

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Chronic urticaria (CU) is defined as the urticaria persisting for more than 6 weeks. However, the etiology is frequently deemed as unclear, as most classical investigations failed to find the causes [1]. Although approximately one-half of CU cases have been shown to have an autoimmune etiology, the remaining cases have no known etiology or culprit agent despite thorough evaluation [1]. The literature shows that 30% of patients believe that food might be a cause of their CU because variations in the diet, especially those that contain high levels of spices, seasonings, or natural histamine-like substances aggravated their symptoms [2,3]. However, clinically relevant allergies to foods are thought to be rare (occurring in less than 10% of cases) in patients with CU [4].
Food additives are substances used as sweeteners, flavorings, coloring agents, antioxidants or preservatives [5]. There are thousands of substances [6], while relatively few have been implicated in the significant adverse reactions [7]. Of these, tartrazine, benzoate, monosodium glutamate (MSG), sulfite, aspartame, nitrites, salicylate and some colorants have been tipped as the potential culprits for adverse food reactions [5]. Their potential roles in CU pathogenesis have been suggested by a few studies [8-13], but they are still under investigation. The reasons for the lack of evidence could be attributed to the practical difficulty of performing the gold standard test, the double-blind placebo-controlled food challenge (DBPCFC) [14,15]. In addition, the methodological issues such as inconsistent inclusion criteria and the absence of a standardized challenge protocol exist, and the outcome of the DBPCFC is not always satisfactory [11,16,17]. The skin prick test, which is widely used to screen sensitized allergens, is not useful for discriminating food additives hypersensitivity [13]. Assuming the culprit additive depends solely on the patient's subjective symptoms, which are sometimes vague and provoked by unrelated foods. Therefore, the selection of potential culprits among various kinds of food additives is also problematic.
The flow cytometric basophil activation test (BAT) is an in vitro tool to assess the expression of basophil activation markers after antigen stimulation. The test has strengths in that it can detect not only IgE-mediated responses [18-20] but also non-IgE-mediated immediate hypersensitivity [21-26], which means that it can be applied to allergic diseases of which the mechanism is not clearly known. Moreover, the BAT is not time consuming and able to examine multiple antigens at the same time.
In this regards, we assumed that the BAT may be useful for diagnosing food additives hypersensitivity in patients with CU. The present study aimed to explore the association between food additives and CU by the utilization of BAT.
Materials and Methods
Study Population
From October 2011 through March 2013, a total of 15 CU patients (duration >6 weeks) from the division of allergy and clinical immunology of Seoul National University Bundang Hospital (SNUBH) were prospectively and consecutively enrolled in this study. They were included if they reported recurrent aggravations of urticaria by various kinds of food from history including food diary but did not have clear evidence of food-specific IgE by skin prick test or food-specific IgE measurements. Skin prick tests were performed for 55 kinds of common food allergens in Korea (Allergopharma, Reinbeck, Germany) [27], and food-specific IgE were measured by the RIDA Allergy Screen (Rbiopharm, Darmastadt, Germany) or UniCAP system (Thermo Fischer, Uppsala, Sweden). In case of positive skin tests or specific IgE tests, clinical correlation was determined by allergy specialists. All patients voluntarily participated in this study, and provided written informed consent. This study was approved by the institutional review board of SNUBH.
Sample Analysis
The BAT was carried out using a commercially available Flow-CAST® kit (Bühlmann, Schönenbuch, Switzerland) according to the manufacturer's instruction. A total of 15 food additives, which had been previously reported to cause hypersensitivity reactions, were tested using commercial allergens of the CAST®-Allergens (Bühlmann, Schönenbuch, Switzerland), which included MSG, sodium nitrite, tartrazine, sodium salicylate, potassium metabisulfite, sodium benzoate, and food colorant mix I (quinolone yellow, sunset yellow FCF, chromotrope FB, amaranth and new coccine), and food colorant mix II (erythrosine, patent blue V, indigo carmine, and brilliant black BN) [28].
Briefly, BAT was performed using the following steps. The patients' blood was processed within 2 hours after sampling in EDTA tubes. After removing the erythrocytes, the sample was treated with stimulation buffer solution. The cell suspensions were divided into 11 tubes containing two positive controls, one negative control, and the 15 kinds of food additives described above, respectively. Regarding the positive controls, monoclonal antibodies to high affinity IgE receptors and non-specific N-formyl-methionyl-leucyl-phenylalanine (fMLP) were used. The stimulation buffer was added to the tubes for background and negative control. The results of the BAT were expressed as percentages of basophils expressing CD203c which was known to be increasingly expressed on the basophil surface after allergenic stimulation in sensitized individuals and was regarded as a basophil activation marker. The expression of CD203c was detected with anti-CD203c-phycoerythrin. The stimulation index (SI) was calculated as follows:
Stimulation index (SI) = percentage of basophils activated by the food additive / percentage of activated basophils in the negative control.
The BAT was determined to be positive if the basophil activation was ≥5% and the SI was ≥2, in accordance with the manufacturer's instructions.
Results
Characteristics of Study Subjects
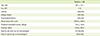
A total of 15 patients with CU were enrolled in this study (Table 1). They had a mean age of 38.7 ± 13.2 years, and 80.0% of them were women. The mean duration of symptoms was 33.0 ± 17.7 months. Only one patients (6.3%) showed elevated peripheral eosinophil counts and 7 patients (46.6%) had elevated total IgE levels ≥250 IU/mL. None had anti-thyroid hormone antibodies. Five patients (33.3%) were positive in skin testing or UniCAP to the food allergens, but all of them did not show any clinical correlations with urticaria.
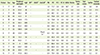
The results of the BAT, skin test and specific IgE test in each patient are summarized in Table 2. Two patients (13.3%) showed positive BAT to any of food additives. The detailed histories of these cases are described as follows.
Patient 1.
A 37-year-old woman visited the outpatient allergy clinic because of urticaria. She suffered from recurrent generalized urticaria, rash, and facial angioedema. She complained that the urticarial aggravation occurred particularly when eating high-seasoned, spicy, or Chinese foods. Previously, she had been treated for allergic rhinitis and also had experienced severe urticaria with a generalized rash after taking non-steroidal anti-inflammatory drugs (NSAIDs). Peripheral eosinophil counts and serum total IgE in her blood were 97.2/µL and 97 kU/L, respectively. T4 and thyroid stimulating hormone were also within normal range. A skin prick test showed weakly positive reactions (wheal size ≥3 mm but allergen/histamine ratio <1) to silk worm pupa, herring, cabbage, celery and walnut; however, none of them provoked urticaria in the history. In the BAT, a total of 18.7% of basophils were activated after stimulation with MSG (Figure 1); however, the other 14 additives did not induce significant basophil activation, compared to the negative control (1.3%).
Patient 2.
A 19 year-old female high school student with recurrent urticaria visited the allergy clinic. She complained of recurrent episodes of localized urticaria and erythematous rashes on face. She had been experiencing urticarial symptoms that had developed after eating a school meal. Her past medical history or family history was unremarkable for allergic diseases. Laboratory findings including peripheral eosinophil count and serum total IgE were within the normal range. The result of an autologous serum skin test was also negative. There were no food allergens which positively reacted to the skin prick test. In BAT, only sodium benzoate activated basophils significantly (37.5% activation; Figure 2). After she abstained from the food additives by avoiding the relevant processed foods, her urticarial symptoms were resolved dramatically without further anti-histamine medications.
Discussion
The present study explored the proportion of patient with food additives hypersensitivity in 15 patients with CU via the utilization of the BAT. All of them had recurrent urticaria aggravated by various food intakes, which did not have evident food-specific IgE against common food allergens. A total of 13.3% of participants showed a positive BAT to any of the tested 15 common food additives, which may suggest a potential clinical utility of the BAT in such cases.
CU can be provoked by specific physical factors, such as pressure, heat, cold, sunlight and even non-specific stimuli [1]. However, for most of the patients with CU, it did not have a well-described cause. Recent advances in the pathogenesis of CU revealed that 45% of patients presented autoimmune markers such as anti-FcεRI-α, anti-IgE or thyroid autoantibodies, and an autologous serum skin test was positive in 4.1-76.5% of cases [29]. However, the etiology of the remaining 55% of patients is still unknown and remained 'idiopathic'.
Many patients regard that urticaria are attributed to food allergies because their symptoms seem to fluctuate according to their diet. There are several reports that 22.5-30.0% of patients regard food as the cause of CU [2,3]. However, contrary to these beliefs, it seems that only less than 10% of CU might be associated with IgE mediated food allergies [30]. Kobra and his colleagues examined the results of DBPCFC and only 10% of patients who complained about food-provoked aggravation of urticaria, reproduced their symptoms [4,31].
The clinical features of CU that can be associated with diet could be somewhat different from those of food allergies. Food allergy is mediated by an IgE-dependent allergic mechanism and is more likely to result in acute urticaria as a generalized allergic reaction. Food allergy also develops in response to only certain foods and/or some foods or vegetables that share antigenic similarity [32]. However, in CU, similar cutaneous reactions could be developed by several apparently unrelated foods and is especially more common as a reaction to commercially prepared forms of foods that are tolerated when prepared at home [33]. These distinct clinical features in CU could arise from food additives, and not from the food itself.
About 3,968 substances are registered in Everything Added to Food in the United States which is regularly updated by the U.S Food and Drug Administration [6]. Despite the great number of food additives, only a few have been implicated in adverse reactions and are mainly mediated through non-IgE mediated immunologic or non-immunologic mechanisms [5]. There have been several case reports on urticaria, angioedema, asthmatic reactions and anaphylaxis caused by food additives [8-13,16,17]. In some of these studies, they performed the oral provocation test for food additives and revealed that hypersensitivity to food additives is the cause of CU [5,8,9,33,34]. However, in these studies, the challenge procedure was executed under poorly controlled circumstances, which were not double-blinded or placebo-controlled. There have been large-scale studies on the prevalence of food additives hypersensitivity in the general population and it has been reported to be quite low (less than 1%, usually 0.18-0.2%) [35-37]. However, children with atopy seemed to show a higher prevalence of hypersensitivity to food additives [36]. However, these studies also had limitations due to the fact that the criteria for patient selection and study design were not consistent.
The DBPCFC is the gold standard to diagnose hypersensitivity to foods or food additives [32]. However, it is difficult to execute this on patients with CU in actual clinical practice. Patients with CU are usually taking an antihistamine, which should be discontinued for a certain period to perform the challenge test. However this may cause an increase in the activity of CU, and thus cause a false positive reaction to the provocation. On the contrary, if the antihistamine is not sufficiently stopped, a false negative result can occur even though food additives are the cause of CU. It is also difficult to conduct the test in a placebo-controlled manner due to the fact that food additives have their own taste and smell. Additionally, in many cases, it is difficult to select candidate additives solely based on the patients' symptoms and food diaries.
A pseudoallergen-free diet can be an alternative option to determine the possibility of hypersensitivity to food additives as a cause of CU. Previous studies reported that a pseudoallergen-free diet could be effective to reduce the severity of CU [10,16,38-40]. Magerl et al. [40] tested a pseudoallergen-free diet on 140 CU patients, and 34% showed significant improvement on urticarial severity and/or quality of life [40]. However, a pseudoallergen-free diet restricts all preserved and processed food, and even all spices and herbs, eggs, cakes, biscuits, tomatoes, fresh and dried fruits, except for salt and chives. Therefore, it is hard to carry out in real life and might cause nutritional imbalances [38].
There are many attempts to develop in vitro methods to diagnose the cause of CU. Recently, basophils are gaining much attention due to their important roles in CU [41-44]. Basophils play an important role in traditional IgE-mediated food allergies [45]. Due to the biological response in which activated basophils plays an important role in causing an allergic reaction, it would be more suitable to measure basophil responsiveness after antigenic stimulation rather than to measure the level of specific IgE in order to evaluate the clinical reactivity of CU. The BAT measures the level of expression of CD63 or CD203c on basophil surfaces with flow cytometry after stimulation of blood cells with allergen [19,20,46]. CD63 or CD203c, which is used as a basophil activation marker, exists within the secretory vesicles inside the basophil at resting stage, and when the basophil is activated causing secretion of the vesicles, the CD63 or CD203c moves to the surface of cell membrane. The level of degranulation of mediators as a result of basophil activation is known to be directly proportional with the expression CD63 and/or CD203c [47-49].
There are numerous reports on the usefulness of the BAT in various allergic diseases. It proved to be especially useful in diagnosing bee or wasp venom anaphylaxis [50]. The BAT could be used to test the induction of tolerance in children with cow's milk allergy [51]. The BAT is also effective in diagnosing food allergies such as IgE-mediated reactions against pollenderived food [19,20] or wheat [46]. It is also useful to test non-allergic or pseudoallergic reactions including drugs [26] such as muscle relaxants [22], antibiotics [23], NSAIDs [24], and even radiocontrast media [21].
However, the BAT for food additives has not been sufficiently studied yet. Garcia-Ortega and his colleagues confirmed using the BAT that hypersensitivity to sodium metabisulfite induced CU [52]. Ebo et al. reported the case of a patient who had a history of recurrent anaphylaxis after eating cheese, and found that hypersensitivity to the natural dye annatto (Ceska Annato WS E160b), which was positive on the BAT, was the cause of anaphylaxis [53]. In our study, the BAT was performed on CU patients whose symptoms were suspected to be related to hypersensitivity to food additives. The culprit was not clearly identified through their history, food diaries, skin prick tests for common food allergens or other additional laboratory tests. Of these patients, one patient showed a positive BAT to MSG and another to sodium benzoate. In these two patients, no symptom developed when they ate at home, but the conditions deteriorated when they ate outside the home, especially for Chinese foods or soups with plenty of seasonings and spices.
The present study has several limitations. First, we did not perform the DBPCFC for the two positive cases as the patients did not agree to perform the oral provocation tests with each additive. Instead, we instructed them on how to restrict the specific additives in their daily diet. Eventually, their symptoms improved after starting a specific food additive-free diet. Second, our low percentage of participants with the positive food additives BAT (13.3%) could raise questions on its diagnostic utility. Several factors are presumed to be responsible. We tested only 15 kinds of common food additives, which could be insufficient for screening purposes. Another possibility could be due to false negative results of the BAT, as shown in our previous study for taurine [54]. In addition, less stringent inclusion criteria could have influenced the positivity of BAT, and have limited our interpretation on the diagnostic utility. We suppose that the positivity might be increased if the subjects were more specifically selected for food additives reactions with oral provocation tests. Nevertheless, our two positive cases were clinically meaningful, as they could have remained unresolved without the diagnostic investigations. Third, we only performed the BAT for 15 patients with CU. This small sample size limits the interpretation of our results. Due to the quite low prevalence of food additives hypersensitivity and it's as-yet undetermined role, a large-scale study is needed to further evaluate the potential utility of BAT with food additives.
Despite the issues surrounding the use of the BAT for food additives, it could be a good alternative to the oral provocation test as a means to evaluate hypersensitivity to food additives in patients with CU. First, it can be applied not only in IgE-mediated, but also in non-IgE mediated reactions, which means that it can be applied to allergic diseases for which the underlying mechanism is not clearly. In addition, BAT results are not affected by anti-histamine or steroid use. Therefore it can prevent the exacerbation of urticaria stemming from the discontinuance of such drugs as well as false negative results for oral provocation tests due to insufficient discontinuation of drugs. The BAT can be used to evaluate multiple candidate allergens or materials simultaneously and independently. It is not easy to identify the culprits in cases of food additives hypersensitivity. Therefore using the BAT as a screening tool for hypersensitivity to various additives could prevent the need to conduct consecutive oral provocation tests for the numerous potential candidate additives.
Conclusion
The pathogenesis of CU has not been clearly determined, and various environmental factors are suspected to be involved. In our explorative study, two of the 15 (13.3%) participants showed positive results in a BAT using food additives. Although these positive results may appear to be low, they were clinically meaningful as the conditions of these two patients could have remained as 'idiopathic' or 'unexplained' without the identification of the possible causes by the BAT. It warrants further studies evaluating the diagnostic utility of the BAT for food additives in patients with CU.


 XML Download
XML Download