

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Dehydration can develop when the body fluid losses exceed fluid intake, and it often occurs during exercise, heat stress, restricted fluid intake, or any combination of these. Marginal dehydration (loss of > 2% body weight) can compromise aerobic exercise performance, particularly in hot weather conditions, and may disturb fluid and electrolyte balance [1-4]. Thus, maintaining a hydrated state prior to physical activity is important not only for optimizing performance but for ensuring health and safety. Further, when an individual becomes dehydrated during exercise, an adequate fluid supply is necessary to maintain fluid balance and physiological homeostasis.
Rehydration should be readily performed after any bout of intense exercise. In some cases, however, an individual may start exercise already in a dehydrated state, such as when an opportunity for full rehydration is not available [5]. Thus, many studies have focused on optimal methods of maintaining a hydrated state before, during, and after a bout of exercise [2-4,6,7]. Specifically, rehydration is a function of the volume of fluid consumption relative to the volume of fluid losses following dehydration. The goal of rehydration is full replacement of any fluid and electrolyte deficits resulting from a previous event [1,2,4]. Successful rehydration can be achieved by applying appropriate rehydration methods using an adequate supply of fluids. Such a method depends on the speed with which rehydration must be accomplished as well as the magnitudes of the fluid and electrolyte deficits.
In this regard, some guidelines for rehydration have been suggested. As an example, forced rehydration in which subjects are instructed to drink a specific amount of fluids is common. It was suggested that 150% of the volume of fluids lost should be consumed in order to properly compensate for fluid loss due to urine production during rehydration [3,6,8]. Consumption of meals and snacks containing sodium along with a sufficient volume of water is also recommended as a hydration method [9], as restoration of body fluids and body weight is more rapid when using rehydration solutions containing electrolytes as compared to plain water [10,11]. Favorable palatability is also recommended to promote voluntary intake of fluids. Fluid palatability is influenced by several factors, including flavoring, electrolyte contents, and fluid temperature [12-15]. The preferred beverage temperature is often between 15 and 21℃. However, the overall rating of palatability seems to depend on individual preference and culture [16].
Nevertheless, complete rehydration after fluid and electrolyte loss is usually not achieved voluntarily. For instance, athletes often fail to completely replace body fluid losses during the first few hours of recovery, despite readily free access to various hydration beverages [1,2,17]. To promote voluntary drinking following exercise, the influence of water temperature has been investigated. Athletes have been shown to prefer and drink greater volumes of cool water compared to water at or above ambient temperature [13-15]. Ingestion of cool or cold water during and after exercise as also acts a heat sink and lowers one's core temperature [18].
Previously, carbohydrate-electrolyte solutions and cool drinks were shown to be favorable for rehydration, but combination of these two during voluntary drinking has not been examined. Although rehydration after exercise-induced dehydration has been well investigated, the effects of beverage temperature and composition on fluid consumption and weight retention upon voluntary dinking have not been thoroughly examined. Thus, this study examined the effects of temperature and composition of beverages on fluid intake and weight regain following exercise-induced dehydration.
Subjects and Methods
Subjects
Eight healthy collegiate men voluntarily participated in this study. Subjects were informed of the experimental procedures as well as any possible risks involved before signing an informed consent form approved by the Institutional Review Board. They reported no relevant medical history or diseases associated with exercise and heat exposure, and none of the subjects took medication at the time of the experiment. Their physical characteristics are presented in Table 1.
Study design
Subjects participated in four experimental trials: two types of beverages at two different temperatures. In each trial, subjects intentionally lost 2% of their initial body weight while exercising at elevated temperature. Following this, the subjects underwent a 90-min recovery period during which they consumed one of four beverages: 10℃ water (10W), 10℃ sports drink (10S), 26℃ water (26W), or 26℃ sports drink (26S) ad libitum. Trials were begun at 08:00-10:00 hours and separated by at least 7 days.
Experimental procedures
Subjects were instructed to abstain from exhaustive exercise, alcohol, and caffeine for at least 24 hours before each trial and encouraged to consume abundant fluids to ensure a normal body weight and hydration state. After 10 hours of overnight fasting, they reported to the laboratory in the morning and were given a 500 ml bottle of water to consume. Two hours later, subjects were instructed to completely void their bladders so that urine samples could be collected. After naked body weights were taken, a rectal probe (T-type thermocouple) was inserted 10 cm beyond the anal sphincter. Subjects also wore an electrical heart rate (HR) monitor (S610i, Polar, Italy) on their chests. Subjects wore lightweight running shorts, socks, and running shoes, and the weight of the exercise apparel was premeasured. Subjects sat quietly at least 20 min in order to obtain a stable condition in which baseline HR, rectal temperature (Tre), blood pressure (BP), and blood sample were measured.
Subjects next entered an environmental chamber maintained at 36-38℃ and 50% of relative humidity. Subjects were then instructed to run on a treadmill at any speed they selected. Subjects were informed of the purpose of the exercise at elevated temperature as well as the target weight reduction. Subjects alternatively ran and weighed themselves until target body weight reduction was met. During exercise, HR, Tre, and running speed were continuously monitored and recorded. No fluid consumption was allowed in the chamber. Once the target weight reduction was achieved, the subjects were instructed to leave the chamber, after which blood and urine samples were collected.
During each recovery period at ambient air temperature, subjects drank one of four beverages (10W, 10S, 26W, or 26S) ad libitum. Initially, 1,500 ml of beverage was provided, and additional beverage was allowed upon request. Investigators did not inform the types of beverage until the recovery period of each session. The volumes of beverage consumed as well as naked body weights were measured after 30, 60, and 90 min of recovery. No verbal encouragement or feedback regarding beverage consumption was given to subjects during the recovery period. Subjects were allowed to void their bladders at any time, but otherwise they sat quietly. The sports drink was a commercially available carbohydrate- and electrolyte-containing fluid (Gatorade, Korea).
Measurements and calculations
Body composition was evaluated by the bioelectrical impedance method (Inbody 520, Biospace, Korea). Exercise duration in each session was recorded. HR and Tre at the end of the running period and during recovery were monitored and recorded. Tre was measured and recorded on a data logger (Hydra series II, Fluke, USA). Body weight was measured to the nearest 0.1 kg (150A, CAS, Korea). BP was measured by brachial auscultation (sphygomomanometry).
A 5 ml venous blood sample was drawn into an EDTA-treated test tube. Whole blood was immediately analyzed for contents of hemoglobin (Hb 201+, HemoCue, Sweden), hematocrit (I-Smart, Isense, Korea), and blood electrolytes, including sodium (Na+), potassium (K+), and chloride (Cl+) (I-Smart, ISense, Korea). Plasma was analyzed for osmolality (Posm) using the freezing point depression method (model 210, Fiske Micro-Osmometer, USA). All measurements were made in duplicate. Urine samples were analyzed for volume and urine specific gravity (USG; UG-1, Atago, USA). Volumes of beverage and urine were measured by a measuring beaker.
The percent changes in plasma volume (%PV) from baseline were calculated from hematocrit and hemoglobin [19]. Mean arterial pressure (MAP) was calculated as one-third the pulse pressure (systolic minus diastolic pressure) plus the diastolic pressure. Total volume consumption was calculated by adding the volumes of all of the consumed fluids. Weight retention was calculated from the body weight changes between post-exercise and end of recovery, corrected for the volumes of fluid consumed and urine excreted. Volume loss was calculated as the total volume of beverage consumed minus weight retention.
Statistical analysis
All measurements were expressed as a mean or standard deviation. To compare singular data between the four conditions, one-way ANOVA was used. Two (beverage temperatures) by two (beverage types) ANOVA with repeated measurements was utilized when appropriate. Window version 12.0 SPSS was used. When a significant interaction was found, post hoc test of Scheffe was employed. Statistical significance was considered when P < 0.05.
Results
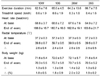
The exercise conditions, inducing body weight reduction, are shown in Table 2. Subjects ran a distance ranging from 8.9-9.3 km to achieve the target weight reduction. No differences between HR, Tre, and body weight changes were observed. During voluntary dehydration, Tre increased by 2.4-2.6℃ and body weight was reduced 1.8-2.0% from baseline.
Table 3 shows the BP, volume parameters, and blood electrolyte responses during the experiments. MAP and USG were not different between the conditions and were maintained within a normal range during the trials. After weight reduction, %PV decreased under all conditions, and it did not return to the baseline after the recovery period (P < 0.001). No group differences were found in %PV. No group differences were noticed in Posm, Na+, K+, and Cl-.
The recovery period at 30-min intervals as well as total beverage consumption are represented in Fig. 1. During the first 30 min of recovery, subjects drank about 948 ml of 10S. This volume was higher than those of 10W (681 ml), 26W (693 ml), and 26S (699 ml), but it was not statistically significant (P = 0.179). When total beverage consumption volumes were compared, no statistical differences were found between the conditions (P = 0.113). The total amount consumed was highest for 10S (1505 ± 614 ml) compared to the other drinks (1164 ± 388 for 10W, 948 ± 297 for 26W, and 1239 ± 401 ml for 26S).
Weight retention and volume loss during the experiment are shown in Fig. 2. Weight retention in those who drank 10S was greater in those who drank 10W and 26W (P < 0.005). Volume loss was lower in those who drank 10S, but it was not significantly different.
Discussion
This study compared differences in weight retention and fluid balance between subjects that consumed various fluids at two different temperatures following exercise-induced dehydration. In this study, we found that weight retention was greatest in those subjects that consumed the cool carbohydrate-electrolyte beverage. In general, in terms of amount consumed, cool temperature and carbohydrate-electrolyte fluid were preferred compared to warmer temperature and plain water, respectively.
These findings support data from previous investigations. Engell and Hirsh [16] previously reported that the preferred water temperature for rehydration is between 15-21℃. In another study, subjects that exercised on a treadmill for 6 hours at elevated temperature consumed 15℃ fluids more than 40℃ fluids, and flavored beverage was the most preferred [7,15,20]. Maximal fluid intake was previously shown to be accomplished with 15℃ water, and any colder or warmer temperature resulted in lower overall consumption [13]. On the other hand, Jung et al. [21] reported no difference in fluid consumption between chilled water and five ambient temperature beverages during heat exposure. Thus, in general, it is possible that beverage temperature may affect palatability, which in turn may impact the total amount of fluid consumed during voluntary drinking. One concern is the effect of temperature on the rate of gastric emptying. However, several studies have reported no significant differences in gastric emptying rate and volume using a cold temperature fluid [22,23].
The flavor of the drink is also associated with the amount of fluid intake [24-27]. Maughan and Leiper [25] examined the effect of palatability of the rehydration fluid. The investigators provided beverages with four different solute contents after dehydration, and subjects were allowed to drink ad libitum. After 2 hours of rehydration, subjects drank a greater volume of sports drink and juice mixture than aerated water. This result indicated that subjects the preferred glucose-electrolyte beverages over non-palatable water. Clapp and colleagues [24] also reported significantly greater fluid consumption of the carbohydrate-electrolyte beverages as compared with colored water when different beverages were provided for consumption ad libitum during 4 hours of intermittent exercise in a hot environment. Beridot-Therond et al. [28] also observed slightly higher consumption of sweetened beverages as compared to mineral water in dehydrated subjects. In addition, consumption of flavored beverages maintained at ambient temperature was shown to be greater than that of ambient temperature water [21]. Animal studies have suggested that altering the sensorial properties of a beverage by adding a sweetener can increase the volume of consumption through increased palatability [29]. Further, a sweet taste may stimulate the hunger sensation in humans [30-32]. Thus, a cool flavored beverage containing both carbohydrates and electrolytes can stimulate palatability, thereby inducing greater voluntary fluid consumption after dehydration.
There are many reports that have compared the effects of both water and solute-containing beverages on body fluid restoration [33,34]. It has been well recognized that water ingestion results in prompt dieresis, even during hypohydration, and prevents a return to a normal hydration state [24,35,36]. Maughan and Leiper [33] demonstrated that there is a strong relationship between the sodium content of an ingested fluid and the rate of fluid restoration. In one study, the volume of urine excretion was smaller upon consumption of electrolyte-containing beverages as compared with electrolyte-free beverages [37]. It has also been shown that there is plasma volume is recovered faster using a higher sodium content beverage as compared to a lower one [33]. The present study also demonstrated higher volume retention as indicated by body weight regain using the cold sports drink. When subjects were allowed to drink plain water regardless of temperature, fluid volume retention was low.
In the present study, subjects did not recover their baseline body weights upon voluntary drinking under any of the conditions. Previous studies have reported that a 1.5-fold volume of fluid ingestion per kilogram of body weight loss is necessary to achieve proper rehydration over a short period of time [3,8,38]. This is due to volume expansion and subsequent increased urine production. In the present study, we observed higher volume consumption only with the cool carbohydrate-electrolyte beverage (1.3 kg weight loss during exercise vs. 1.5 L of beverage intake over 90 min). Further, even under these conditions, the volume of fluid consumed was not anywhere near 1.5-fold the volume of fluid lost. It should be noted that the subjects drank ad libitum. Previous studies also reported that voluntary fluid consumption is not sufficient to replace all fluid losses following dehydration [35,39]. In practical terms, drinking beverages to recover from fluid loss might not be feasible under the circumstance of voluntary drinking, especially when the temperature and composition of the beverage are not optimal to the individual. In fact, many studies reported that subjects who drank water equivalent to 100% of the volume of body fluids lost expressed discomfort during ingestion [38].
Under the conditions of this study, we did not observe any marginal differences in blood solute concentration. Further, plasma volume did not fully recover to baseline even after 90 min under all conditions. It has been suggested that the composition of the rehydration beverage should optimally contain 5-10% carbohydrates, 20-30 meq/L of sodium, and 2-5 meq/L of potassium [40]. Here, sodium and potassium ions replace electrolyte losses due to sweating, and sodium further prevents excessive urine production [6,38]. During recovery, sodium consumption in fluids not only retains ingested fluids but also helps to stimulate thirst sensation. Under normal circumstances, the consumption of a carbohydrate-electrolyte solution maintains the sodium concentration in the blood as compared to consumption of plain water [41]. Thus, plain water is not considered to be the optimal solution for replacing water lost during exercise [39,42]. In the present study, under all conditions, both plasma volume and osmolality deviated from baseline after 90 min of recovery. This suggests that both volume and blood tonicity may contribute to the stimulation of thirst sensation [17,43,44]. Ironically, a lesser volume of fluids taken in during recovery had the effect of maintaining thirst when drinking water only. One explanation is that there was lower amount of water consumed versus that lost. In addition, hyponatremia, defined as when the blood sodium level is less than 135 mmol/L [4], induced by excessive drinking of water following 2% body weight reduction was not observed in this study.
In this study, subjects drank greater amounts of cold carbohydrate-electrolyte beverage than plain water and moderate temperature beverage, resulting in greater weight retention. This suggests that cold carbohydrate-electrolyte beverage is favorable for rehydration during recovery when voluntary drinking is applied.




 XML Download
XML Download