

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Despite the progresses in health care, cardiovascular disease (CVD) remains the main cause of death worldwide [1]. Recently cardiovascular mortality is increasing in developing countries, mostly because of the influence of Western lifestyle, such as smoking, lack of physical activity and dietary habits. In Iran, as a developing country, CVDs are considered as the most leading causes of mortality [2] and there is a rising trend in its prevalence [3]. CVD occurred as a result of numerous risk factors such as, diabetes, obesity, high blood pressure, dyslipidemia and smoking [4]. Furthermore, dietary factors and life style patterns are more important in development of CVD [5]. Several investigations described the role of diet and nutrients in the expansion of metabolic diseases [6,7]. High intake of cholesterol and saturated fatty acids are associated with CVD mortality [8]. Despite the expectation that the dairy products (as a main source of cholesterol and saturated fat) may lead to development of CVD and metabolic diseases, the results of different studies are inconsistent. Although several studies have shown the hypercholesterolaemic effect of diets rich in dairy products, [9,10] others couldn't find any association between milk consumption and CVD [11]. Moreover, some studies showed positive effects on metabolic parameters as a result of consumption of milk products. These studies suggest that the intake of dairy products, as a good source of essential nutrients and high quality protein, may reduce the risk of heart disease [12,13]. Cheese as a high saturated fat dairy product, may increase cholesterol concentration and can be associated with higher CVD risk [14,15]; contrarily, cheese is a good source of calcium (Ca) that might reduce heart disease by influencing plasma lipid profiles [16], reduce blood pressure [17,18], and adiposity [19,20]. It has been claimed that the intake of fermented products like cheese is negatively associated with cholesterol concentration [21]. Previous investigations indicated that cheese may not have any unfavorable effect on lipid profiles [22] and that cheese may even have a cholesterol lowering effect [23]. A recent study reported that the frequency of consumption of cheese was negatively associated with serum TG and positively associated with serum HDL cholesterol [24]. In contrast, some studies found non-significant association between cheese consumption and heart disease [25,26]. Another study reported that cheese intake is positively associated with myocardial infarction [27]. Overall, due to inconsistent results, the effect of cheese on CVD risk factors has remained uncertain [28]. Cheese has been one of the most important dairy products in Iranian diet, especially for breakfast [29]. Furthermore, the studies on cheese and CVD risks were done in the western and developed countries with different lifestyle, and according to our knowledge there is no study from developing countries, particularly the Middle East region including Iran. Therefore, current study aimed to investigate the association between cheese intake and cardiovascular risk factors among Iranian people.
SUBJECTS AND METHODS
Participants
Information from the first phase of Isfahan Healthy Heart Program (IHHP) obtained for this cross-sectional study. Isfahan cardiovascular research institute and Isfahan provincial health office conducted the IHHP, which was a community-based program for cardiovascular prevention and control and healthy lifestyle promotion.
This study was completed in three provincial cities of Isfahan, Arak and Najafabad. Multistage cluster random sampling method was used for selecting individuals. More complete information about IHHP and sampling method is reported elsewhere [3,30]. Individuals who had dietary and anthropometric data, lipid profiles, plasma glucose and other biological measurements were included in this study. Individuals with history of chronic diseases or taking medications were excluded. Written informed consents were obtained from all participants who were 1,752 people (782 men and 970 women). The Ethics Committee of Isfahan University of Medical approved the study.
Measurements
Trained interviewers collected demographic, socio-economic data, medical and family history, smoking habits, as well as physical activity level using pretested questionnaire. Height was measured in bare foot by a wall fixed measuring tape and weight was measured in light clothing by calibrated scale. Body mass index (BMI) was calculated as weight in kilogram divided by height in meters squared. Waist circumference at the smallest circumference between lowest rib and the iliac was horizontally measured and hip circumference measurement was done at the greatest point of hip.
Dietary habits
To evaluate dietary intakes of participants a validated food frequency questionnaire (FFQ) that consists 49 items was used by expert technicians. The validity of this food frequency questionnaire was confirmed by Medical Education Development Center before being used [3]. The frequency and the portion size of consumption during the previous year for each food item were individually asked. Global dietary index (GDI), expressing diet quality, was produced by calculating the average of the mean of 29 frequency questions in seven categories.
Biochemical assessment
Blood samples were collected after overnight fasting. Fasting blood samples were frozen at -70℃ until being assessed at the central laboratory of Isfahan Cardiovascular Research Institute. Measurement of fasting plasma glucose (FPG), serum total cholesterol and TG levels was done by enzymatic colorimetric method. Measurement of HDL-C cholesterol was completed subsequent to sedimentation of non-HDL cholesterol by dextran sulphate-magnesium chloride. Friedewald equation [31] was used to calculate serum LDL-C cholesterol level. Enzyme immunoabsorbent and immunoassay was used to measure Apo A and Apo B.
Having three or more factor of FBS > 126 mg/dl or waist > 102 cm for men and > 85 cm for women or TG > 150 mg/dl or HLD < 40 mg/dl for men and < 50 mg/dl for women or systolic blood pressure > 130 mmHg and diastolic > 85 mmHg has been considered as metabolic syndrome. Having one disorder in lipid profiles (Cholesterol > 240 mg/dl, LDL-C > 160 mg/dl, HDL-C < 40 mg/dl for men and < 50 mg/dl for women, TG > 200 mg/dl) has been considered as dyslipidemia.
Statistical methods
Statistical analysis was done using SPSS 15 software. Student's t test was applied for comparing means of continuous variables between categories of cheese intake. To compare categorical variables Chi-square test was used. Logistic regression in different models was used to explore the associations between categories of cheese consumption and cardiovascular risk factors. First, we adjusted for age and sex, in second model further adjustment was done for dietary intakes and physical activity and then a last adjustment was done for BMI. In all models cheese intake < 7 times per week was considered as the reference.
RESULTS
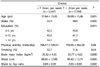
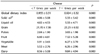
Characteristics of study participants by frequency of cheese consumption per week are presented in Table 1. Individuals who consumed more cheese (7 ≤ times per week) were older, mostly female, and tended to have higher BMI, waist and waist to hip ratio with different education status in comparison with people with lower cheese intake (< 7 times per week) group. No significant difference was found in physical activity and smoking between two groups. Table 2 indicates the cardiovascular risk factors of study participants by the frequency of cheese consumption. Higher consumption of cheese was associated with higher CRP, apolipoprotein A and HDL level but not with other cardiovascular risk factors including FBS, total cholesterol, LDL-C, TG and Apo B. Dietary intake of participants by frequency of cheese consumption are shown in Table 3. Higher consumption of cheese was positively associated with consumption of liquid and solid oil, grain, pulses, fruit, vegetable, meat and dairy products and negatively associated with Global Dietary Index. Crude and multivariate-adjusted odds ratio and 95% CI of cardiovascular risk factors in different groups of cheese intake are presented in Table 4. In crude model there was no difference between two groups but after adjustment for age and sex, low HDL level was negatively associated with cheese consumption (OR:0.89; 96% CI: 0.80-0.98). After control for other potential confounders such as dietary intakes and physical activity the association did not change. Further adjustment for BMI showed strong negative association between cheese intake with metabolic syndrome (OR:0.81; 96% CI: 0.71-0.94), low HDL level (OR:0.87; 96% CI: 0.79-0.96), and dyslipidemia (OR:0.88; 96%vCI: 0.79-0.98).
DISCUSSION
In the present cross-sectional study as part of Isfahan Healthy Heart Program (IHHP), higher consumption of cheese was associated with lower cardiovascular and metabolic risk factors, which shows the beneficial effect of cheese intake. These results are apparently in contrast with previous knowledge about blood lipids and dietary fat consumption as cheese considered as a main source of saturated fat among dairy products. It has been reported that milk and dairy products consumption were positively correlated with total cholesterol, LDL-C and HDL-C levels [9]. In contrary, the consumption of milk and its products has been demonstrated to be negatively associated with the prevalence of metabolic syndrome [32]. These results are reported from various populations that consume different kinds of milk products, and this difference may be one possible reason for this inconsistency. For example, high consumption of milk in Scandinavian countries led to high mortality of heart disease whereas, high consumption of cheese in France may be one of the reasons of low heart disease mortality [33].
It is supposed that the effect of fat intake from cheese on serum lipids might be different from what expected from fat content. In a previous study a positive relationship was found between the intake of milk and heart disease mortality, although cheese consumption was negatively but not significantly correlated [25]. Another study showed a positive association between dairy fat intake and coronary heart diseases but the study recommended that cheese could be an exception [34]. Other studies also reported that individuals in higher category of cheese consumption were not at higher risk of myocardial infarction [28], hypertriglyceridemia [33] or high LDL-C level [35] than people consuming lower amount of cheese. It has been reported that cheese consumption could even reduce LDL-C in comparison with equal fat from butter [36].
Our finding that higher consumption of cheese can be inversely associated with cardiovascular risk factors including metabolic syndrome, low HDL-C level and hyperlipidemia is in accordance with other earlier investigations on cheese consumption, which showed positive association between the intake of cheese and HDL-C level [24], and a negative association with total cholesterol levels [37] and metabolic syndrome [38,39]. Nevertheless, a prospective study found a positive association between cheese intake and cholesterol level, as well as IHD mortality [40]. Other studies reported a positive association between cheeses consumption and metabolic syndrome [41], cardiovascular risk factors [14] and myocardial infarction [27]. Different results among various studies might be depended on different population samples, lifestyles and study design [39].
A possible mechanism for beneficial effect of cheese consumption could be the effect of the high content of calcium in cheese. Previous studies showed that dietary calcium with fat generate calcium soup and increase the excretion of lipid in feces [42] and significantly reduce serum cholesterol and triglyceride levels [43]. The effect of fermented dairy products on cholesterol concentration could be another mechanism for cheese effect. It has been suggested that the bacteria existed in large intestine convert unabsorbed carbohydrates to short-chain fatty acids, which could modify cholesterol synthesis in the liver. Also, these bacteria could bind bile acids to cholesterol and increase its excretion and reduce bile acid recycling [21]. Furthermore, high protein content of cheese, hypothesized as another possible mechanism for its effect on cholesterol [36].
Several limitations are considered in the current study. First, this study was designed as a cross-sectional study that makes decision on causality impossible. Second, to assess dietary intake we used qualitative FFQ that may lead to misclassification and underestimation and just give a crude estimate of the cheese intake, although it has been claimed that single FFQ ranks participants on total intake [44]. Third, there might be some residual confounding affecting the association between cheese consumption and cardiovascular risk factors, such as other lifestyle, dietary factors and dietary supplementation that were not controlled in our analysis. Finally we didn't know about the fat content of consumed cheese. The fat content of cheese is an important factor influencing the result of different studies.
In conclusion, we found an inverse association between frequency of cheese intake and cardiovascular risk factors; however, further prospective studies are required to confirm the present results and to illustrate the probable mechanism.


 XML Download
XML Download