

 ePub
ePub Citation
Citation Print
Print


| Korean J Sports Med. 2015 Dec;33(2):134-138. Korean. Published online December 07, 2015. https://doi.org/10.5763/kjsm.2015.33.2.134 | |
| Copyright © 2015 The Korean Society of Sports Medicine | |
|
Jung Hoei Ku,
Hyung Lae Cho, | |
| Department of Orthopaedic Surgery, Good Samsun Hospital, Busan, Korea. | |
| Received May 01, 2015; Revised June 03, 2015; Accepted June 04, 2015. | |
|
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by- | |
|
Abstract
| |
|
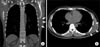
Scapulothoracic bursitis refers to inflammation of the bursae secondary to trauma or overuse owing to sports activities or work. It usually causes persistent pain and scapulothoracic crepitus by irritation of bursa but can be presented as painless mass around chest wall. We report a case of scapulothoracic bursitis in a baseball pitcher presenting as rapidly growing chest wall mass confused with a soft tissue tumor. Computed tomography and magnetic resonance imaging revealed as a well-demarcated cystic mass situated between the scapula and chest wall. Incisional drainage resulted in complete resolution of the mass within a couple of weeks. Scapulothoracic bursitis may be presented as painless huge mass in overhead sports athlete and one of the differential diagnoses of soft tissue tumor of the chest wall. |
|
Keywords: Scapulothracic bursitis; Chest wall mass; Incisional drainage; Baseball pitcher |
|
|
Figures
|
|

|
|

|

|
Notes
|
No potential conflict of interest relevant to this article was reported.
|
References
|
| 1. | Conduah AH, Baker CL 3rd, Baker CL Jr. Clinical management of scapulothoracic bursitis and the snapping scapula. Sports Health 2010;2:147–155. 
|
| 2. | Kuhn JE, Plancher KD, Hawkins RJ. Symptomatic scapulothoracic crepitus and bursitis. J Am Acad Orthop Surg 1998;6:267–273.
|
| 3. | Warth RJ, Spiegl UJ, Millett PJ. Scapulothoracic bursitis and snapping scapula syndrome: a critical review of current evidence. Am J Sports Med 2015;43:236–245.
|
| 4. | Sisto DJ, Jobe FW. The operative treatment of scapulothoracic bursitis in professional pitchers. Am J Sports Med 1986;14:192–194.
|
| 5. | Sohn KM, Moon DG, Sung CM, Choi PY, Park HB. Spontaneously regressed bilateral scapulothoracic bursitis. J Korean Orthop Assoc 2011;46:73–77.  
|
| 6. | Son SA, Lee DH, Lee YO, Lee SC, Kim KJ, Cho JY. Operative management in a patient with scapulothoracic bursitis. Korean J Thorac Cardiovasc Surg 2013;46:486–489.
|
| 7. | Williams GR Jr, Shakil M, Klimkiewicz J, Iannotti JP. Anatomy of the scapulothoracic articulation. Clin Orthop Relat Res 1999;(359):237–246.
|
| 8. | Higuchi T, Ogose A, Hotta T, et al. Clinical and imaging features of distended scapulothoracic bursitis: spontaneously regressed pseudotumoral lesion. J Comput Assist Tomogr 2004;28:223–228.
|
| 9. | Shackcloth MJ, Page RD. Scapular osteochondroma with reactive bursitis presenting as a chest wall tumour. Eur J Cardiothorac Surg 2000;18:495–496.
|
| 10. | Zembsch A, Schick S, Trattnig S, Walter J, Amann G, Ritschl P. Elastofibroma dorsi. Study of two cases and magnetic resonance imaging findings. Clin Orthop Relat Res 1999;(364):213–219.
|