

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The Korea Central Cancer Registry reported that the incidence of cancer in 2010 was 405.1 per 100,000 populations. The severity of cancer have been increased by 92.3% (incidence) and 12.6% (mortality) compared to those in 1999 and 2002, respectively [1,2]. Previous study has reported that malnutrition is a direct cause of deaths in 40 to 50% of cancer patients [3]. Malnutrition in cancer patients occurs due to loss of appetite, therapy-associated complications and psychological factors [4,5]. Consequently, cancer patients experience loss of immune capability, delayed wound repair process, lower quality of life, and increased morbidity and mortality [6-8]. Therefore, nutritional status of cancer patients seems to be an important factor to improve responsiveness to treatment and overall quality of life in cancer patients.
Cancer is treated by surgery, radiation therapy, chemotherapy, and in many cases, combined adjuvant therapies are used for better results. Radiation and chemotherapy affect not only tumor cells but also rapidly proliferating normal cells including oral and gastric mucosa, which create various side effects such as difficulties in food intake [9]. Especially, reduced food intake and tumor-associated cachexic syndrome decrease immune potency and tolerance to the treatment. Furthermore, chemotherapy can induce ageusia or dysgeusia [9-11], which worsen inappropriate dietary intake.
Therefore, appropriate dietary intake and nutritional support are crucial not only to improve nutritional status of the patients but to strengthen the immune ability. Also, patients maintaining appropriate nutritional status are well tolerable to treatment regimen. However, the functions of digestive tract as well as appetite are lower in cancer patients compared to those of healthy people requiring the use of oral nutritional supplements. Previous studies reported that nutritional status of cancer patients was improved by using oral nutritional supplement [8,12], while sensory preference was a major determinant for its use [13]. Also, the palatability of the oral nutrition supplement was the main factor in long term compliance and successful use [14]. Supplement preference can be affected by various factors including taste, color, flavor, after taste and texture. Due to a loss of appetite in patients, oral nutritional supplements are required to consider both nutrition and palatability which needs sensory evaluations by the target group during the course of product development. Therefore, the purpose of this study was to compare sensory evaluation score of trial manufactured oral nutritional supplements to one of the top sellers in the market, and to examine possible differences between patient and control groups. Study results will be applied to develop new oral nutritional supplements to improve the nutritional status of cancer patients.
Materials and Methods
Subjects
The subjects of this study were 30 cancer patients (11 men, 19 women) aged over 20 who were diagnosed to have malignant tumors. The patients were under anticancer treatment or ended the treatment within 6 months. Control group included age- and sex-matched healthy individuals (n = 30) aged over 20, who are not diagnosed to have chronic disease and not taking any medication. Cancer patients were recruited by contacting outpatients enrolled in DMC Bundang Jesaeng Hospital and control subjects were recruited through an in-campus advertisement at Sookmyung Women's University. This study was approved by DMC Bundang Jesaeng Hospital (IMG13-03) and Sookmyung Women's University (SM-IRB-13-0916-006) Institutional Review Boards. Written and informed consents were obtained from all the participants prior to the study.
Survey
In this study, each participant was interviewed by the investigators using a questionnaire. The questionnaire included the subject's gender, age, cancer sites, particular medical conditions, drinking habits, smoking status, use of oral nutritional supplement, and artificial dentition. Also, patients were asked whether they thought their taste had been changed since the diagnosis of cancer.
Trial manufactured products
The oral nutritional supplements used in this study were provided from Erom (Seongnam, Korea). The supplements used for the sensory assessment were 3 types, which include cereal base, cereal base+herb, cereal base+fruit. The compositions of the supplements are listed in Table 1.
The rice bran and fungus (L. edodes) were both obtained from Kyonggi-do, Suwon, Korea. The L. edodes was cultured in a L. edodes culture medium containing rice bran until there was significant mycelia growth. The mycelia of L. edodes and the insoluble rice bran components were then removed by centrifugation, and the polysaccharides were collected from the resulting supernatant by alkali extraction and ethanol precipitation, affording the rice bran exo-biopolymer. The rice bran exo-biopolymer obtained was powdered by lyophilization. Black rice (Super C3GHi) had higher content of cyanidin-3-glucoside (C3G) than currently available cultivated black rice [15]. Black rice (Super C3GHi) was freeze-dried at -30℃ in a vacuum dryer and grinded. Chia seed was purchased from Chia Company (Port Melbourne, Victoria, Australia). Native grass was consist of Citrus unshiu, Angelica gigas Nakai, Cnidium officinale Makino, Polydonati rhizoma, Astragalus membranaceus, Paeonia japonica, Baekbokryeong and Acanthopanax, All ingredients were formulated and irradiated before sealing.
The products are in powder form although it is recommended to mix with milk for extra energy supply. A cereal based oral liquid nutritional supplement with scorched cereal flavor which is used most frequently by cancer patients were used as a control to evaluate sensory preference for trial manufactured. A total of 40 g powder was mixed with 160 mL (cereal base, cereal base+herb) or 180 mL (cereal base+fruit) of whole milk. For the sensory evaluation, a 30 mL portion of each test products were provided.
Sensory evaluation
The sensory evaluation was performed by scoring each test product from 1 (very bad) to 5 (very good) for color, flavor, viscosity and taste. Also, the overall rank of each products were determined. Single blinded evaluation was performed for each product contained in a paper cup at room temperature. Participants were randomly allocated to supplement sequence in order to avoid allocation bias. Before starting the evaluation, participants were seated in a quiet interview room, and asked to score the products. The participants were asked to rinse their mouths with distilled water before evaluating each product. After evaluating each product, subjects were also asked to rank the four supplements in order of preference.
Statistical analysis
The statistic analyses were performed using the SAS 9.2 program (SAS Inc., Cary, NC, USA). All variables were shown in the average ± standard deviation or percentage, and p < 0.05 indicated statistical significance. Differences of socio-demographics and sensory characteristics between the patients and the control were evaluated by the t-test (continuous variables) and chi-square test (categorical variables). Statistical significance about sensory characteristics was determined with one-way analysis of variance (ANOVA). When the ANOVA indicated a significant difference among the means, the differences were further evaluated using Duncan's multiple-range test.
Results
General characteristics of the subjects are shown in Table 2. The average age of the cancer patient group and control group were 59 years (range 19-89) and 53 years (range 40-64), respectively. Highest proportion (30%) of the cancer patients were diagnosed with breast cancer, followed by colorectal cancer (17%) and lung cancer (13%). Among cancer patients, 20% was diagnosed with hypertension, 17% was diagnosed with diabetes, and others had hypothyroidism, cardiac insufficiency, or dyslipidemia.
One individual in cancer patients group was a current smoker, while 23% in the control group was smokers (p < 0.01). None of the cancer patients answered he or she is a current alcohol user, while 43% of the control group answered that they use alcohol (p < 0.0001). There was no difference in artificial dentition (implant, denture) between two groups. Forty% of the cancer patients answered they experienced taste change after being diagnosed with cancer. In addition, 17% of the patients was using oral nutritional supplements.
Sensory assessment results are summarized in Table 3. The cancer patient group showed significant preference differences for test products in flavor (p = 0.0052), viscosity (p = 0.0003), and taste (p = 0.0183). On the other hand, study participants in the control group showed no significant preference differences for test products in all sensory characteristics. For overall preference, both cancer patient group and control group gave the highest rank to the control supplement product which has scorched cereal flavor. Also, the control group showed significantly higher preference for the viscosity of fruit added supplement (p = 0.0058), and for the taste of plain cereal base supplement (p = 0.0327) indicating lowered sensitivity towards viscosity or taste in cancer patients.
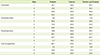
Using the ranking significance test of Basker, overall preference was determined (Table 4). In the cancer patient group, the control supplement product received significantly higher preference (p = 0.05), while no difference in the preference was found in the control group. The proportions of study subjects in each rank (1 to 4) was analyzed (Table 5). However, 66.8% of control subjects preferred fruit-added supplement followed by control supplement.
Discussion
Cancer is a wasting disease, and anticancer treatments cause many side effects including oral and gastrointestinal mucositis, and nausea, which seriously affects the nutritional status of the patient with higher possibility of malnutrition than patients with other diseases [16-18]. The malnutrition condition of cancer patients can affect not only the body function and its maintenance, but also the immune competency and drug metabolism, thus, balanced and active nutrition arbitration which involves protein, vitamin, minerals and sufficient energy is necessary [19]. In this study, a sensory assessment on trial manufactured oral nutritional supplements for cancer patients were performed. Despite the importance of providing proper nutritional support in these patients, the availability of nutrition supplement products are limited. Study results indicated that the control supplement, cereal-based with scorched cereal flavor, is the most preferred product by the patient group. However, no difference in overall preference over test products was observed in control group indicating cancer patients may be more sensitive to the palatability of the supplement due to the loss of appetite. Previous study reported that chemotherapy had variable influence on both taste sensitivity and perceived intensity of the taste [20]. Our results also indicated that fruit added supplement was more preferred than plain cereal base or herb base supplements, although the difference was not significant.
Not only to provide appropriate calorie and macronutrients, oral nutritional supplements in the market are enriched with other bioactive components such as eicosapentaenoic acid (EPA) and Bifidobacterium [21,22]. A previous study indicated that supplementation based on an oral powder formula enriched with EPA improved inflammatory parameters [21] in cancer patients. Trial manufactured products used in our study include grind chia seed rich in omega-3 fatty acids as well as other phytochemicals which is known to suppress inflammatory responses. However, due to granule-like residues present in these products, patient group gave lower score compared to the complete liquid type control product. Therefore, it might be necessary to improve palatability of value-added oral nutritional supplements. Oral nutritional supplements can be provided either in liquid or powder form, however cancer patients frequently find it difficult to chew and swallow, and most of the supplements are sold in a liquid form. In Korea most oral nutritional supplements are in a liquid form providing 200 kcal/200 mL. However, test products used in this study are supplied as a powder form (40 g) which is recommended to mix with 200 mL of milk or soy milk to provide 275-285 kcal.
Most of the cancer patients exhibit loss of appetite and taste change during their illness and treatment. Therefore, it is important to improve palatability of oral nutritional supplements and increase the variety of the product so that the patients can be offered chances to choose. In this study, taste, flavor, viscosity, color and other sensory factors were investigated, which can provide preliminary data necessary to develop optimized oral nutritional supplement for cancer patients. It is also meaningful since test products are powder form offering the patients chances to increase calorie intake by using different type of liquid to mix. Although the difference was not significant, the patient group preferred herb and fruit base over plain cereal base suggesting possibility of developing new products other than products with classic taste and flavor.
However, this study has a few limitations. First, while the sensory assessment on oral nutritional supplement was performed for powder type, the control supplement was a liquid type product. Since cancer patients are already used to the clear liquid type products, the trial manufactured products with a little granules are relatively new possibly affecting the sensory scores. Secondly, cancer patients included in this study received either radiation therapy or chemotherapy which may affect the palatability differently. Further large scale studies are necessary to compensate above limitations.
Conclusion
This study provides preliminary data on palatability of trial manufactured oral nutritional supplements. Cancer patients are shown to be more sensitive to sensory factors compared to the healthy controls. Patients are also used to a classic cereal-based clear liquid type product although they showed different preferences among other types of supplements. Further studies are necessary to develop next generation oral nutritional supplements containing other bioactive ingredients with higher palatability.




 XML Download
XML Download