64.2%, respectively, of the more decreased echogenicity group. These results differed from Vejbjerg et al.'s (11), possibly due to a difference in the analysis of T3, T4, and TSH levels. We divided the T3, T4, and TSH levels into low, normal and elevated groups, whereas Vejbjerg et al. used the mean serum TSH level. The difference might also have been caused by our inclusion of questionable Graves' disease and Hashimoto's thyroiditis, which could have shown decreased echogenicity on thyroid US. In our study, 59% and 67.6% of the patients with severe decreased echogenicity showed positive levels of TgAb and TPOAb. Of the patients with heterogeneous decreased echogenecity, 48.5% showed TPOAb positivity, very similar to the result of Vejbjerg et al. (48.5%). Additionally, in our study, patients with decreased echogenicity and thyroid enlargement showed significantly increased levels of TPOAb and TSH-rAb.
The key to the diagnosis of autoimmune thyroid disease is detection of elevated anti-thyroid antibody titers, which include TgAb, TPOAb, and TSH-rAb (1617). Ultrasonography, while not a diagnostic method for autoimmune thyroid disease, is nonetheless helpful for evaluation of thyroid echogenicity. Considering our results, each US findings of markedly decreased, heterogeneous echogenicity and thyroid enlargement in an asymptomatic population can be helpful for predicting autoimmune thyroid disease. In such cases, an asymptomatic population might also show abnormal T3, fT4, and TSH levels, as compared to mild decreased echogenigity, homogeneous echogenicity or normal thyroid size. Therefore, when an asymptomatic population shows markedly decreased echogenicity or heterogeneous decreased echogenicity or decreased echogenicity with thyroid enlargement, the possibility of autoimmune thyroid disease can be predicted, and further evaluation such as thyroid function test and anti-thyroid antibody test can be recommended.
Our study has several limitations. First, it was a retrospective analysis, hence, a more controlled and prospective trial is needed to determine the exact significance of thyroid US in the prediction of autoimmune thyroid disease. Second, since the gray scale score was not used in measuring sonographic echogenicity, this study cannot be considered as objective. However, our experts reached a consensus on echogenicity (degree of decreased echogenicity and heterogenicity) and thyroid size measurement results. Studies employing a more standardized gray scale are needed. Third, ultrasonographic thyroid volume was not measured objectively due to the retrospective nature of the study. In most adults, the thyroid measures between 1.3 and 1.8 cm at the thickest anteroposterior dimension. The thyroid gland with an anteroposterior diameter of > 2 cm is considered as enlarged (1314). Fourth, because the population of this study was asymptomatic, it was heterogeneous including cases of both Hashimoto's thyroiditis and Graves' disease. Correspondingly, the serum levels of T3, fT4, and TSH showed no significant linear correlation, and therefore, statistical interpretation was very difficult. Because T3, fT4, and TSH levels were highly variable, ranging from extremely low to extremely high, we concluded that comparison of the median values among the groups would not be effective. Fifth, we did not compare the patients showing decreased echogenicity with those showing normal echogenicity. Many papers have already reported that patients with decreased echogenicity manifested significantly different thyroid function and autoimmune activity from those of patients with normal echogenicity (1112). Therefore, we focused on patients with varying degrees of decreased echogenicity.
The role of thyroid US in asymptomatic population is uncertain. However, the widespread use of US may lead to increased detection of decreased echogenicity on thyroid US. In conclusion, although they had no symptom related to the thyroid, the patients with each sonographic findings of markedly decreased, heterogeneous echogenicity or thyroid enlargement may have abnormal thyroid function test and autoimmune activity. These findings may facilitate the physicians' decision to order tests for thyroid function and autoimmune activity.






 XML Download
XML Download