

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
For children, protein and calcium, as well as minerals such as magnesium, manganese, copper and zinc are necessary for proper growth and development. Of these elements, manganese (Mn) is known to be an essential nutrient for skeletal structure formation as well as in the amino acid, cholesterol and carbohydrate metabolisms [1]. Mn also plays a critical role in the function of various enzymes, including arginase and Mn superoxide dismutase.
In animal experiments, Mn deficiency has been shown to bring about impaired insulin production, changes in lipoprotein metabolism, an impaired oxidant defense system, and precocious pubertal development [2-4]. Most significantly, if the deficiency occurs during early development, there can be pronounced skeletal abnormalities and irreversible ataxia [1]. It was also found that Mn supplementation improved spine bone mineral density in growing rats via increasing osteoblast activity [5]. Therefore, its function with regard to nutrition for appropriate growth and development during childhood is very important. It has however been reported that excessive Mn intake causes neurotoxicity and increases Mn concentration in the blood [1]. It has also been reported that for adults of aged 50 or more, drinking water with elevated Mn levels is related to a higher prevalence of neurological signs [6]. There was also a study showing that children between 6 and 12 years of age showed lower cognitive performance when they had a high Mn concentration in their hair [7]. Despite this, adequate Mn intake is necessary for children in their growth stage, and can be obtained through cereals, vegetables and legumes. The Mn content is also high in nuts, seeds, fish, and green tea. Korean foods typically include rice as the staple with vegetables and pulses as side dishes, which could suggest that there is a lower risk of Mn deficiency in Korea than in other western dietary styles. However, intake of food from animal sources is increasing in Korea due to a growing preference for western food. As a result, studies of Mn intake and identification of its food sources are required.
In Korea, the dietary reference intakes (DRIs) for Mn are set as the adequate intake (AI) for all age groups. The tolerable upper intake level (UL) is set for age groups older than 1 year of age. The AI and UL of Mn were set for the first time in 2005 by the Korean DRIs. There is still insufficient data to set a general estimated average requirement (EAR) and a recommended nutrient intake (RNI) for Mn. Therefore, at present Mn intake recommendations are presented as the AIs for different age groups. Currently, the AI of Mn for 12 to 14 year olds is set at 4.0 mg/day for boys and 3.5 mg/day for girls. For both sexes in this age range, the UL of Mn is 7.0 mg/day. Kim and colleagues conducted a study of healthy 354 Korean adults above the age of 20 in which it was observed that the average Mn intake per day was 4.5 mg, which represents 140.9% of the adequate intake [8].
A study in Japan that examined 25 children aged between 3 and 6 years showed that their 1.56 mg/day Mn intake was close to the recommended value [9]. In another study from Poland which examined 4 to 16 year olds it was reported the average Mn intake was at 0.067 mg/kg B.W. per day [10]. However, there have been no studies on the Mn intake of Korean children. Considering the importance of Mn in bone health, metabolism and normal growth, it is necessary to correct this research lacuna and accurately assess the Mn intake of Korean children during their growth period. Therefore, the goal of this study is to evaluate the food sources of Mn and Mn intake of Korean children during their growth stage.
Subjects and Methods
Subjects
The subjects in this survey comprised 257 children aged 11 to 12 years (boys 123; girls 134) in Seoul, Korea. After explaining the study objective and details of this research project, subjects gave their informed consent to participate. Anthropometric measurements and dietary surveys were conducted on the survey subjects. Data were collected between July and August 2008.
Anthropometric measurements
Height was measured using a height-measuring instrument on which the individual subject stood without shoes. Weight was measured using a calibrated scale, with the subject dressed in light clothing. Their body mass index was calculated as their body weight in kilograms divided by their height in meters squared. Using age, sex and Body Mass Index (BMI) as the standard measurements, subjects who were between the 85th and 95th percentile were classified as overweight, whereas those in the 95th percentile or above were classified as obese [11].
Dietary intake survey
A dietary intake survey was conducted using a three-day dietary record method. Subjects were asked to keep a nonconsecutive three-day dietary record that included one weekend day or holiday. Subjects were asked to record the times at which they consumed food and the type and amounts of all foods and beverages being consumed. Subjects were asked to provide detailed descriptions of each food item, including the proportions and the product name. Results of the dietary intake survey were analyzed in terms of nutrient intake using the Can-Pro 3.0 program (Korean Nutrition Society). Manganese consumption was calculated through the use of the manganese content database from the list of Koreans' 366 most frequently consumed foods [12] and through the food composition table created by the National Rural Living Science Institute, Korea [13]. After calculating the intake of Mn per individual, the status of the intake was calculated in relation to the Dietary Reference Intakes for Koreans [14], and the Mn intake per food group, as classified with Can-Pro 3.0 program (Korean Nutrition Society), was also analyzed.
Statistical analysis
Mean and standard deviation values were calculated using the SAS program (version 9.1, SAS Institute, Cary, NC, USA). To assess the differences between boys and girls, unpaired t-test was used for continuous variables, and χ2-test was used for discontinuous variables. Statistical significance was evaluated at the level of P < 0.05.
Results
General characteristics of the subjects
The general characteristics of the subjects are shown in Table 1. The average age, height, weight and BMI of the subjects were 11.9 years, 154.7 cm, 46.1 kg, and 19.2 kg/m2, respectively. There was no significant difference in height between boys and girls, but the BMI values of the boys were higher than those of the girls (P < 0.001).
Nutrient intakes of the subjects
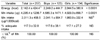
The dietary energy and Mn intakes of the subjects are shown in Table 2. Boys had an average energy consumption of 2,249.2 kcal per day, compared to 2,044.5 kcal for girls (P < 0.001). In boys the daily Mn intake was 4,585.3 µg, and in girls this was 4,029.3 µg (P < 0.001). Boys and girls had 2,041.1 µg and 1,983.9 µg Mn intake per 1,000 kcal of consumed energy, respectively, which are not significantly different values. Boys reached 117.6% and girls 117.1% of the adequate Mn intake value. Neither groups exceeded the tolerable upper Mn intake level.
Manganese intake from food groups and its food source
Our subject's daily Mn intakes separated by food groups are shown in Table 3. Food groups that provided a high Mn intake were cereals (2,181.3 µg), vegetables (901.8 µg), seasonings (381.6 µg), pulses (330.2 µg), fruits (104.2 µg), and fish and shellfish (102.1 µg). The Mn intake derived from cereals was significantly higher in boys than it was for girls (P < 0.001). As listed in Table 4, the food item that contributed the most to daily Mn intake was rice (39.8%). The food sources that provided the most Mn, in descending order, were rice, soybean curd, kimchi, black rice, and cereals. There was little sex difference in the food sources from which our subjects derived Mn, with rice, soybean curd, kimchi, cereals and black rice being the most significant items for boys and rice, kimchi, soybean curd, black rice and red pepper powder being the richest Mn sources for girls.
Discussion
Twenty-five to forty percent of the body's Mn content is found in bones, with the remaining Mn being found in the liver, pancreas, and kidney. Mn is a component of arginase, pyruvate carboxylase, Mn superoxide dismutase (MnSOD) and galactosyltransferase. There are Mn metalloenzymes that activate glutamine synthetase, phosphatase, glycosyltransferase, kinase and decarboxylase [15]. By composing or activating these enzymes, Mn plays a key role in the synthesis of carbohydrates, fats, the protein metabolism and glycoproteins. It is also involved in immunity, glucose regulation, energy metabolism in cells, reproduction, and bone growth. Mn is also important in the body's defense against free radicals through controlling the synthesis of DNA, RNA and mucopolysaccharides.
Currently, there is insufficient data about the distribution of Mn intake in Koreans, due to the lack of a complete database displaying the Mn content in foods. After analyzing the National Health and Nutrition Examination Survey, using a database of the Mn contents of 101 different foods, the Korean average Mn intake was found to be 3.8 mg/day. Cereals contributed the most to this (57.3%), followed by vegetables (20.1%), soybean curd (6.1%) and seasonings (5.9%) [16]. Specifically, rice supplied 1,952 µg (51.6% of the total) followed by kimchi (0.213 µg), soybean curd (0.149 µg) and persimmon (0.144 µg). Kim and colleagues [8] studied the Mn intake of 354 Korean adults above the age of 20 using the same database and reported an average Mn intake of 4.54 mg/day (140.9% of the adequate intake) and 2.934 mg per 1,000 kcal of consumed energy. In our study, the Mn intake of children was found to be 4.295 mg/day, which is similar to the Mn intake found for adults [8]. However, the Mn intake amount per 1,000 kcal was 2.011 mg, which represents a lower Mn density diet compared to that of adults. The key Mn-providing food sources for children were found to be similar to those for adults, and include cereals (50.8%), vegetables (21.0%), seasonings (8.9%) and pulses (7.7%).
In a previous study of 94 Japan children between 3 and 5 years of age, Mn intake was reported to be 1.3 mg/day [17]. A report by Aung et al. [9] also showed that in 25 children aged between 3 and 6, the daily Mn intake was 1.56 mg/day, which is close to the recommended value. Comparing these prior results with the current study, even though the Mn intake databases used for the analyses were not the same, it can nevertheless be proposed that Korean children consume higher amounts of Mn than their peers in other coutnries. This higher Mn intake may be due to the fact that the Korean diet traditionally contains more Mn rich foods such as rice, cereals and pulses.
Mn intake is also drastically different between populations due to varying dietary patterns. Frequent tea drinkers and vegetarians have a higher Mn intake rate. The daily Mn consumption for an omnivorous child was shown to range from 1.5 mg per day to as much as 3.6 mg per day, whereas for vegetarian this was shown to range from 2.7 mg per day to as much as 4.3 mg per day [18].
According to a study by Kim and Sung [19], postmenopausal vegetarian women had a 4.2 mg/day Mn intake, significantly higher than that for omnivores, whose Mn intake was 3.4 mg/day. In this study, for both vegetarians and omnivores, cereals, pulses, vegetables and seasonings were found to be the main sources of dietary Mn [19]. Choi examined the Mn contents of the 30 most common foods, then analyzed this data in conjunction with the National Health and Nutrition Examination Survey and reported an average daily Mn intake of 3.4 mg/day [20]. The foods which most contributed to Mn intake were rice, kimchi, soybean curd, radish, Korean Chinese cabbage, soybean sprout and bread, ranked in descending order [20]. In this study, most dietary Mn came from rice, soybean curd and kimchi (52.0% of total Mn intake). In our study, we found that black rice, cereals, red pepper powder, and soy sauce all contributed to Mn intake, which differed from the results in Choi [20]. Interestingly, 78.5% of the dietary Mn consumed by boys came from the 20 main food sources, which was lower than the figure for girls of 83.5%. Given this finding, we concluded that boys derived their dietary Mn from more varied food sources than girls.
There were some limitations to our research. First, because our study was performed over summer months, seasonal variations in Mn intake could not be reflected. Second, our subjects' daily energy consumption was 2,142.4 kcal, which was higher than those of the KNHANES subjects aged 6-11 years (1,632.3 kcal) and the EER (estimated energy requirement) for 9-11 year olds (boys; 1,900 kcal, girls; 1,700 kcal) and for 12-13 year olds (boys; 2,400 kcal, girls; 2,000 kcal) [14,21]. Therefore, the Mn intake in our study might have been over-estimated. Yet, considering that our research is the first to estimate the Mn intake of Korean children, we believed that our study result may nevertheless help in systematic follow-up studies of childhood Mn intake.
To conclude our findings, it can be proposed that Korean children receive a sufficient Mn intake from their daily diet and do not exceed the upper intake level. The main food sources of Mn for children aged 11-12 were found to be rice, soybean curd, kimchi, black rice, and cereals, in descending order. The results of our study may be used as a basis for the development of follow-up studies addressing Mn intake in children.



 XML Download
XML Download