

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
A number of studies have assessed the diets of individuals and populations in terms of single foods, food groups, nutrients, or other individual dietary components. An alternative approach is to examine overall diet quality in order to reflect the complexity of food intake patterns and dietary exposure [1]. The assessment of diet quality in a population is important in policy-making, monitoring service outcomes, and designing research interventions [2]. The Healthy Eating Index (HEI) was developed by the US Department of Agriculture (USDA) "to provide a single summary of diet quality based on different aspects of a healthy diet" [3]. The HEI-2005 is a valid measure of diet quality and has various potential purposes. It is used for epidemiological research to monitor a population's diet and evaluate nutrition interventions. The HEI-2005 assesses dietary intakes on a per calorie basis rather than on the basis of absolute amounts of foods consumed; thus, the HEI-2005 assesses the quality of the relative proportions of foods consumed rather than the quantity of foods consumed [4].
In recent years, epidemiological studies on diet and chronic diseases have tended to focus on the relationship between diet quality and disease risk in different age groups, including children, adolescents, adults, and elderly people [2,5-7]. Most of these studies performed on adolescents determined diet quality and the relationship between diet quality and health outcomes [8-10]. The HEI is a useful index in assessing diet quality, and it has been used to successfully monitor the diet in adolescents [8,10]. Adolescence, the transition from childhood to adulthood, is one of the most dynamic periods of human development [11]. Physiological and social conditions affect adolescents' dietary patterns. Physiologically, energy and nutrient requirements rise due to increasing body size and sexual maturation, including menarche in girls. Socially, adolescence affords an opportunity for food selection independent of parental guidance. Consequently, adolescents may tend to acquire unhealthy eating behaviours such as skipping meals, under-eating, or over-eating, all of which decrease diet quality [12]. However, according to our knowledge, no study has been specifically performed to determine the diet quality in Turkish adolescents.
The aim of this study was to use the HEI-2005 to assess diet quality and determine the relationship between the HEI-2005 and energy and nutrient intakes of adolescents.
Subjects and Methods
Participants and study area
A cross-sectional study was conducted on a total of 1,104 adolescents (469 girls and 635 boys) aged 14 to 18 years (mean ± SD, 15.8 ± 1.24 years old). Subjects were randomly selected from healthy adolescent primary school children living in Ankara, which is the capital city and the heart of the Anatolian Plateau in west central Turkey. Inclusion of the subjects was on a voluntary basis; prior to acceptance, children's parents or caregivers were fully informed about the objectives and methods of the study. Adolescents and their parents signed an informed consent and filled in the questionnaires, which adhered to Declaration of Helsinki protocols (World Medical Association). Data were collected in face-to-face interviews from March 2009 to September 2010.
Measurements
All measurements were taken by trained dieticians and with participants wearing light clothes and no shoes. A portable scale was used to measure body weight to the nearest half-kilogram. Height was measured to the nearest 0.1 cm with a stadiometer. Waist circumference (WC) was measured at the mid-point, above the iliac crest and below the lowest rib margin at minimum respiration, using a flexible tape [13]. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2).
Instrument
Food consumption was measured using the 24-hour dietary recall (24HR) method. Series of photographs of foods usually consumed in Turkey were shown to adolescents in order to estimate portion size while keeping the food record [14]. Energy and nutrient intake was calculated using the Nutrition Information System (BeBiS) program [15]. All food groups along with energy and nutrients intakes were created from dietary records using this program.
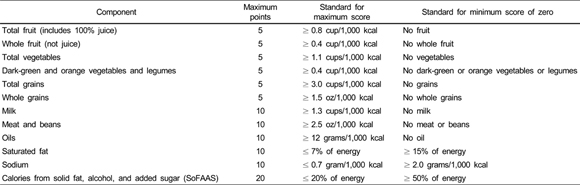
The Healthy Eating Index (HEI) is a measure of diet quality that assesses conformance to Federal dietary guidance. The original HEI was created by the US Department of Agriculture (USDA) in 1995. The USDA's HEI was recently revised to reflect the 2005 Dietary Guidelines, and a new scoring system was developed [3]. The HEI-2005 comprises 12 components, which are scored on a scale from 0 to M, where M is 5, 10, or 20 according to the component. Each component is expressed as a ratio of an individual's intake of a specific food or nutrient to their intake of energy, before scoring [10,16].
The total HEİ-2005 score was calculated in three steps:
1) For each individual, calculate each HEI-2005 component score on the basis of his/her 24-HR. Then, for each component score and for the total score, take the (arithmetic) mean over the individuals which is called the mean score. The HEI-2005 total score is calculated as the sum of these scores over the 12 components.
2) For each individual and each component, calculate the ratio of the reported intake of food group or nutrient (relevant to the HEI component considered) to the reported energy intake. Then, take the mean of these ratios over the individuals. Finally, calculate the HEI-2005 component score based on this mean ratio. We call this the score of the mean ratio. The HEI-2005 total score is calculated as the sum of these scores over the 12 components.
3) Calculate the population's total intake of food group or nutrient (relevant to the HEI component considered) and total energy intake, and take the ratio of these. Then, calculate the HEI-2005 component score based on this ratio of the totals. We call this the score of the population ratio. The HEI-2005 total score is calculated as the sum of these scores over the 12 components [16].
Possible scores range from 0 to 100, with 100 points referring to perfect diet quality and lower results indicating larger deviations from the recommended intakes. Participants' diets can be categorized as "poor" (≤50), "needs improvement" (from 51 to 80), and "good" (> 80) score [10,17]. (Appendix 1).
Statistical analysis
The data analyses were carried out using SPSS version 13.0 software (SPSS Inc., Chicago, IL, USA). The descriptive statistics of means with 95% CI were used to summarize the data collected. All values are reported as the mean (χ̅) ± standard deviation (SD). The relations between HEI scores and educational status, meals, and snack numbers were investigated with an age- and gender-adjusted linear regression model. The Kolmogorov-Smirnov test was used to determine whether or not outcome variables were normally distributed. To compare normally distributed data, the t-test was used. Mann Whitney U test was used for non-normally distributed data. In all analyses, 5% and 1% significance levels were used. The Pearson Correlation test was used to determine the relationship between HEI-2005 and nutrient intakes.
Results
The education status of the adolescents' parents was classified as low (less than 8 years) or high (more than 8 years); 66.7% had a mother and 51.0% had a father with a low education level. In total, 74.4% of adolescents reported that they consumed 3 meals per day, and 74.7% had one to four snacks per day. When age and gender were adjusted, associations between HEI-2005 scores and parental education level were found to be significant (P < 0.05), whereas associations between HEI-2005 scores and numbers of meals and snacks were not found to be statistically significant (P > 0.05). HEI-2005 scores increased linearly as the mother's and father's education level increased (P < 0.01) (Table 1).
The HEI-2005 scores for 42.8% of adolescents were classified as "poor diet" and 57.2% were "needs improvement". According to the HEI-2005 scores, no subjects were classified as having a "good diet". No differences in the HEI-2005 scores were observed according to age or anthropometric measurements (body weight, height, waist circumference, and BMI) (P > 0.05) (Table 2).
Protein and dietary fibre intake and the percentage of total energy from protein and carbohydrates were significantly greater in the "needs improvement" group compared with the "poor diet" group adolescents (P < 0.01). Dietary fat intake and the percentage of total energy from fat were significantly high in the "poor diet" group. No differences in the HEI-2005 classification groups were observed for daily total grains, saturated fat, and energy intakes. The average intake of the other components was significantly greater in the "needs improvement" group compared with the "poor diet" group of adolescents, except for oil, saturated fat, sodium, energy from solid fat, alcohol and added sugar (SoFAAS), and energy (P < 0.01) (Table 2).
HEI-2005 scores were evaluated per person. The mean total HEI-2005 score was 51.5 ± 9.07 (χ̅Boys: 51.2 ± 9.26 and χ̅Girl: 51.8 ± 8.92). The gender difference in HEI-2005 scores was not significant in this respect (P > 0.05). The total fruit, whole fruit, total vegetables, dark green and orange vegetables, and legumes component scores were significantly high in girls (P < 0.01). Furthermore, the meat and beans, oil, and sodium components scores were significantly high in boys (P < 0.01) (Table 3). [Ed: not sure which items are together here. Please check comma usage]
HEI-2005 was found to correlate significantly with age as well as total energy, protein, fat, and dietary fibre intakes (P < 0.05) (Table 4). There were negative correlations between HEI-2005 scores and age, total energy intake, and fat intake (r = -0.073, P= 0.015; r = -0.088, P= 0.003; r = -0.170, P= 0.000, respectively); positive correlations were only determined between HEI-2005 scores and protein and dietary fibre intakes (r = 0.064, P = 0.035; r = 0.112, P = 0.000, respectively). There were no correlations observed between HEI-2005 scores and the anthropometric measurements (P > 0.05).
Discussion
Healthy eating habits may help adolescents achieve their full growth potential and may provide beneficial health effects throughout life. However, many adolescents do not adopt healthy eating habits due to complex and different factors. Friends, advertising, and promotion of commercial products such as soft drinks, sugary and salty foods, chips, and fast foods all affect negatively the eating habits of adolescents [12]. On the other hand, as providers, models, and regulators, parents try to reduce the negative effects of these factors by imbuing healthy eating habits in their children [18]. In this study, adolescents' total HEI-2005 scores increased in parallel with parental education level, and their relationship was found to be statistically significant when age- and gender-adjusted. Similarly, the enKid Study reported that a low parental educational level is significantly associated with poor nutrition [19]. Nutritional education should be focused on the whole family in order to improve the diet quality of adolescents.
Meal skipping is another factor associated with low diet quality that is commonly used by adolescents trying to control their weight. Woodruff et al. [20] indicated that participants who skip breakfast are likely to have worse diet quality than those who regularly consume meals. In the present study, the majority of adolescents (74.4%) regularly consumed 3 main meals per day (breakfast, lunch, and dinner) as well as one to four snacks per day (74.7%). However, 25.6% of adolescents skipped main meals, which reduced their total HEI-2005 scores, although not significantly. Adolescent eating behaviours that involve nutritional risk may emerge, including skipping meals, especially breakfast; inappropriate eating between meals (over-consumption of cookies, candies, chewing gum, snacks, and soft drinks); increasing intake of added sugars and saturated fats; and low consumption of fruits and vegetables, reducing the intake of micronutrients [21]. Unhealthy adolescent dietary practices not only have immediate deleterious physical and psychological effects, but they can also determine the trajectories of eating habits that influence chronic disease risks throughout adulthood, such as obesity and cardiovascular disease [22].
Contradictory relations between HEI and BMI have been reported by several studies [2,4,8,20]. Studies have reported that there is no relationship between total HEI score and body weight [17,10] or BMI [21] in adolescents. Similarly, in the present study, total HEI scores did not correlate with body weight, height, waist circumference, or BMI (P > 0.05). However, Feskanich et al. [8] reported a weak unadjusted association between a dietary index and BMI in children and adolescents. These inconsistencies among studies have been attributed to variations in the age of the populations studied, study protocols, dietary assessment methods, composition, and range of dietary index [23].
Studies conducted on adolescents' diet quality have indicated that total HEI scores are at the "poor" and "need improvement" levels [24-26]. According to the HEI scores, 74.4% of adolescents' [21] and 84.5% of schoolchildrens' [24] mean scores were found to be between 51-80, which means "needs improvement", and only 2.9% and 3.5% of them, respectively, had a good diet. Goodwin et al. [25] reported that the overall quality of dietary intake of adolescents is poor based on their HEI scores. In another study among adolescents, 13% had HEI scores < 51 "poor", one third had scores < 60, indicating a diet that "needs improvement," and only 15% had HEI scores > 80, indicating "good" diet quality [22]. In the present study, diet quality scores ranged between 23.7 and 77.5, whereas the mean score was found to be approximately 51.5 ± 9.07 according to HEI-2005. Adolescents had a poor diet (42.8%) or a diet that needs improvement (57.2%). There were no subjects with a "good diet". Therefore, the overall diet quality of adolescents needs modification.
Lower mean subgroup scores were found for whole grains, total vegetables, total fruits, dairy products, and meat and beans. Grain is a staple food of the Turkish people. A major percentage of energy comes from bread and other cereals (58%), and grain is mainly consumed as bread, macaroni rice, and bulgur (cracked wheat), which is a cereal and crushed wheat grain [27]. In this study, the total grain subscore was found to be high while the whole grain subscore was found to be low, and there was no significant difference between genders. Taste, texture, appearance, and availability were factors that may have prevented the consumption of whole grains, whereas grain consumption was very high in adolescents. "Healthy People 2001" includes the objective to "increase the proportion of persons aged two and older who consume at least six daily servings of grain products, with at least three being whole grains" [28]. Whole grain consumption in the recommended amounts prevents chronic disease and helps maintain a healthy weight. Diet quality and nutrient intake can be significantly improved by increasing the consumption of the whole grain subgroup of HEI-2005 [29]. However, consumption of whole grains in children and adolescents remains generally low [29,30]. In the present study, the impact of whole grain subgroup may have been small due to low consumption. Intakes of many macro- and micronutrients such as fibre, magnesium, vitamin E, calcium, and potassium also can be improved with increased consumption of whole grains. Whole grain consumption should be encouraged for children, adolescents, and their parents by health professionals, especially dietitians [29]. To improve the availability of whole grain breads and other products at home, parents should be provided with information to help them identify and prepare whole grain products [31].
Generally, the typical adolescent diet is poor in overall quality due to high intake of fat, saturated fat, and sugar and low intake of dairy products, fruits, and vegetables [25, 26]. In this study, adolescents consumed less than five servings of fruits and vegetables per day. Especially, total fruit and total vegetable subscores of the HEI-2005 were lower in boys than in girls. These findings were similar to previous research in Turkey [32,33] and other countries [34,35], which found that fruit and vegetable intakes among adolescents were lower than recommended levels. The World Health Organization (WHO) recommends a minimum daily intake of 400 g of fruits and vegetables [21]. Although our country is rich in fruits and vegetables and these are moderately priced, consumption of them is under the recommended level. This is mainly because fast foods with high carbohydrate and fat contents are preferred by adolescents. To promote fruit and vegetable consumption, national campaigns like the "5 A Day Program" should be conducted in Turkey.
Although meat is one of the main ingredients of Turkish cuisine, population-based studies have shown that consumption of meat is lower than the recommended level in Turkey [36]. In the present study, the total mean score for meat was found to be low, and also the scores based on HEI-2005 were determined to differ significantly according to gender, being higher in boys. Dwyer et al. [37] found that boys have significantly higher subscores for meat than girls, although there was no significant difference according to gender. In this study, the results indicate that Turkish adolescents consume meat, meat products, and beans at levels lower than the daily recommended levels, which could be one of the main reasons for the iron deficiency anaemia seen frequently among adolescents in Turkey (approximately 30%) [27,38].
Trends in beverage consumption over the past several decades suggest that the overall nutrition profile of adolescents is changing. Total energy intake from beverages is increasing in adolescents [39]. Inadequate intake of dairy products in adolescents was also seen in this study. The milk subscore was relatively low and did not differ according to gender. The same result was reported by De Andrade et al. [21] and Troiano et al. [40]. As a consequence of increasing consumption of soft drinks, milk intake has dramatically decreased among adolescents. Milk is crucial for increased bone mineral density during the periods of peak bone mass development in adolescence and for reducing the risk of osteoporosis in later life [21]. Overall diet quality in adolescents may be compromised by changing beverage trends, with less nutritious beverages replacing micronutrient dense drinks, including milk [41].
The HEI-2005 subscore for energy from solid fat, alcohol, and added sugar (SoFAAS) was found to be remarkably high in both genders. A higher mean SoFAAS reflects lower intakes of saturated fat, trans-fat, alcoholic beverages, and added sugar. Therefore, diet quality is significantly improved with a high SoFAAS subcore in the HEI-2005. The reason for the increase in SoFAAS subscore is especially related to low alcohol consumption, but another possible reason may be misreporting of consumption of SoFAAS and dietary recall bias of adolescents by this age group in Turkey.
The HEI-2005 was found to correlate with age as well as protein, dietary fibre, fat, and total energy intakes. Age displayed an inverse association with the HEI-2005 score, indicating that dietary quality significantly decreases with adolescents' age, which was corroborated by De Andrade [21]. Significant positive correlations between HEI-2005 and total energy [8,10] and fibre intakes [10] were observed. In this study, it was determined that the HEI-2005 scores positively correlated with protein and dietary fibre intakes and negatively with fat and total energy intakes. The group with HEI-2005 scores from 51 to 80, which means "needs improvement", consumed higher protein, carbohydrate, and dietary fibre contents than the "poor diet" group. On the other hand, fat intake was significantly high in the "poor diet" group (P < 0.01) (Table 2). HEI-2005 component scores are based on ratios of reported intakes of food groups or nutrients to that of total energy. SoFAAS and saturated fat intake increased energy consumption. However, low saturated fat, SoFAAS, and sodium intakes also increased the total HEI 2005 score. Total HEI-2005 score increased with higher consumption of whole grains, fruits, and vegetables, which are rich in fibre, and whole grains, milk, and meat and beans, which are rich in protein. In this study because of inadequate consumption of whole grains, fruits, vegetables, milk, and meat subgroups total score was decreased. The high energy intake of adolescents was related to a low HEİ-2005 score, which puts them at higher risk of obesity and other chronic diseases [22]. On the other hand, negative or positive correlation between energy intake and HEI scores can be attributed to the use of different diet quality assessment methods, mainly the original HEI and HEI-2005, which are composed of different subgroup ratios [16]. The limitation of this study was that it assessed food intake by only the 24-hour recall method. Dietary intake may vary from day to day, and a 24-hour recall assessment may not reflect an individual's habitual intake. Therefore, the results obtained cannot be generalized for the whole adolescent population in Turkey. However, they emphasize the importance of providing data for further research. Further research is needed to determine the relationship between diet quality and health outcomes of adolescents and different age groups.
This study indicated that according to the HEI-2005 assessment, the diet quality of the majority of adolescents needs to be improved. Methods are needed to improve the nutritional habits of adolescents. For this purpose, measures in the family, preschool, school, and adulthood, covering the period of training programs, should be initiated by the government via advertisements and campaigns. Especially, schools can create environments that promote healthy eating. School-based interventions that also involve families and communities are needed to help improve diet quality to prevent or reduce risk factors for diet-related chronic diseases.



 XML Download
XML Download