

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The measurement of serum specific IgE (sIgE) is a valuable supplementary test in the diagnosis of immediate type allergic reactions to foods, pollens, and Hymenoptera venoms. Reported methods exclusively designed for quantitatively measuring sIgE in serum include the ImmunoCAP (CAP; Phadia AB, Sweden) [1], and the IMMULITE 3gAllergy (IMMULITE; Siemens Healthcare Diagnostics, USA) [2]. Other methods for screening for the presence of multiple sIgEs include the multiple-antigen simultaneous test (Hitachi Chemical Co., Japan) [3], and the fluorescence allergosorbent test (Mitsubishi Chemical Medience Co., Japan) [4]. Of these four immunoassay methods, only CAP and IMMULITE can quantitatively measure Hymenoptera venom sIgE, and use fluorescent enzyme and chemiluminescent enzyme detection technologies, respectively, on automated platforms.
Many published studies involving the measurement of sIgE to Hymenoptera venom have used CAP [5, 6]. Although few published studies have used IMMULITE to measure sIgE to Hymenoptera venom, one study indicated that the accuracy of IMMULITE was much better than that of CAP in measuring sIgE when compared with skin testing [7]. This study, however, was conducted in a European population. Since The prevalence of Hymenoptera venom allergy in Japan [8] may be higher than in European populations when compared to epidemiologic studies reported in the 2011 British Society for Allergy and Clinical Immunology guidelines [9], especially among adults such as forestry workers who have a high risk of occupational exposure to Hymenoptera [10], it is important to establish viable diagnostic methods for Asian populations [11]. Additionally, at least one previous study has demonstrated the clinical significance of low levels of sIgE to Hymenoptera venoms. Grunwald et al. [12] detected sIgE to honeybee venom at 0.23 IUA/mL in a patient with a systemic response, and confirmed the diagnosis using a recombinant allergen specific for honeybee acid phosphatase, Api m 3. Therefore, in this study, we assessed the sensitivity and the specificity of IMMULITE and CAP for detecting sIgE to Paper wasp (WA) and Yellow Jacket (YJ) venom in a Japanese population by comparing results to responses to these two types of Hymenoptera stings, and history of systemic reactions according to the clinical history.
Go to : 
MATERIALS AND METHODS
Clinical history was obtained from patients who are forestry workers. This population has a high risk of exposure to WA or YJ sting, and low prevalence of stings by honey bees or other Hymenoptera [10]. Patients had a history of anaphylactic reactions caused by unidentified Hymenoptera stings. Anaphylaxis was defined as emergence of symptoms affecting at least two major organ systems occurring rapidly after exposure, in accordance with established guidelines [13].
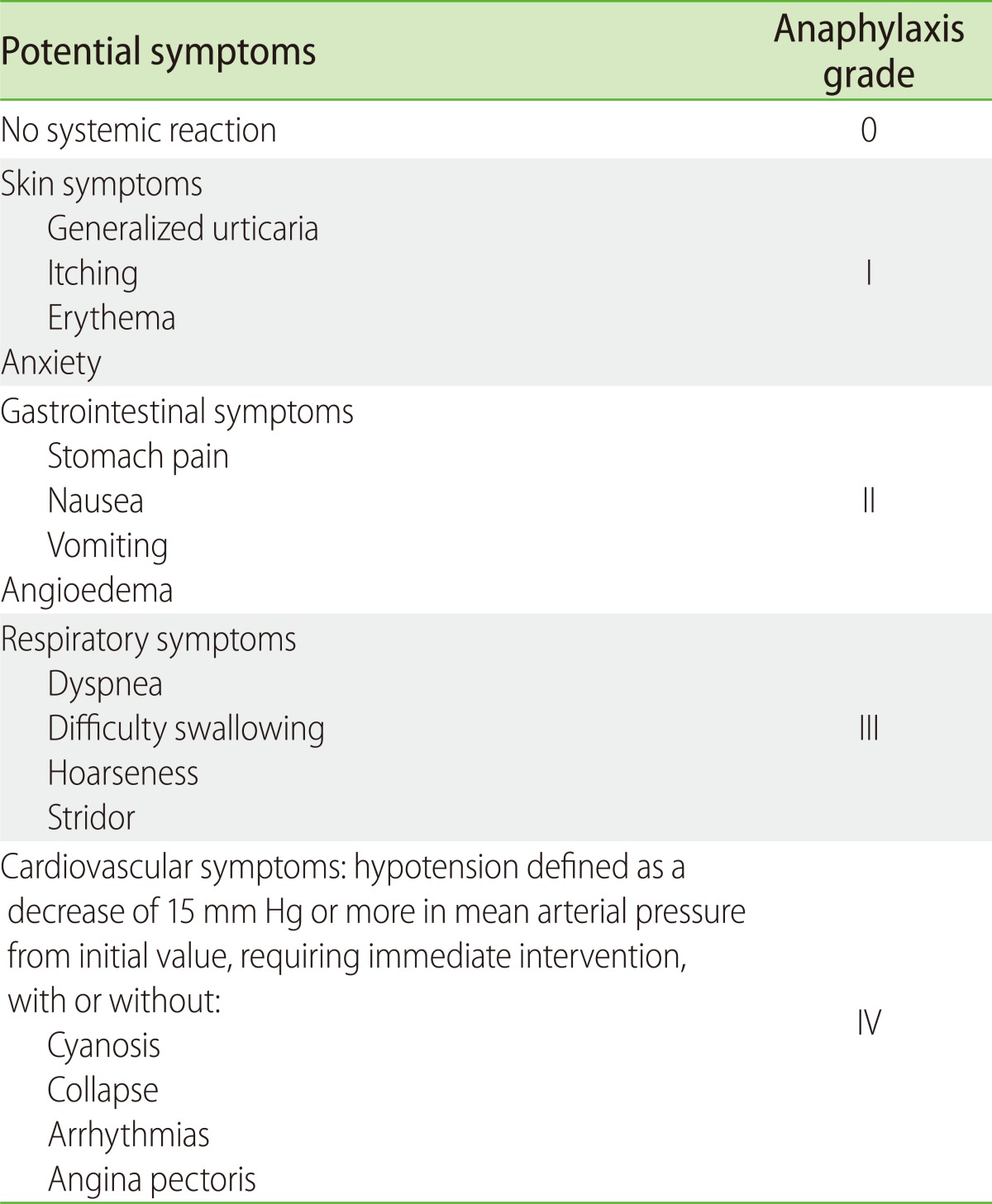
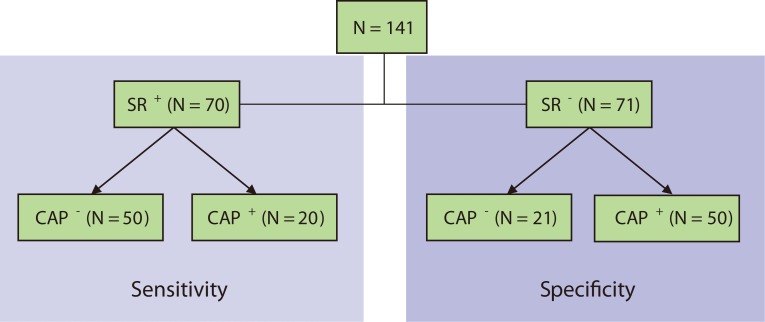
This study was approved by the Dokkyo Medical University Research Ethics Committee and written informed consent was obtained from each participant prior to study enrollment. A total of 141 participants were enrolled; 70 patients reporting a previous systemic (anaphylactic) reaction to a Hymenoptera sting were enrolled to assess sensitivity, while 71 individuals reporting no history of Hymenoptera sting were enrolled to evaluate specificity. All participants completed questionnaires and underwent peripheral blood tests between July and November 2009 using CAP. The questionnaire was administered by an allergist and collected information on age, sex, history of Hymenoptera stings, history of a systemic reaction (SR), and severity of SR. The severity of anaphylactic reaction was classified according to the method of Mueller [14] (as summarized by Biló et al. [15]) and is outlined in Table 1. The symptoms of each participant were classified according to the most severe symptoms he or she had experienced.
To assess sensitivity, we used the IMMULITE WA and YJ assays to test the serum of 50 participants with a history of anaphylactic reactions following Hymenoptera stings, but who had tested negative for sIgE to both WA and YJ venom according to the initial CAP testing. As the control, we used IMMULITE to test serum from 20 participants with a history of anaphylactic reactions to Hymenoptera stings and positive CAP tests for sIgE (≥0.35 IUA/mL). The history of Hymenoptera sting(s) with or without an anaphylactic or other hypersensitivity reaction was directly confirmed by an allergist familiar with each participant.
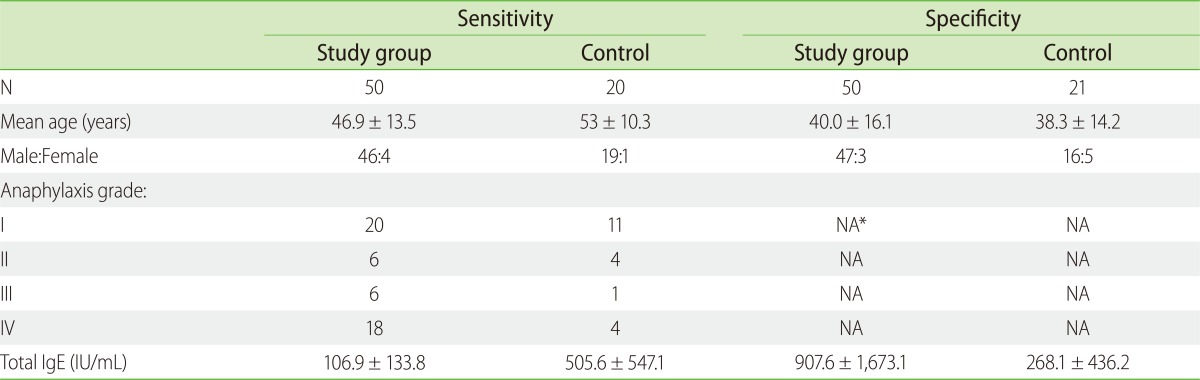
To assess specificity, we used IMMULITE to test serum from 50 participants who reported they were Hymenoptera sting-naïve, yet who tested positive using the CAP tests for sIgE to either WA or YJ (results ≥ 0.35 IUA/mL). The control for this part of the study consisted of 21 participants without history of Hymenoptera stings by self report who were negative using these CAP tests (<0.35 IUA/mL). Population characteristics for each of these four groups are described in Table 2. Fig. 1 presents as flowchart illustrating cohort assignment.
The CAP system expresses the results of tests for sIgE in quantitative units (IUA/mL) and has a working range of 0.35-100 IUA/mL. Similarly, the detection of sIgE by the IMMULITE is expressed as quantitative units (IUA/mL), and has a working range of 0.1-100 IUA/mL. The interpretations of positive results for CAP or IMMULITE are based on values ≥ 0.35 IUA/mL or ≥ 0.1 IUA/mL, respectively.
The differences between groups were examined for statistical significance by analysis of variance using Bonferroni's test. Correlations were tested with Spearman's rank test. P values less than 0.05 were considered significant.
Go to :
RESULTS
Two-by-two contingency tables were constructed to evaluate the sensitivity and specificity of each of the assays compared to SR; agreement was also calculated. Results of the YJ assay for IMMULITE and CAP vs. SR are shown in Tables 3A and 3B; WA results are in Tables 4A and 4B.
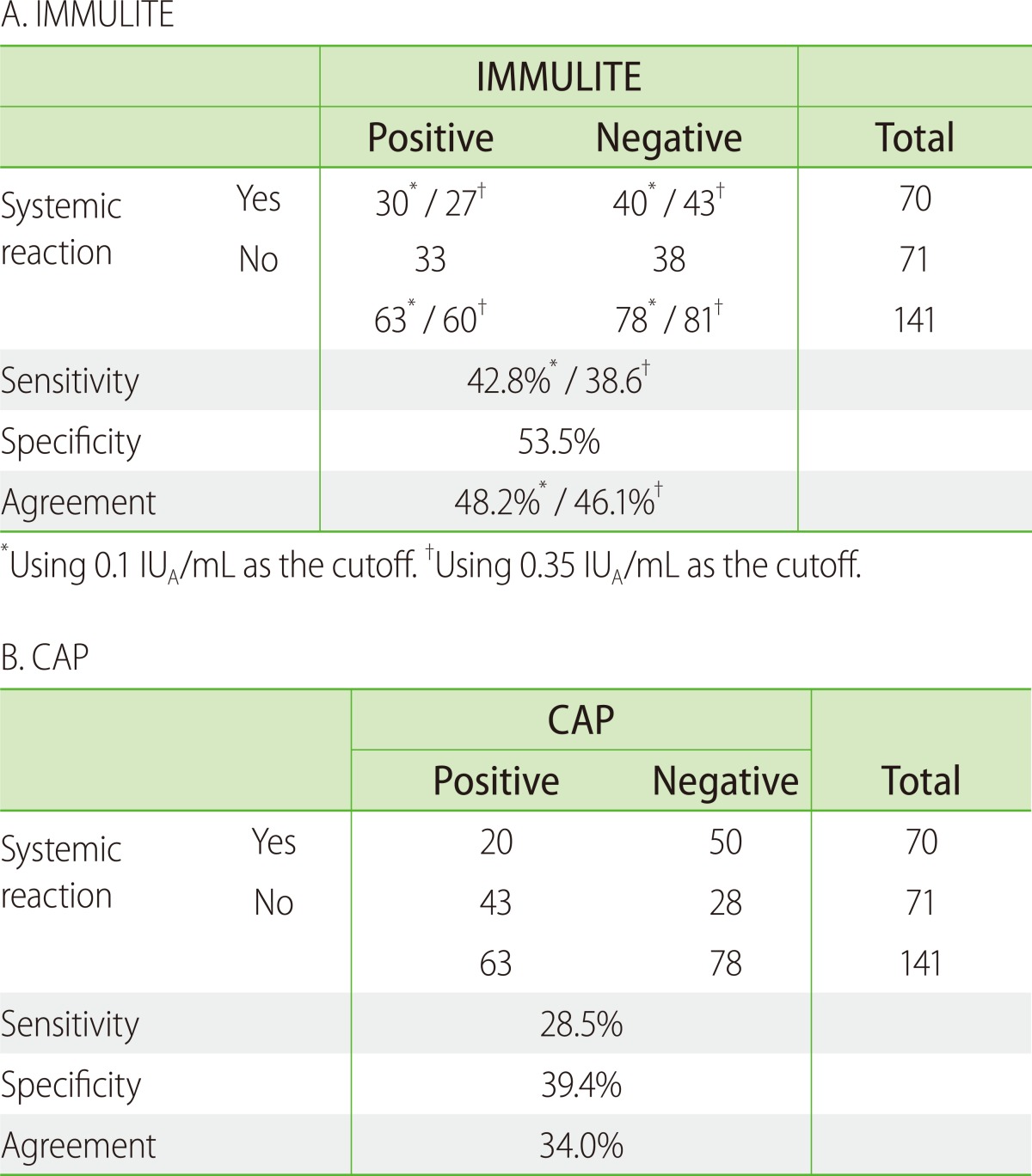
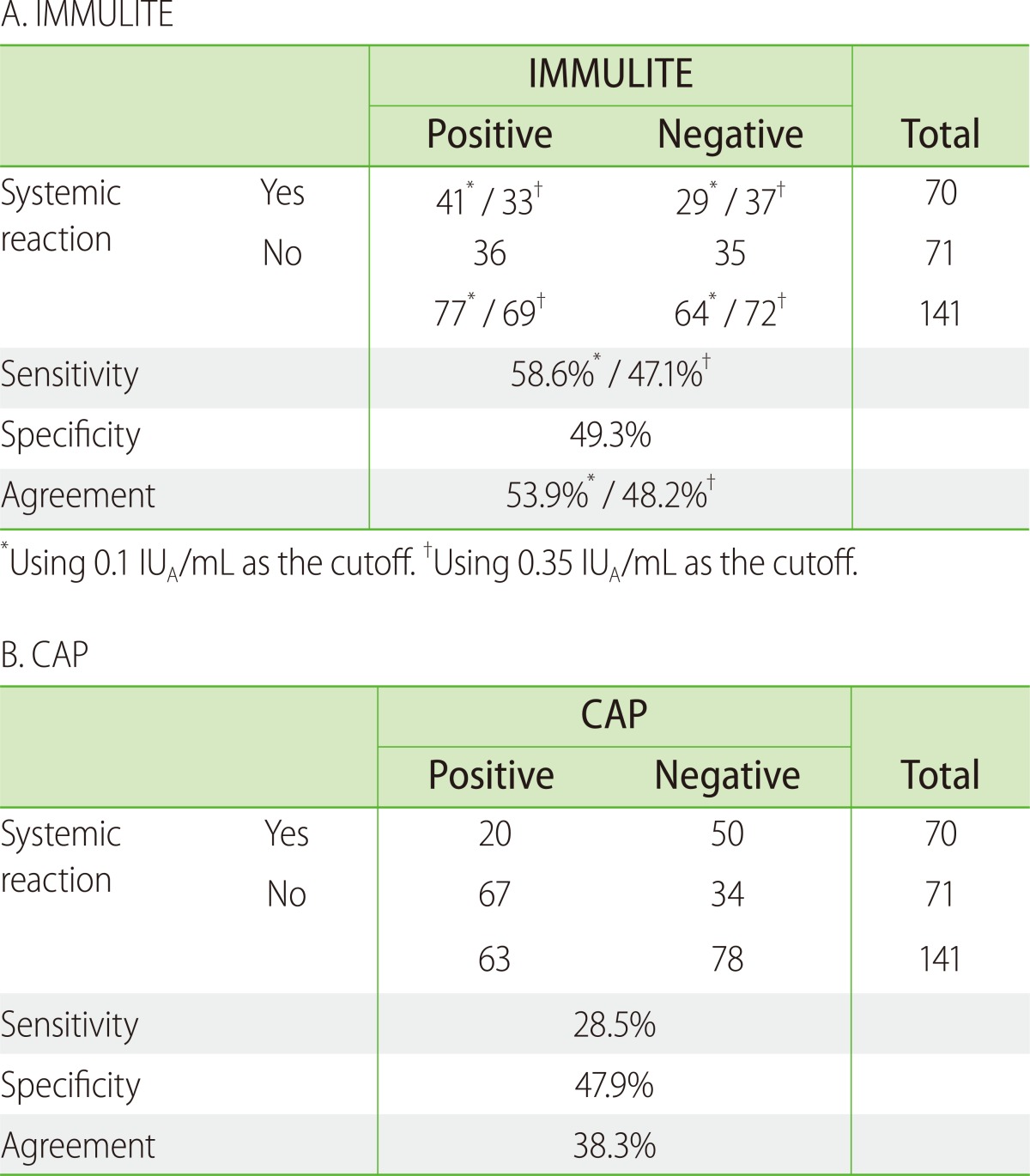
Among the 50 participants who had a history of Hymenoptera stings but were negative according to CAP for YJ and WA sIgE, 10 (20%) were positive for YJ sIgE according to IMMULITE, and 21 (42%) were positive for WA sIgE. When the CAP cutoff value of 0.35 IUA/mL was applied to the IMMULITE data from the same participants, only 7 (14%) of the 50 CAP-negative participants were positive for YJ sIgE, and 13 (26%) were positive for WA sIgE (Tables 3 and 4, Fig. 2). Overall, sensitivity for the IMMULITE YJ assay was 42.8% when the manufacturer's 0.1 IUA/mL cutoff was applied, and 38.6% when the 0.35 IUA/mL CAP cutoff was applied. For the IMMULITE WA assay, sensitivity was 58.6% at the 0.1 IUA/mL cutoff and 47.1% at the 0.35 IUA/mL cutoff. Sensitivity for both CAP assays was lower at 28.5%.
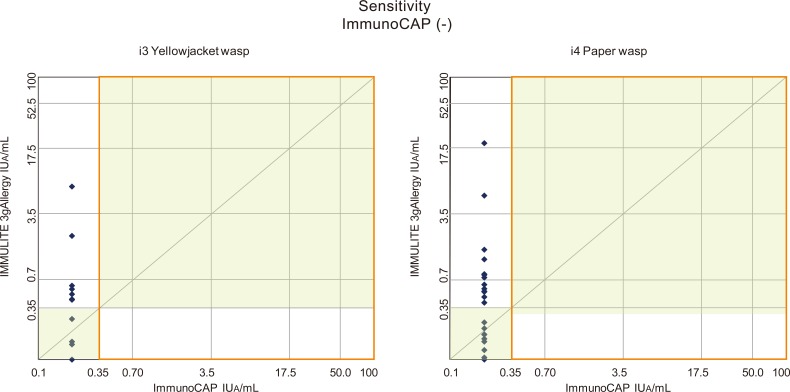 | Fig. 2Quantitative results for Hymenoptera sIgE according to IMMULITE 3gAllergy (IMMULITE) using its 0.1 IUA/mL cutoff among the 50 participants who had a history of Hymenoptera stings but who tested negative according to ImmunoCAP (CAP) (<0.35 IUA/mL). Results demonstrate IMMULITE's sensitivity relative to CAP.
|
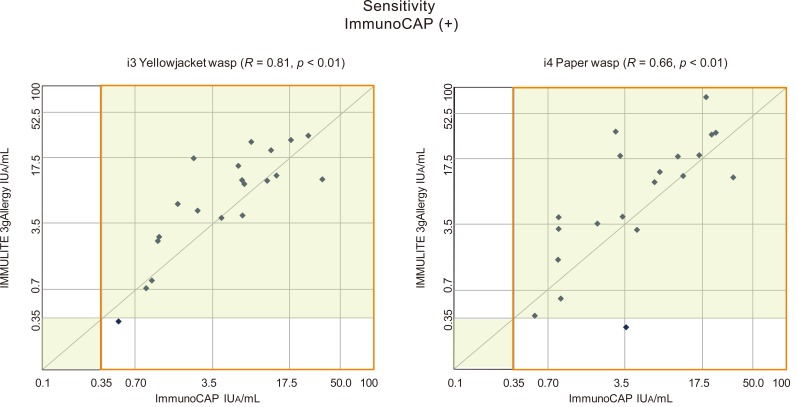
We also analyzed correlation between the two systems for participants who were reported positive by both systems (n = 20, Fig. 3). The correlation coefficients were R = 0.81 (p < 0.01) for sIgE to YJ, and R = 0.66 (p < 0.01) for sIgE to WA. These results were similar to those reported by Hamilton et al. [16].
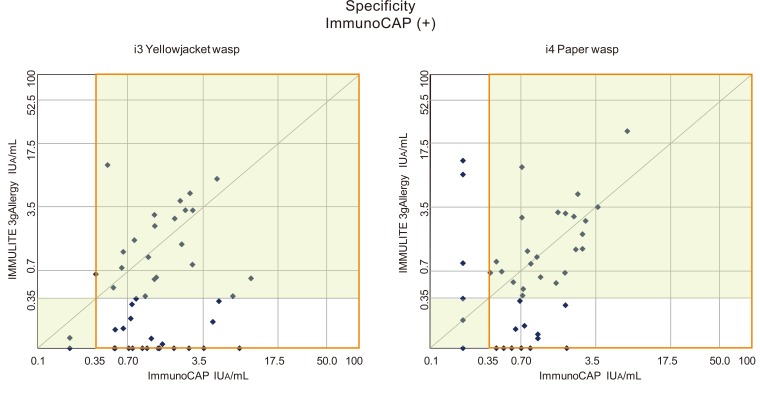
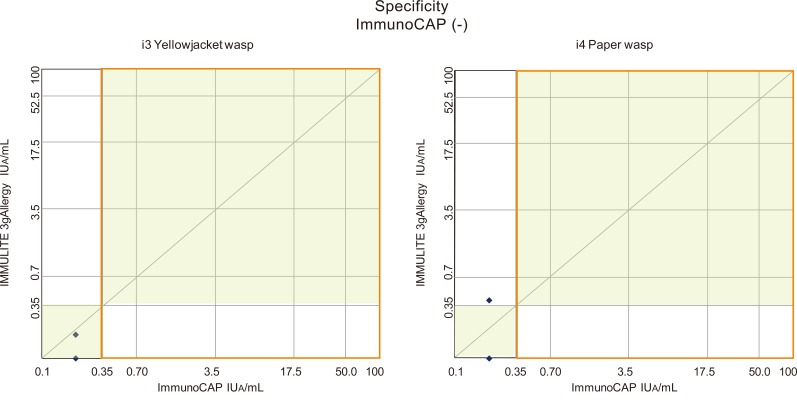
Of the 71 Hymenoptera sting-naïve participants, 21 tested negative for sIgE to both YJ and WA according to CAP (thus presumably representing the true negative population). One patient sample that was CAP-negative yielded a low positive-result according to IMMULITE. This single IMMULITE low positive-result could represent a false positive resulting from cross-reactivity to an antigen similar to Hymenoptera venom, possibly as a result of involvement of cross-reactive carbohydrate determinants (CCD) as described by Hemmer et al. [17]. Alternatively, it may actually reflect a true positive-result in a participant who had sustained a previous sting or stings, but had no recollection or record of it.
Interpretation of tests results for the 50 participants who had no history of Hymenoptera stings, yet who initially tested positive according to CAP is more challenging. This group was retested for sIgE to YJ and WA venoms using CAP at the time of this study, and also tested using the corresponding IMMULITE assays. Upon retest, CAP reported 7 of the 50 sera (14%) were negative for YJ sIgE, and 14 (28%) were negative for WA sIgE. According to IMMULITE, 18 (36%) were negative for YJ sIgE and 15 (30%) were negative for WA sIgE (Figs. 4 and 5). Combining the results from this group with the 21 participants who appear to represent true negatives (20 for IMMULITE) suggests that specificity is poor for both methods, although the IMMULITE showed potentially higher specificity for both YJ venom (IMMULITE vs. CAP YJ sIgE: 53.5% vs. 39.4%) and WA venom (IMMULITE vs. CAP WA sIgE: 49.3% vs. 47.9%).
Go to :
DISCUSSION
The question remains as to why any of the participants in this group tested positive for sIgE to insect venom when there had been no previous exposure. As mentioned above, the large number of positive results could have arisen through cross-reactivity with CCDs. At least three of the major Hymenoptera venom allergens-phospholipase A2, hyaluronidase, and acid phosphatase are reported to be glycoproteins containing Manα1-6(Xylβ1-2)Manβ1-4GlcNAcβ1-4(Fucα1-3)GlcNAc (MUXF) carbohydrate configurations [18]. Cross-reactivity to CCD has been noted to occur in patients already sensitized to glycoproteins bearing similar MUXF carbohydrate groups found in pollens, as well as to those found in natural rubber latex [19, 20]. Another possibility to consider is that at least some of the participants in this cohort may have experienced a previous sting by either a wasp or yellow jacket, or even by another species of Hymenoptera, and were either unaware of the event or had forgotten it. In this case, many individuals who were previously sensitized and thus CAP-positive may have lost sensitization to Hymenoptera venom over time, and now report as CAP-negative/IMMULITE-negative [15, 21].
In general, the IMMULITE assays demonstrated better agreement with SR than the CAP assays. Agreement for the IMMULITE YJ assay was 48.2% at the 0.1 IUA/mL cutoff and 46.1% at the 0.35 IUA/mL cutoff, while agreement for the CAP YJ assay was 34.0%. For the IMMULITE WA assay, agreement was 53.9% at the 0.1 IUA/mL cutoff and 48.2% at the 0.35 IUA/mL cutoff, while agreement for the CAP WA assay was 38.3%.
Although sensitivity, specificity, and agreement for sIgE to suspected Hymenoptera venom exposure are low for both systems with respect to systemic reaction, all of these parameters are greater for IMMULITE than for CAP. While the difference in sensitivity in particular between the assays could simply be a reflection of IMMULITE's lower cutoff level (0.1 IUA/mL vs. CAP's 0.35 IUA/mL), sensitivity remained better using the IMMULITE assay even when CAP's 0.35 IUA/mL cutoff was applied. Specificity for IMMULITE also remained higher than for CAP when the 0.35 IUA/mL cutoff was applied to this analysis. Detection of different antibody epitopes with better specificity and/or affinity for Hymenoptera venom antigens could provide a possible explanation for IMMULITE's better performance. It is also possible that the two assays direct antibodies to different Hymenoptera venom antigens altogether, with the IMMULITE antibodies being directed toward an antigen(s) that is/are more prevalent or found in a higher concentration in our study population than the CAP antibodies.
There are limitations in this study. These results could have been further confirmed with skin tests for YJ and WA from each participant, although this approach was not applied because of the risk of systemic reaction. It may be argued that specificity should have been determined using a patient population that had experienced a sting from either paper wasps or yellow jackets, but did not express a systemic reaction. Use of this population could confound analysis, however, as it has been reported that sIgE can be detected in 30-40% of those experiencing a Hymenoptera sting but who do not have a systemic reaction, which would be then detected as false-positives [21].
In conclusion, we found that the overall positive rate for sIgE to both WA and YJ from the participants who had history of anaphylactic reactions and negative CAP tests was 20-42% when evaluated using the IMMULITE quantitative assay using the manufacturer's reported LoD of 0.1 IUA/mL, and was 14-26% when the CAP cutoff of 0.35 IUA/mL was used. Additionally, sensitivity, specificity and agreement were higher with the IMMULITE than with the CAP, regardless of the cutoff. Thus, the IMMULITE proved useful in detecting sIgE to Hymenoptera venom and may in fact be better for diagnosing patients with suspected Hymenoptera anaphylaxis.
Go to :
 XML Download
XML Download