

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Kimchi is a salt fermented cabbage and is widely consumed in the traditional Korean diet. Kimchi is usually prepared by mixing salted cabbage with spice ingredients such as red pepper powder, garlic and ginger. It has been demonstrated that various unique microorganisms [1] and bioactive components present in kimchi show antioxidant capacity, an elevated immune response, and anti-cancer and anti-diabetic effects. For example, Lactobacillus plantarum, a major player in kimchi ripening, chelates metal ions [2] and potentiates the immune response [3]. Furthermore, components produced during the fermentation process show anti-cancer effects by inhibiting the Ras oncogene signaling pathway [4] and anti-atherosclerotic effects through lowering low density lipoprotein (LDL)-cholesterol oxidation [5]. Indeed, 3-(4'-hydroxyl-3',5'-dimethoxyphenyl) propionic acid, a component isolated from kimchi, was demonstrated to reduce LDL oxidation [6]. In addition, it was shown to reduce lesion size in the aortic sinus of apolipoprotein E knockout mice [7]. In a type2 diabetic animal model, ingestion of kimchi tends to lower fasting blood glucose levels and improves glucose tolerance [8]. Despite increasing awareness of the health benefits of kimchi, there is a concern about kimchi consumption due to its high salt contents. Most Koreans consume kimchi as part of their diet, and kimchi is a significant food source contributing to sodium intake in Koreans comprising 16-28% of the total daily sodium dose [9,10]. Since high sodium intake is positively associated with an increased incidence of hypertension, reducing the salt content in kimchi is generally considered to be health-beneficial. As such, reducing kimchi salt content has been a challenging task for food manufacturers because of the negative association between consumer acceptance and lower salt content in their products [11].
Hypertension is one of the risk factors for developing cardiovascular, cerebrovascular, and chronic renal diseases [12,13] and is prevalent worldwide [14,15]. Considering the high prevalence and long-term complications of hypertension causing cardiovascular mortality, non-pharmacological regimens are necessary to modulate hypertensive risks. Epidemiological and prospective studies have suggested that salt consumption is associated with an increased risk for hypertension [16,17]. Additionally, dietary restriction of sodium intake is effective to reduce blood pressure [17-19]. Therefore, regulating dietary sodium intake, which could be easily manipulated, could be a preventive measure to avoid the adverse pathological progress of hypertension.
In the present study, we tested whether consuming kimchi with low sodium content would lower the risks associated with hypertension compared to consuming kimchi with high sodium content without altering various other beneficial food constituents generated during the process of kimchi production. To address this question, we utilized spontaneously hypertensive rat (SHR), a well-studied experimental model of primary hypertension [20] and examined the effects of kimchi consumption on blood pressure and cardiac hypertrophy.
Materials and Methods
Animals
Eight-week-old male Wistar-Kyoto (WKY) rats and SHR were purchased from Harlan Laboratory (Barcelona, Spain). Rats were acclimated for 2 weeks before the experiment started. Eight of the 10 week old rats were randomly assigned into five different diet groups. One group was fed regular AIN-76 (Table 1) diet for 6 weeks and others with AIN-76 plus varying salt levels of kimchi for 6 weeks. Rats were housed in a temperature (18-24℃) and humidity (50-60%) controlled room. Animal body weight and diet consumption were measured weekly. WKY male rats were used as normotensive controls and received the control AIN-76 diet. SHRs were used as the hypertensive animal model and were divided into four groups: SHRs fed a control AIN-76 diet (SHR), SHRs fed the control diet supplemented with a low salted kimchi (SHR-L), those supplemented with a medium salted kimchi (SHR-M), or those supplemented with a high salted kimchi (SHR-H). All experimental procedures were approved by the Committee on Animal Experimentation and Ethics of Korea University.
Kimchi preparation
Low, medium, and high sodium kimchi were prepared for this study. The low sodium kimchi (Chongga, Daesang FNF Corp, Korea) contained 1.4% salt based on wet kimchi weight. The medium sodium kimchi (Chongga, Daesang FNF Corp, Korea) was 2.4% salt, which is commercially provided in Korean market, and the high sodium kimchi was 3.0% salt, which is generally prepared and served by Korean housewives [21]. The kimchi was freeze-dried and supplemented with the AIN 76 diet. The study was designed to provide 1 g wet weight of kimchi daily to each rat, which is the quantity equivalent to the amount of kimchi consumed by Korean healthy adults (200 g/day).
Blood pressure measurement
Systolic blood pressure (sBP) was measured with a tail cuff plethysmograph using a blood pressure measuring system (LE5002, Panlabs.l., Barcelona, Spain), as described previously [22]. Briefly, rats were placed in a warm chamber (37℃) for 5 min to rest and allowed to rest in a chamber. Occluding cuffs and pneumatic pulse transducers were placed on the tail. Five readings were obtained from each rat, and the average value of three readings, after removing the highest and lowest, was considered the sBP.
Tissue and blood sample collection
Rats were fasted overnight prior to sacrifice. The heart was excised and weighed, and then the left ventricle (LV) was excised and weighed. Blood samples were collected into a polystyrene tube via the abdominal inferior vena cava. Serum was obtained by centrifugation at 3,000 rpm for 30 minutes at 4℃ and stored in a freezer at -80℃ before analysis.
Cardiac histology
LVs were fixed in 10% formalin and stored in 10% phosphate buffered formalin. LV tissues were embedded in paraffin blocks and sectioned (5 µm). Tissue sections were subjected to periodic acid-Schiff staining and analyzed by microscopy (Olympus BX41, Olympus America Inc., Center Valley, PA, USA) at a magnification of 400×. The diameters of at least 50 myocytes with longitudinal orientation were determined using the analySIS-getIT program (Olympus Soft Imaging Solution). The diameter was obtained by taking the distance passing through the center of the nucleus to the longest part of the myocyte.
Serum biochemical analysis and aldosterone measurement by enzyme-linked immunosorbant assay (ELISA)
Serum levels of blood urea nitrogen (BUN), creatinine (Cr), glutamate oxalacetate transaminase (GOT) and glutamate pyruvate transaminase (GPT) as well as potassium and sodium levels were measured with an autoanalyzer (Express Plus, Bayer, Pittsburgh, PA, USA). ELISA was performed using a rodent aldosterone ELISA Test kit according to manufacturer's instruction (Endocrine technologies, CA, USA). Data represent averages of two independent experiments.
Statistical analysis
Statistical analysis was performed using SPSS version 11.0 for Windows (Statistical Package for the Social Science, SPSS Ins., Chicago, IL, USA). Results are presented as means ± SE, and the differences among the experimental groups were analyzed using Student t-test or one-way analysis of variance (ANOVA) followed by Duncan's multiple range test. ANOVA for repeated measures from general linear model (GLM) was also performed to examine whether the change of blood pressure during the observational period (6 weeks) were different among the groups (diet type). A P < 0.05 was considered significant.
Results
Food intake and body weight gain
Average initial body weight in the WKY group was significantly lower than that in the SHR groups (WKY, 217.9 ± 3.4 g; SHR 260.5 ± 4.1 g; SHR-L, 262.4 ± 5.0 g; SHR-M, 260.0 ± 3.0 g; and SHR-H, 266.5 ± 4.2 g). After 6 weeks on the experimental diets, all rat groups had similar body weights ranging from 291.2 ± 6.6 g to 320.1 ± 8.2 g. Cumulative body weight gain was less in the SHR groups compared to that in the WKY group. However, this change was not due to lower food intake in the SHR groups, because the sum daily food intake was slightly higher in the SHR groups (SHR, 803.6 ± 25.5 g; SHR-L, 750.7 ± 12.7 g; SHR-M, 744.1 ± 5.4 g; and SHR-H, 765.6 ± 9.2 g) than that in the WKY (694.8 ± 19.9 g) group. The overall food efficiency ratio (FER) was higher in the WKY group compared with that in the SHR groups (Table 2). In contrast, no differences in body weight gain, food intake, or FER were observed between the kimchi-supplemented SHR groups (SHR-L, SHR-M, and SHR-H) and the control SHR group (Table 2).
Systolic blood pressure
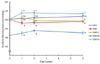
All SHR groups displayed significantly higher sBP levels than those in the WKY group over the course of the experiment (Fig. 1). A significant diet effect on blood pressure was observed during the observational period (P < 0.001). At 1 week of the diet treatments, the SHR-H group began to show increases in sBP, and levels were significantly higher than those in the SHRs that were not supplemented with kimchi (SHR-H, 223.4 ± 9.9 mmHg and SHR, 189.2 ± 6.2 mmHg). After 2 weeks of kimchi supplementation, the sBPs of the SHR-L (200.1 ± 7.6 mmHg) group were significantly lower than those of the SHR-H (224.0 ± 7.3 mmHg) group. This statistically significant difference in sBP between SHR-L and SHR-H continued until the end of experimental period (at 6 weeks, SHR-L, 199.0 ± 7.1 mmHg and SHR-H, 221.4 ± 4.8 mmHg). After 6 weeks of kimchi supplementation, sBP levels in the SHR-L group were similar to those in the SHR groups that were not supplemented with kimchi (SHR, 194.7 ± 8.3 mmHg).
Cardiac and LV mass
After 6 weeks of the diets, clear increases were observed in cardiac mass, the cardiac index (mg of cardiac mass/g of body weight), LV mass, and the LV index (mg of LV/g of heart) in all SHR groups compared to those in the WKY group (P < 0.001) (Table 2). However, kimchi supplementation among the SHR groups did not elicit any changes in these parameters. These results indicate that the SHR group showed a tendency for cardiac and LV hypertrophy, whereas kimchi supplementation, regardless of sodium content, did not trigger a further disturbance of heart function in the SHR groups.
Cardiomyocyte size
Cardiomyocyte size was substantially larger in all SHR groups than that in the WKY group (Fig. 2). However, kimchi supplementation did not significantly alter the size of cardiomyocytes in the SHR groups (SHR, 17.3 ± 0.3 µm; SHR-L, 17.8 ± 0.5 µm; SHR-M, 16.0 ± 0.4 µm; and SHR-H, 17.5 ± 0.5 µm).
Serum levels of biochemical parameters and aldosterone
Serum levels of BUN, GOT, and GPT were higher in the SHR groups than those in the WKY group (P < 0.001) (Table 3). The SHR-H group showed a tendency for higher BUN levels than those in the SHR-L group, but the difference was not significant. Serum concentrations of sodium, potassium, and Cr were not different among the groups (Table 3). As shown in Fig. 3, serum levels of aldosterone in the SHR groups were higher than those in the WKY group, and those in the SHR-L group were lower than those in the SHR groups (Fig. 3).
Discussion
While there is an increasing interest in health benefits originating from kimchi, there is also a concern regarding sodium intake accompanied by kimchi consumption. Here, we investigated the possible effects of kimchi consumption on hypertension and/or cardiac function by varying salt levels in kimchi. Previous findings suggesting that sodium intake modulates blood pressure [16,23] were re-emphasized in a relatively recent study using a genetically homogeneous population [24]. In that epidemiological study, normotensive subjects with different degrees of sodium intake showed different blood pressure levels, suggesting a cause-and-effect relationship between sodium intake and blood pressure [24]. Additionally, dietary approaches that use decreased sodium content successfully lower blood pressure in human subjects who are either normotensive or hypertensive, indicating a direct association between sodium intake and blood pressure [17,18]. Therefore, kimchi as a salted traditional Korean dish might contribute to an increase in blood pressure.
Cardiac hypertrophy is one of the adverse changes caused by hypertension. It is considered to be a severe form of hypertensive vascular disease because of its continuous progression to cardiac failure even after treatment for hypertension [25]. Furthermore, a prolonged hypertensive condition manifested by increased blood pressure can damage tissue structures and cause functional consequences such as cardiac failure [25,26] and kidney disease [27]. Thus, the hypertrophic status of cardiac tissues can be used as an indicator of the degree of hypertension severity. In addition, many studies have corroborated that salt loading enlarges cardiac myocytes and induces fibrosis in the heart and kidneys apart from its hemodynamic effect [28-30]. Gu et al. [31] demonstrated that sodium directly regulates hypertrophic growth of cardiac myoblasts and vascular smooth muscle cells. Taken together, salt loading can be a strong inducer of cardiac hypertrophy and fibrosis, which are suggested to be a mechanism responsible for a progressively damaged heart condition [28,29,32]. In particular, LV hypertrophy, which is directly associated with salt intake, is an independent determinant of cardiovascular morbidity and mortality in patients with hypertension [33,34]. Salt loading increases LV mass in non-spontaneously hypertensive WKY rats without inducing noticeable effects on arterial pressure [28,30,32]. Therefore, LV mass could be an effective way to detect cardiac hypertrophy severity that might be induced by kimchi salt content. Because of the close link among salt consumption, hypertension, and cardiac hypertrophy, we investigated whether kimchi, a salted and fermented Korean cabbage dish, could adversely affect blood pressure and/or cardiac hypertrophy. We also searched for the possibility of using low sodium kimchi to lessen sodium-related adverse effects on hypertension and/or cardiac hypertrophy, which was measured by blood pressure, LV mass, and cardiomyocyte size, respectively. The amount of kimchi provided per day to rats was equivalent to an average daily dose observed in the typical Korean diet [21]. Throughout the experimental period, the SHR groups showed elevated sBPs compared to those in normotensive WKY rats, indicating that the SHR rat is a good model to test the effect of high sodium kimchi under the hypertensive condition. The high sodium kimchi containing 3.0% salt by wet weight elicited a modest but significant increase in sBP in SHRs, which develop hypertension spontaneously. Based on these findings, frequent intake of high sodium kimchi may be not advisable for those who have a high risk for hypertension. At the same time, the blood pressure-elevating effects of high sodium kimchi may be harmful to those who are susceptible to hypertension. In a previous study, WKY rats, in which blood pressure is within the normal range, showed modest changes in blood pressure and LV mass only when they were fed a diet loaded with extremely high salt (8% in diet) [32,35]. Therefore, even if we did not identify the effect of high sodium kimchi supplementation on blood pressure in the normotensive WKY group, it is presumed that a high sodium kimchi diet was less likely to affect blood pressure in people whose blood pressure is within the normal range. Interestingly, the low sodium kimchi, containing 1.4% of salt by wet weight, did not further raise sBP even in a hypertensive state, as shown in the SHR groups. This finding suggests that the salt content found in low sodium kimchi is not high enough to exceed a threshold level to elicit an increase in blood pressure and thereby allow the body to retain its ability to maintain constant blood pressure level. Therefore, lowering salt content in kimchi appears to be effective to avoid an elevation in blood pressure under hypertensive conditions.
While the exact mechanism of the inhibitory effect of low sodium containing kimchi on the elevation in blood pressure is unclear, the rennin-angiotensin-aldosterone system (RAAS) might be involved. RAAS plays an essential role in the maintenance of volume homeostasis and regulation of blood pressure [36]. High salt increases blood pressure through increased RAAS activation, leading to an increase in cardiac output and vascular resistance [37]. Thus, the extent of changes in blood pressure is buffered by regulation of the RAAS. Angiotensin converting enzyme inhibitors are often used to effectively lower blood pressure [38]. In the present study, higher levels of serum aldosterone were observed in the SHR groups when compared with those in the WKY group, suggesting that an increase in blood aldosterone may be one of the mechanisms to raise blood pressure in SHRs. Interestingly, serum aldosterone levels were lower in the low sodium kimchi group even if their blood pressure levels were similar to those of SHRs. Furthermore, the medium and high sodium kimchi groups demonstrated that their aldosterone levels were similar to the SHRs despite that their blood pressure was much higher than that of the SHRs. Taken together, eating kimchi appears to be effective for either reducing or maintaining blood aldosterone levels to control blood pressure. However, the possible aldosterone lowering effect of kimchi was not reflected in the blood pressure levels of all kimchi groups. Thus, overall aldosterone-modulating effects by kimchi might not be strong enough to lower blood pressure in SHRs which may experience various blood pressure-increasing mechanisms. Clearly, low sodium kimchi did not further elevate blood pressure in the SHRs unlike medium and high sodium kimchi. Therefore, low sodium kimchi could be an alternative way to maintain the beneficial effects of kimchi without exerting harmful effects on blood pressure.
We examined cardiomyocyte size and the LV index to further demonstrate the effects of sodium derived from kimchi on hypertension. Blood pressure is closely associated with cardiac hypertrophy, which is one of the major risk factors underlying cardiovascular morbidity and mortality [39]. In the present study, the SHRs showed a higher LV mass and a higher LV index than those of the WKY, suggesting that the SHR is in a relative cardiac hypertrophic state compared to that of the WKY. Regardless of sodium content, kimchi supplementation in the SHRs did not further increase cardiac and LV mass or cardiac myocyte size after 6 weeks of the diets. Therefore, salt content ranging from 1.4% to 3% of total kimchi wet weight did not seem to exert changes in cardiac mass and functions, at least during 6 weeks of kimchi supplementation. It is of interest that the high sodium kimchi supplementation did not further enlarge cardiomyocytes, although its high sodium content significantly elevated BP under a hypertensive state. This raises the possibility that certain bioactive components contained in kimchi might display beneficial effects on heart function, which was not experimentally shown in this study.
Besides the heart we examined the function of other organs such as the kidneys and liver following kimchi supplementation using general biochemical parameters to investigate if there was any adverse effects of kimchi. The kidneys are another organ targeted by hypertension and play an important role in the pathogenesis of hypertension [40]. In our study, BUN and Cr were used as biochemical indicators of short and long-term kidney function in SHRs and WKYs. Relatively elevated BUN levels were observed in all SHR groups compared to those in the WKY group, indicating an SHR-specific difference in basal BUN levels, which was also shown in another study [41]. However, Cr levels in SHRs did not appear to be affected by primary hypertension, as they had similar levels of Cr to those in the WKY group. Kimchi supplementation did not affect either BUN or Cr levels in the SHR groups, suggesting that kimchi may not influence kidney function in this setting. GOT and GPT levels are indicators of general liver function. In line with previous findings [41], we observed higher levels of GOT and GPT in all SHR groups relative to those in the WKY group at the end of experiment when the animals were 16-weeks-old, but these changes were not further affected by kimchi supplementation. Therefore, we conclude that kimchi is less likely to have a negative effect on liver function. In contrast, cations such as sodium and potassium in the serum were equally maintained in both the SHRs and WKYs, indicating that sodium and potassium levels were not affected by the initial changes occurring during the development of primary hypertension in this setting.
In summary, supplementation with low sodium kimchi did not influence blood pressure, cardiomyocyte size, or LV mass in SHRs, whereas supplementation with high sodium kimchi further raised blood pressure. Our findings show the significance of a low sodium kimchi diet for maintaining blood pressure when compared to high sodium kimchi under a hypertensive condition. Considering the numerous health benefits of consuming kimchi, as evidenced by in vivo and in vitro studies [20,22,24-27], low sodium kimchi could be an alternative option for those who may need to restrict sodium intake because of hypertension or related disease conditions while maintaining its associated beneficial health effects.





 XML Download
XML Download